• Exacerbations ofasthma are episodes which are characterized by a
progressive increase in symptoms of shortness of breath, cough,
wheezing or chest tightness and progressive decrease in lung
function i.e they represent a change from the patients usual status
that sufficient to require change in treatment.
4.
• In additionto factors known to increase the risk of asthma exacerbations some
features are specifically associated with an increase in the risk of asthma-related
death.
FACTORS THAT INCREASE ASTHMA RELATED DEATHS:-
• A history of near-fatal asthma requiring intubation and mechanical ventilation.
• Hospitalization or emergency care visit for asthma in the past year.
• Currently using or having recently stopped using oral corticosteroids (a marker
of event severity).
• Not currently using inhaled corticosteroids.
• Over-use of SABAs, especially use of more than one canister of salbutamol (or
equivalent) monthly.
• A history of psychiatric disease or psychosocial problems.
• Poor adherence with asthma medications and/or poor adherence with (or lack
of) a written asthma action plan.
• Food allergy in a patient with asthma.
5.
DIAGNOSIS OF ACUTEEXACERBATION
• The decrease in expiratory airflow can be quantified by
lung function measurements such as peak expiratory flow
(PEF) or forced expiratory volume in 1 second (FEV1),
compared with the patient’s previous lung predicted values.
• In the acute setting, these measurements are more reliable
indicators of the severity of the exacerbation than
symptoms.
• The frequency of symptoms may, however, be a more
sensitive measure of the onset of an exacerbation than pef.
7.
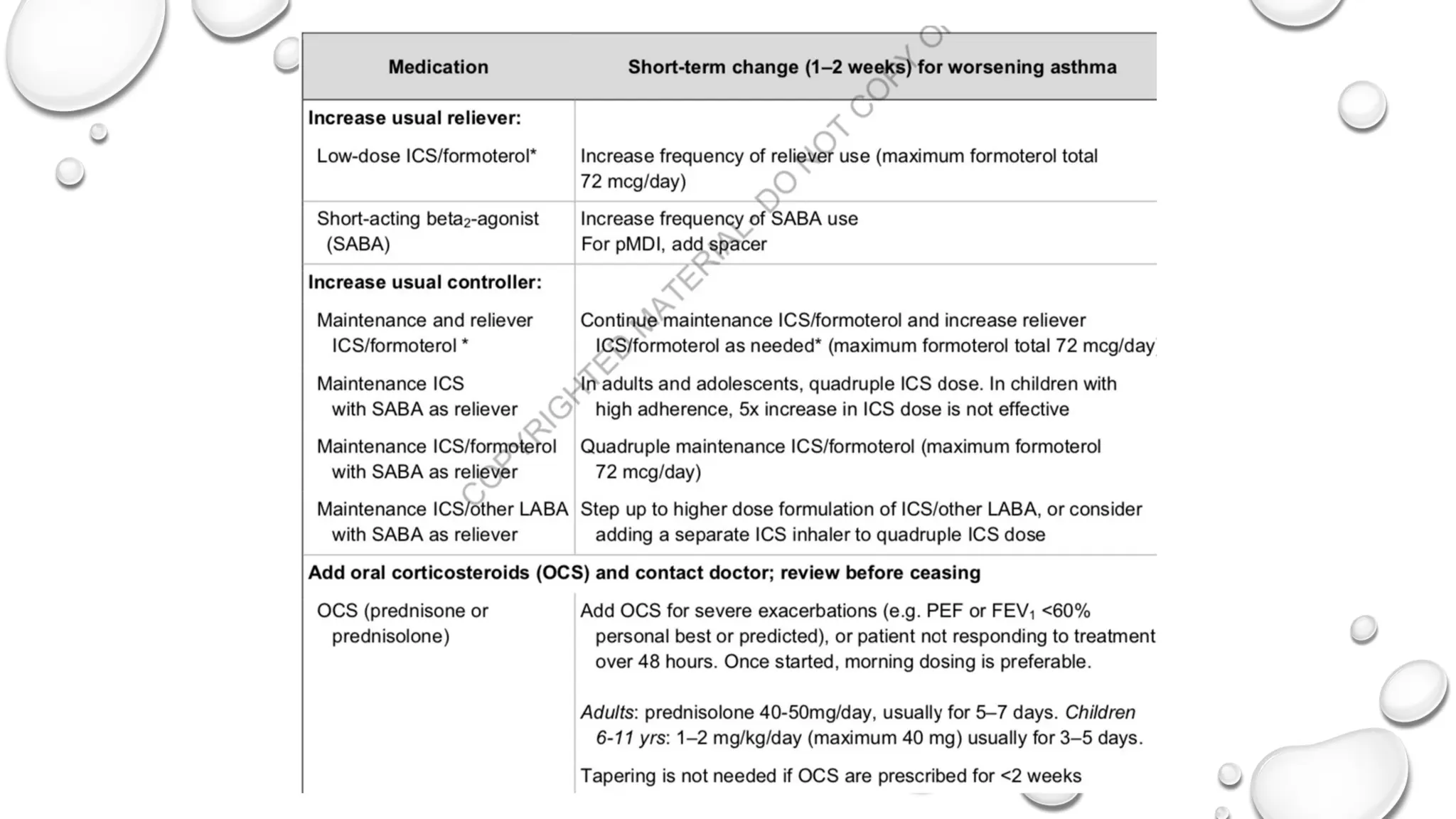
All patients shouldbe provided with a written asthma action plan
appropriate for their level of asthma control and health literacy,
so they know how to recognize and respond to worsening asthma.
The action plan should include when and how to change reliever
and controller medications, use oral corticosteroids, and access
medical care if symptoms fail to respond to treatment.
Patients who deteriorate quickly should be advised to go to an
acute care facility or see their doctor immediately.
10.
Follow up afterself managed acute
exacerbations
• Patients should see their primary care health care provider for a semi-urgent review
(e.g. Within 1–2 weeks), for assessment of symptom control and additional risk
factors for exacerbations ,and to identify the potential cause of the exacerbation.
