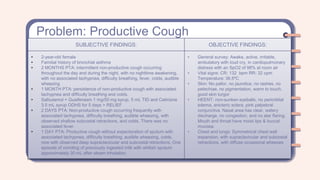
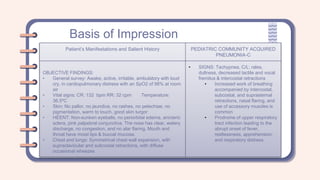
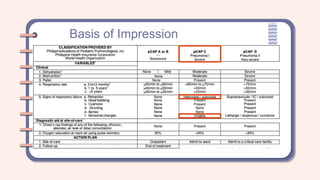
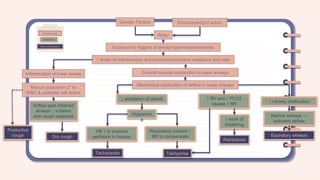
A 2-year-old female presented with a productive cough that had progressed over two months. She had a family history of asthma. On examination, she was tachycardic, tachypneic, and had supraclavicular and subcostal retractions with diffuse wheezing. Based on her history of recurrent cough and family history of asthma, as well as her physical exam findings, she was assessed as having a bronchial asthma exacerbation. Differential diagnoses considered included community-acquired pneumonia and bronchiolitis.