• The written asthma action plan should be reviewed to see if it met the patient’s
needs.
• Maintenance controller treatment can generally be resumed at previous levels 2–4
weeks after the exacerbation, unless the history suggests that the exacerbation
occurred on a background of long-term poorly controlled asthma.
• In this situation, provided inhaler technique and adherence have been checked
• (Step up in treatment may be required).
11.
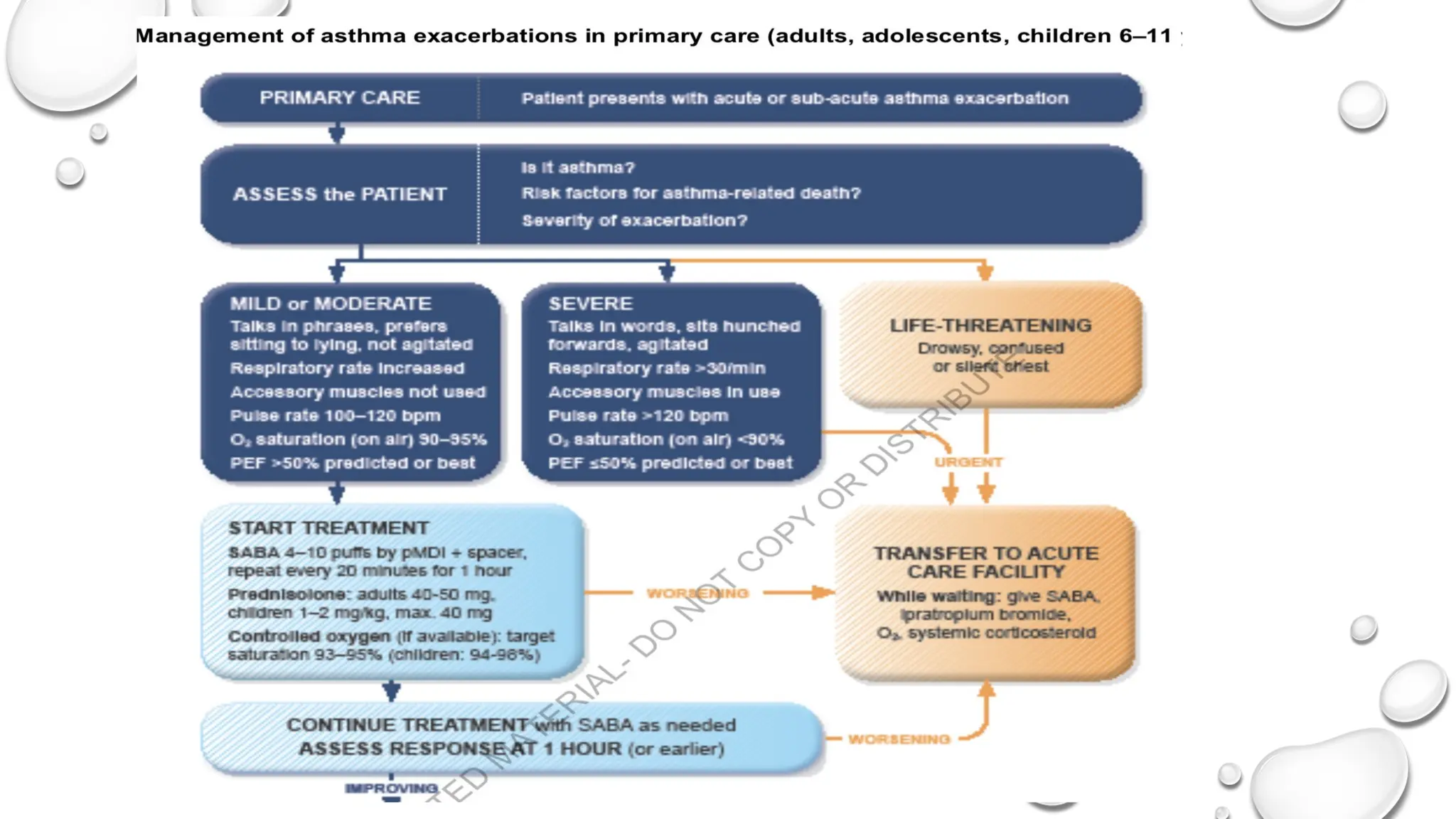
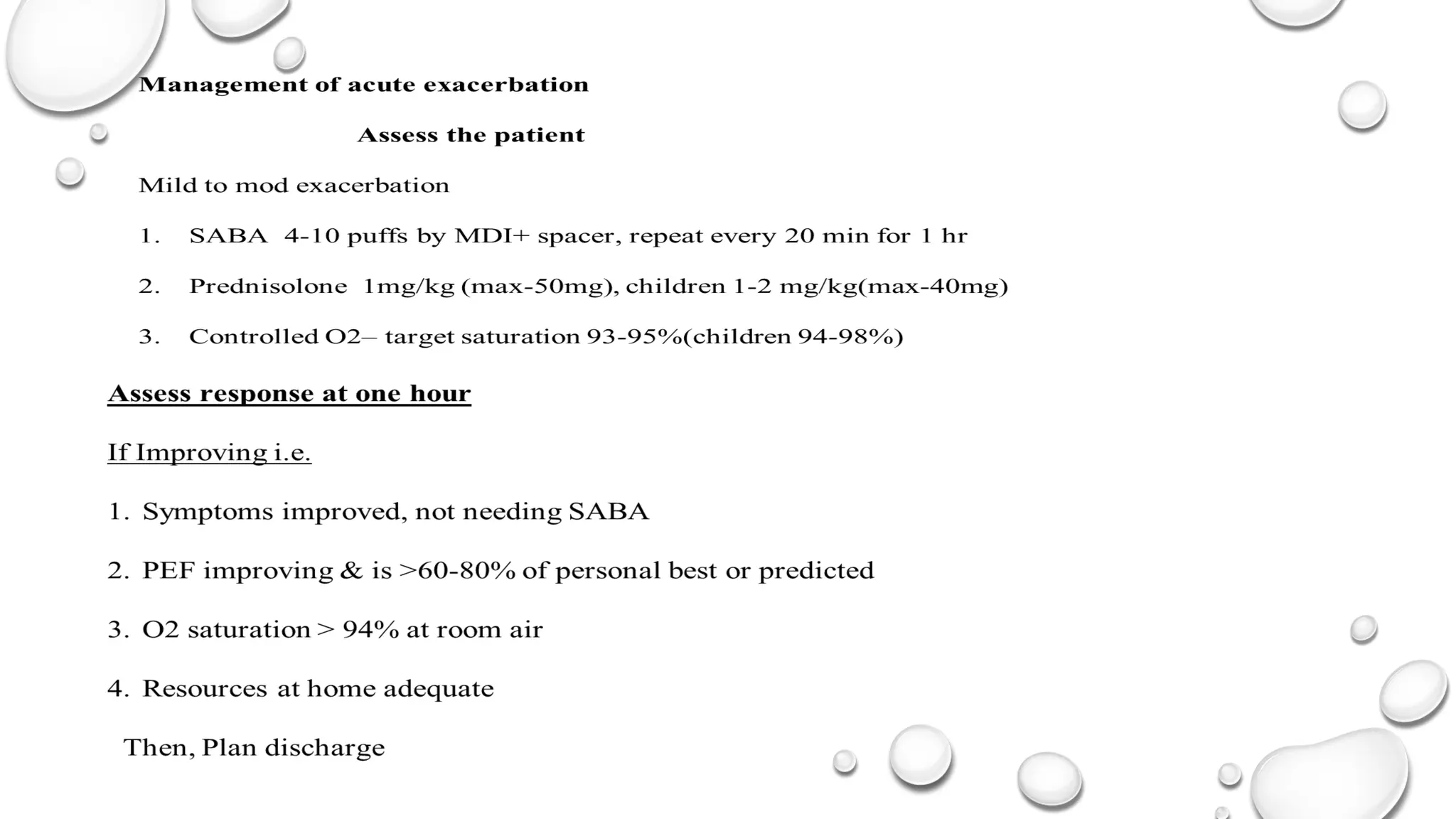
Main initial therapiesemployed at primary care setting include :
Repetitive administration of short-acting inhaled bronchodilators,
early introduction of systemic corticosteroids, and controlled flow oxygen supplementation.
The aim is to rapidly relieve airflow obstruction and hypoxemia, address the underlying inflammatory pathophysiology,
and prevent relapse
Brief focused history and relevant physical examination should be conducted concurrently with the prompt initiation of
therapy, and findings documented.
If the patient shows signs of a severe or life-threatening exacerbation, treatment with SABA, controlled oxygen and
systemic corticosteroids should be initiated while arranging for the patient’s urgent transfer to an acute care facility.
12.
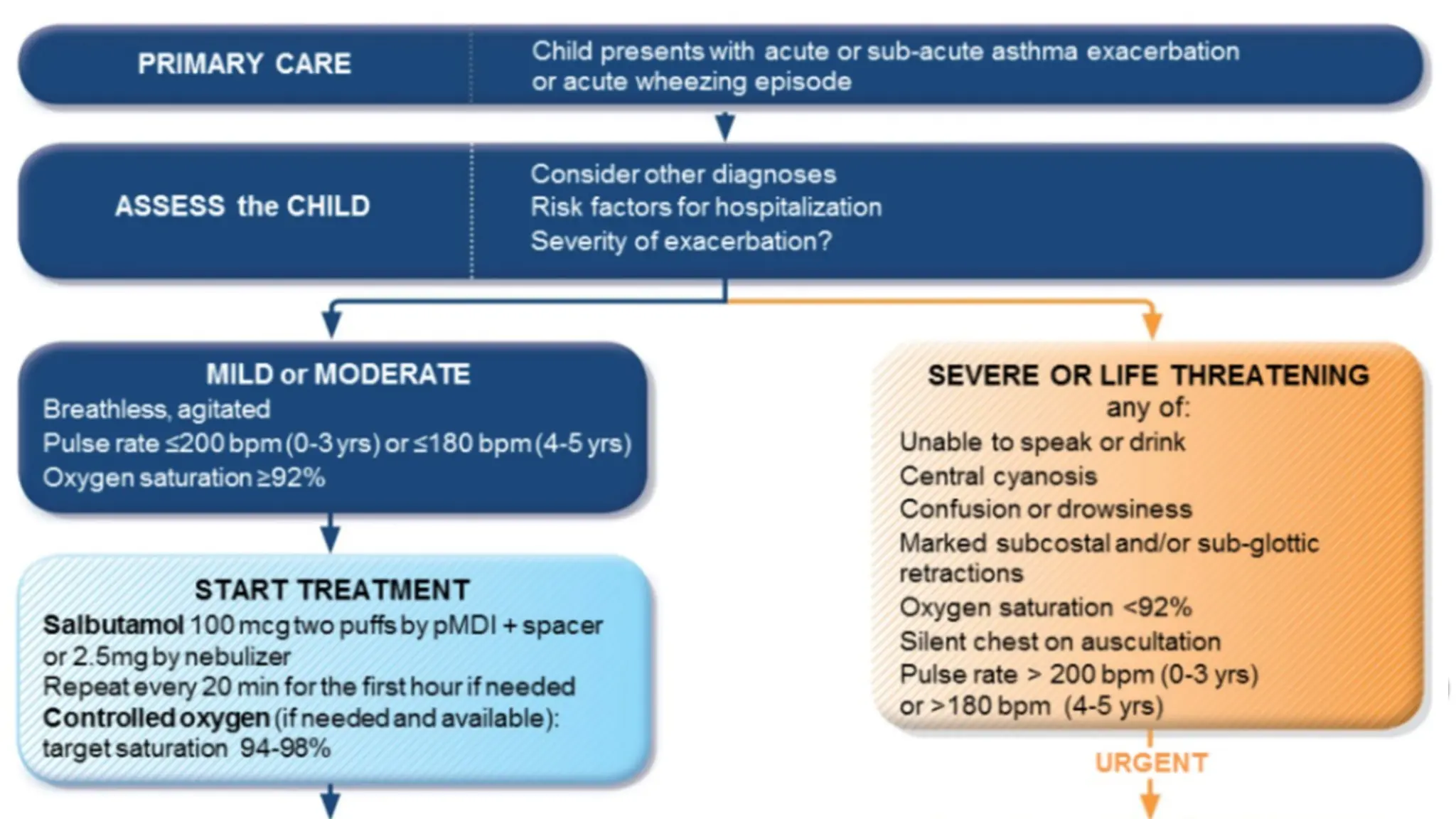
Assessment of Severity
•The severity of exacerbation is assessed by evaluating pulse rate, respiratory
rate, use of accessory muscles and ability to complete a sentence.
Becker asthma score is a quick assessment of severity by using respiratory rate,
wheezing, inspiratory: expiratory ratio and accessory muscle use.
A score >4 is considered moderate status asthmaticus while patient with
Score 7 and above should be admitted to the ICU .
17.
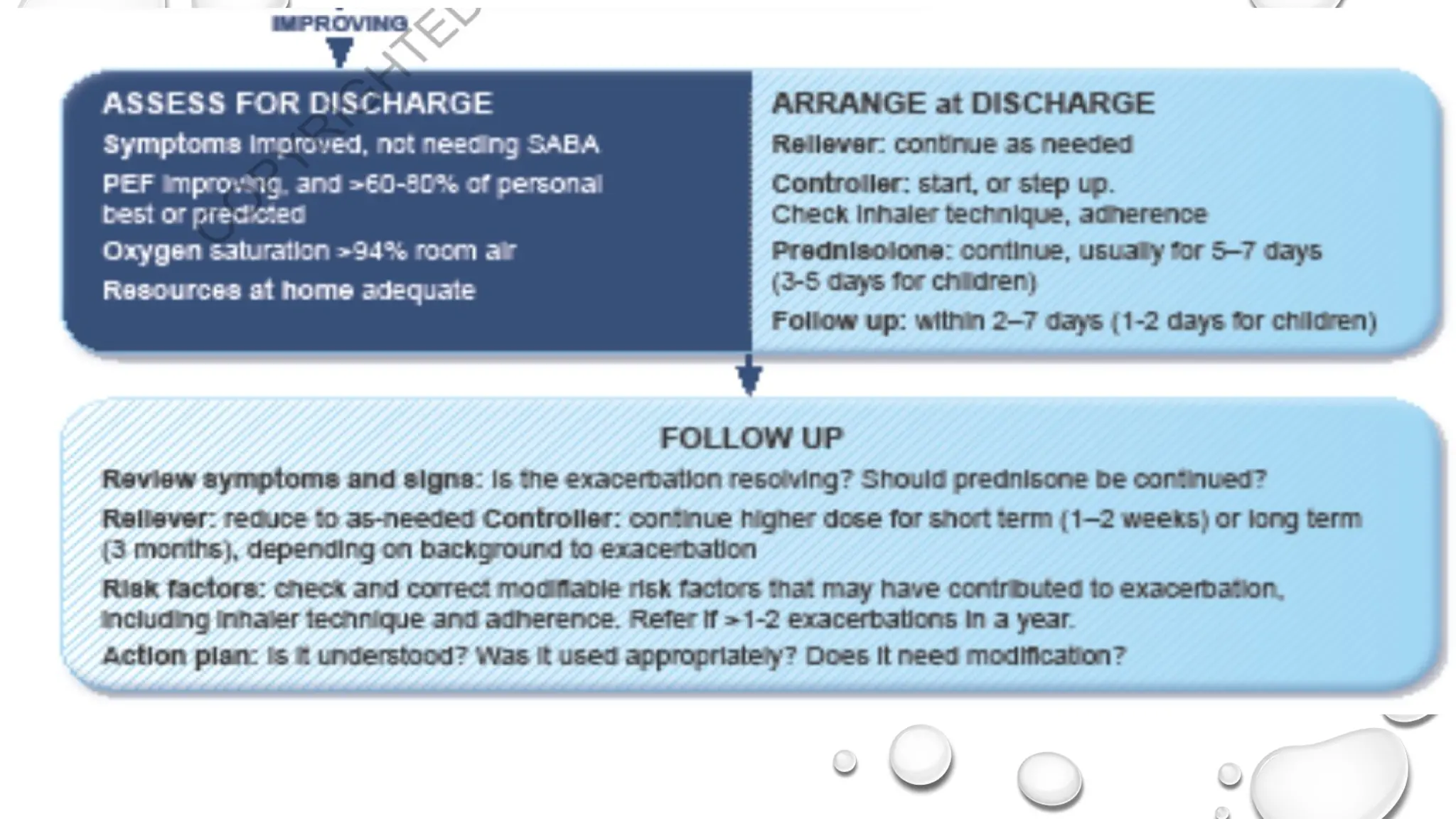
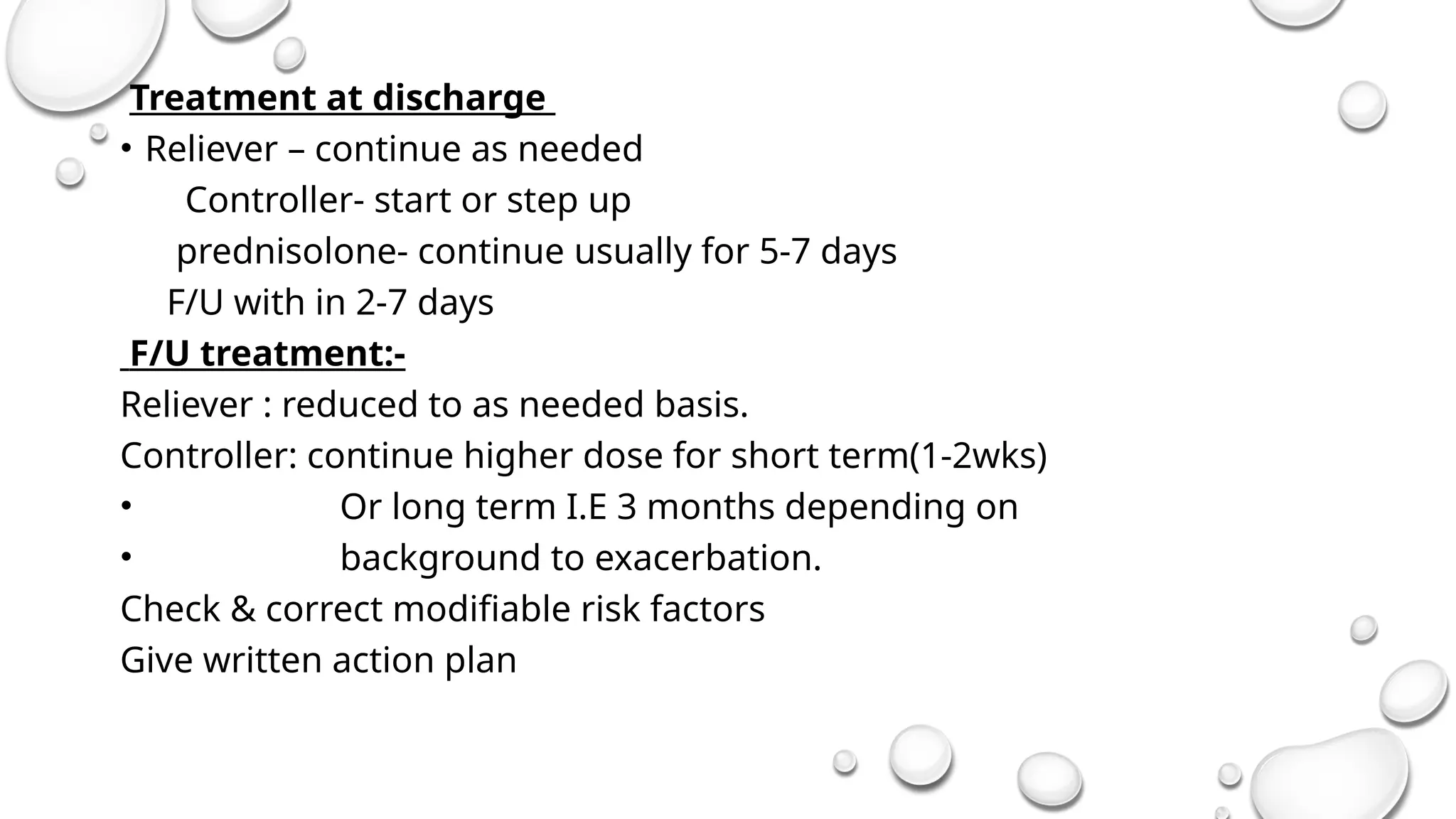
Treatment at discharge
•Reliever – continue as needed
Controller- start or step up
prednisolone- continue usually for 5-7 days
F/U with in 2-7 days
F/U treatment:-
Reliever : reduced to as needed basis.
Controller: continue higher dose for short term(1-2wks)
• Or long term I.E 3 months depending on
• background to exacerbation.
Check & correct modifiable risk factors
Give written action plan
18.
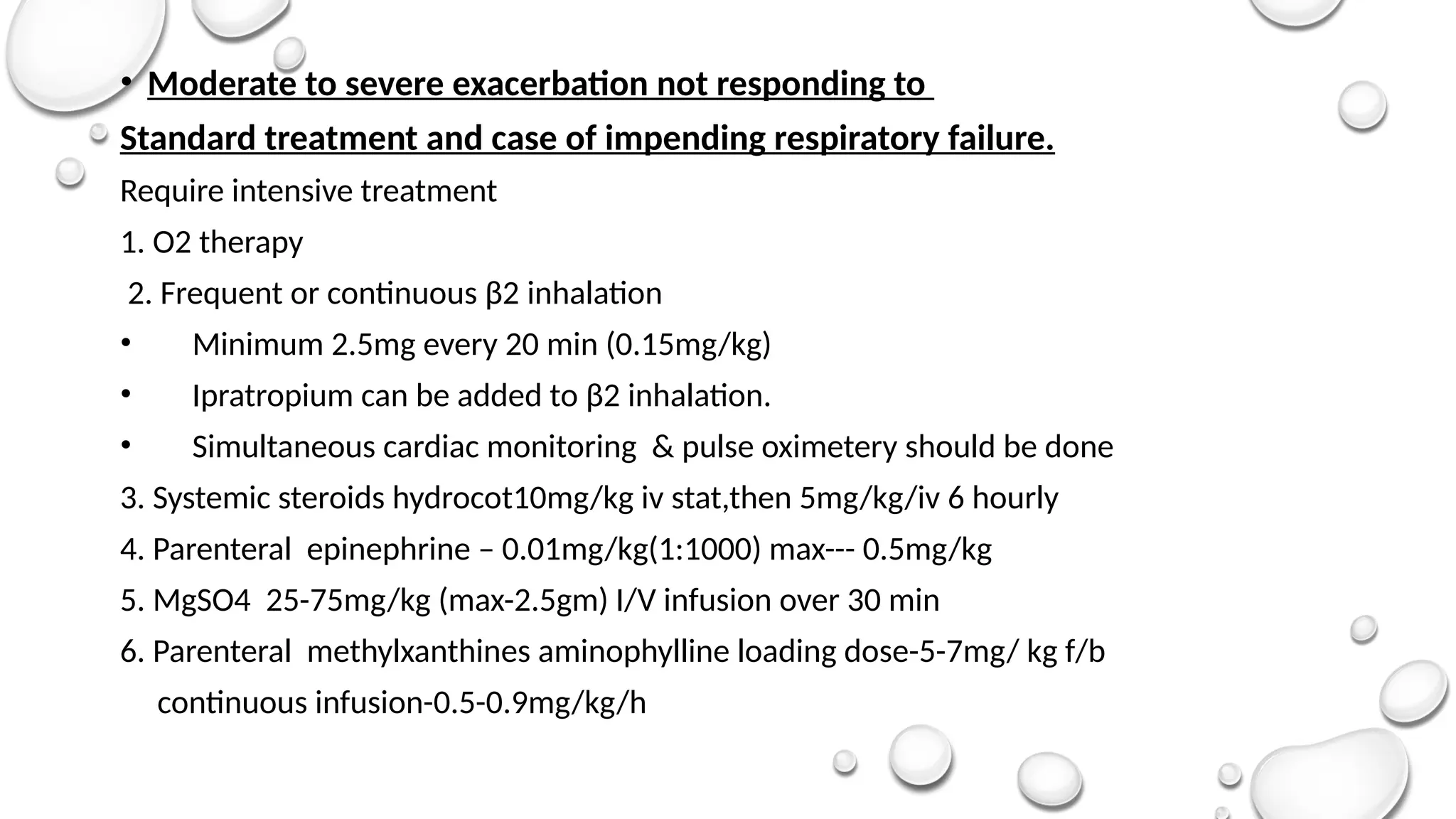
• Moderate tosevere exacerbation not responding to
Standard treatment and case of impending respiratory failure.
Require intensive treatment
1. O2 therapy
2. Frequent or continuous β2 inhalation
• Minimum 2.5mg every 20 min (0.15mg/kg)
• Ipratropium can be added to β2 inhalation.
• Simultaneous cardiac monitoring & pulse oximetery should be done
3. Systemic steroids hydrocot10mg/kg iv stat,then 5mg/kg/iv 6 hourly
4. Parenteral epinephrine – 0.01mg/kg(1:1000) max--- 0.5mg/kg
5. MgSO4 25-75mg/kg (max-2.5gm) I/V infusion over 30 min
6. Parenteral methylxanthines aminophylline loading dose-5-7mg/ kg f/b
continuous infusion-0.5-0.9mg/kg/h
20.
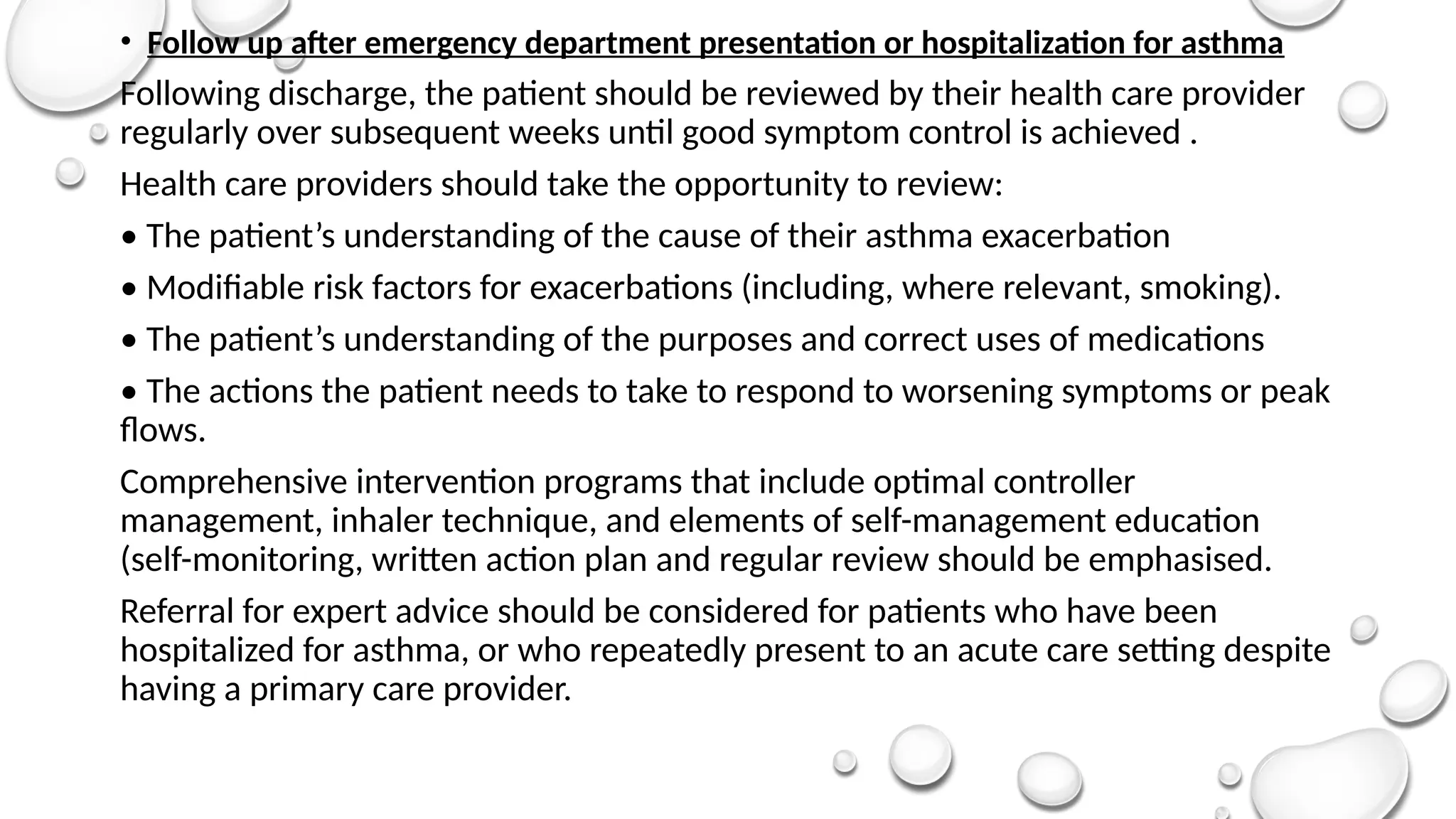
• Follow upafter emergency department presentation or hospitalization for asthma
Following discharge, the patient should be reviewed by their health care provider
regularly over subsequent weeks until good symptom control is achieved .
Health care providers should take the opportunity to review:
• The patient’s understanding of the cause of their asthma exacerbation
• Modifiable risk factors for exacerbations (including, where relevant, smoking).
• The patient’s understanding of the purposes and correct uses of medications
• The actions the patient needs to take to respond to worsening symptoms or peak
flows.
Comprehensive intervention programs that include optimal controller
management, inhaler technique, and elements of self-management education
(self-monitoring, written action plan and regular review should be emphasised.
Referral for expert advice should be considered for patients who have been
hospitalized for asthma, or who repeatedly present to an acute care setting despite
having a primary care provider.
21.
• Medications
•
Inhaled corticosteroids(ICS)
• Initiate ICS prior to discharge, if not previously prescribed. Patients currently
prescribed ics-containing medication should generally have their treatment
stepped up for 2–4 weeks and should be reminded about the importance of
adherence with daily use.
Oral corticosteroids (ocs)
• Prescribe at least a 5–7 day course of OCS for adults (prednisolone or
equivalent 40-50 mg/day) and 3–5 days for children (1–2 mg/kg/day to a
maximum of 40 mg/day). Review progress before ceasing OCS. If the OCS is
dexamethasone, treatment is only for total 1-2 days.
• For patients considered at risk of poor adherence, intramuscular
corticosteroids may be considered).
Reliever medication
• Transfer patients back to as-needed rather than regular reliever medication
use, based on symptomatic and objective improvement.
• If ipratropium bromide was used in the emergency department or hospital, it
22.
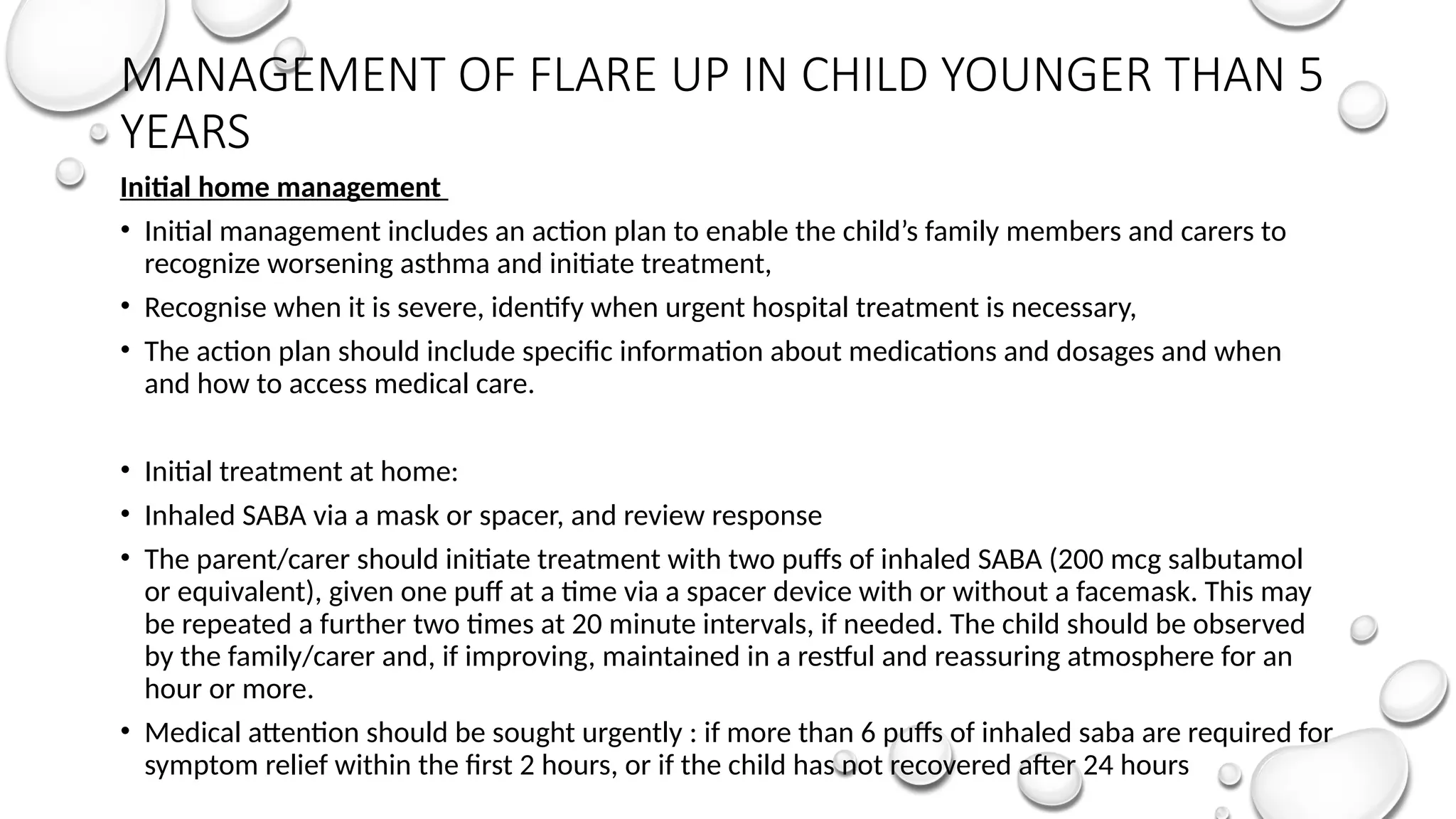
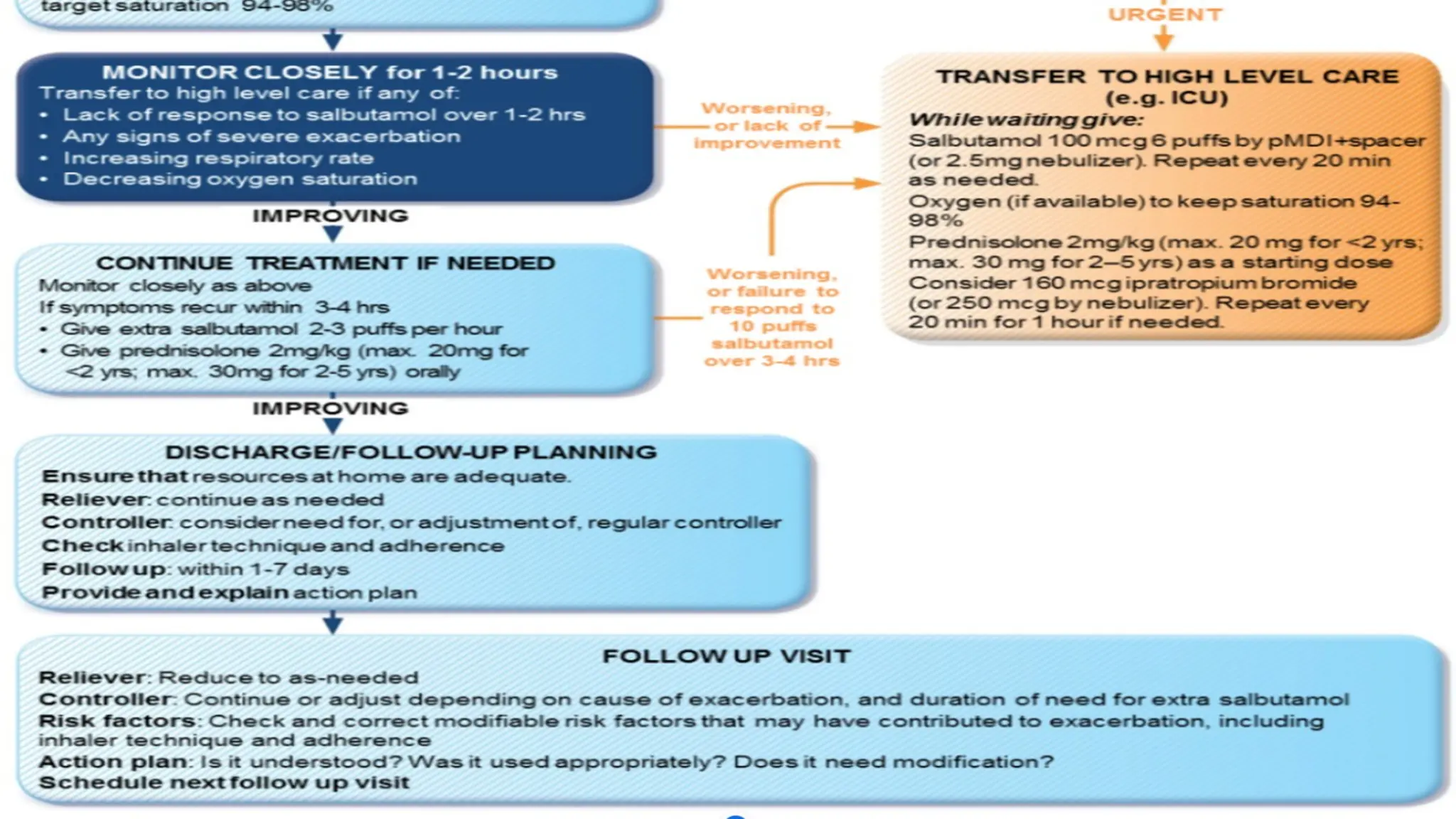
MANAGEMENT OF FLAREUP IN CHILD YOUNGER THAN 5
YEARS
Initial home management
• Initial management includes an action plan to enable the child’s family members and carers to
recognize worsening asthma and initiate treatment,
• Recognise when it is severe, identify when urgent hospital treatment is necessary,
• The action plan should include specific information about medications and dosages and when
and how to access medical care.
• Initial treatment at home:
• Inhaled SABA via a mask or spacer, and review response
• The parent/carer should initiate treatment with two puffs of inhaled SABA (200 mcg salbutamol
or equivalent), given one puff at a time via a spacer device with or without a facemask. This may
be repeated a further two times at 20 minute intervals, if needed. The child should be observed
by the family/carer and, if improving, maintained in a restful and reassuring atmosphere for an
hour or more.
• Medical attention should be sought urgently : if more than 6 puffs of inhaled saba are required for
symptom relief within the first 2 hours, or if the child has not recovered after 24 hours
26.
Discharge and followup after an exacerbation
Before discharge, the condition of the child should be stable (e.G. He/she
should be out of bed and able to eat and drink without problems).
Children who have recently had an asthma exacerbation are at risk of further
exacerbations and require follow up. The purpose is to ensure complete
recovery, to establish the cause of the exacerbation, and, when necessary, to
establish appropriate maintenance treatment and adherence .
Prior to discharge from the emergency department or hospital, family/carers
should receive the following advice and information I.E instruction on
recognition of signs of recurrence and worsening of asthma.
The factors that precipitated the exacerbation should be identified, and
strategies for future avoidance of these factors implemented.
A written, individualised action plan, including details of accessible
emergency services. Careful review of inhaler technique.