This study examined the association between parental education level, accuracy in perceiving a child's weight status, and willingness to accept obesity counseling from non-physician providers. The study found that parental education level was not associated with accurately perceiving a child's weight, having an overweight or obese child, or willingness to receive counseling from sources other than a physician. Parents of all education levels were most willing to receive counseling from a medical doctor and least willing from a schoolteacher. The study was limited by using a convenience sample and only assessing two non-physician counseling sources.
Implementing NutriSTEP® in Ontario - Success Stories, Lessons Learned and Nex...Nutrition Resource Centre
This presentation will briefly cover what is nutrition screening and the ethical issues around screening for nutritional risk in young children.
In addition to this brief introduction, we will have a number of dietitians present the implementation and evaluation of NutriSTEP in their communities as well as in other communities using similar models. A brief summary of the provincial process evaluation results will be reviewed and then we will wrap up with some of the other activities and next steps in the NutriSTEP Program. We will conclude with a 20-30 minute discussion period for a Q&A Period.
The NutriSTEP questionnaire targets The child’s parent or primary caregiver—the person who is most knowledgeable about the child’s eating and other health habits.
It is a paper and pencil questionnaire with 17 questions covering the four constructs of nutrition risk for this age group. These are:
Physical growth and weight concerns
Food and fluid intake
Physical activity and screen time
Factors affecting food intake (food security; and the psychosocial feeding environment)
We would like to tell you about NutriSTEP®. This work has been led by dietitian researchers from the Sudbury & District Health Unit Public Health, Research, Education & Development (PHRED) program, NRC and the University of Guelph, Dr Heather Keller and Dr Janis Randall Simpson.
As of spring 2007, NutriSTEP® has been a program of the Nutrition Resource Centre of the Ontario Public Health Association.
NutriSTEP® is of interest to a number of programs and agencies that service young children and their families.
The Youth-Nex Conference on Physical Health and Well-Being for Youth, Oct 10 & 11, 2013, University of Virginia
"Developing Sustainable Family-Centered Obesity Interventions: What Can
We Learn from Developmental Psychology and Implementation Science?"
- Kirsten Davison, Ph.D.
Davison is an Associate Professor of Nutrition at the Harvard School of Public Health. She completed her PhD at the Pennsylvania State University in Child and Family Development.
Panel 3 — Nutrition and Healthy Eating. As we understand more about what defines good nutrition for youth, we are also increasingly understanding the importance of instilling healthy eating habits for youth in the context of family, school, and sport. This varied panel covers major topics within this under-considered but important area of youth development.
Implementing NutriSTEP® in Ontario - Success Stories, Lessons Learned and Nex...Nutrition Resource Centre
This presentation will briefly cover what is nutrition screening and the ethical issues around screening for nutritional risk in young children.
In addition to this brief introduction, we will have a number of dietitians present the implementation and evaluation of NutriSTEP in their communities as well as in other communities using similar models. A brief summary of the provincial process evaluation results will be reviewed and then we will wrap up with some of the other activities and next steps in the NutriSTEP Program. We will conclude with a 20-30 minute discussion period for a Q&A Period.
The NutriSTEP questionnaire targets The child’s parent or primary caregiver—the person who is most knowledgeable about the child’s eating and other health habits.
It is a paper and pencil questionnaire with 17 questions covering the four constructs of nutrition risk for this age group. These are:
Physical growth and weight concerns
Food and fluid intake
Physical activity and screen time
Factors affecting food intake (food security; and the psychosocial feeding environment)
We would like to tell you about NutriSTEP®. This work has been led by dietitian researchers from the Sudbury & District Health Unit Public Health, Research, Education & Development (PHRED) program, NRC and the University of Guelph, Dr Heather Keller and Dr Janis Randall Simpson.
As of spring 2007, NutriSTEP® has been a program of the Nutrition Resource Centre of the Ontario Public Health Association.
NutriSTEP® is of interest to a number of programs and agencies that service young children and their families.
The Youth-Nex Conference on Physical Health and Well-Being for Youth, Oct 10 & 11, 2013, University of Virginia
"Developing Sustainable Family-Centered Obesity Interventions: What Can
We Learn from Developmental Psychology and Implementation Science?"
- Kirsten Davison, Ph.D.
Davison is an Associate Professor of Nutrition at the Harvard School of Public Health. She completed her PhD at the Pennsylvania State University in Child and Family Development.
Panel 3 — Nutrition and Healthy Eating. As we understand more about what defines good nutrition for youth, we are also increasingly understanding the importance of instilling healthy eating habits for youth in the context of family, school, and sport. This varied panel covers major topics within this under-considered but important area of youth development.
Latent Class Analysis of Adolescent Health Behaviorsasclepiuspdfs
Background: Behavior is one of the most important components in health. While the impacts of adolescent risky activities have been studied extensively, less attention has been paid to health. This study examines the patterning of health behaviors among adolescents age of 10–19 years. Methods: Latent class analysis identified homogeneous, mutually exclusive “classes” (patterns) of eight, leading health behaviors - sleep, alcohol consumption, cigarette smoking, physicians’ visits, meal autonomy, wearing braces, general health assessment, and having a permanent tattoo. Results: Resulting classes include (1) healthy, (2) moderately healthy, and (3) unhealthy. The characteristic behaviors and tendencies of each class differed by gender. Conclsion: This study attempts to classify adolescents by their own health behavior without including parental attributes. While adolescents do not typically prescribe to predictable behaviors and actions, the emphasis on healthy behaviors by some suggests an individual awareness of behavioral impacts and importance of healthy lifestyle choices
Childhood obesity, a very complex health issue that becomes a growing problem in the U.S. In fact, “over the past three decades, childhood obesity rates have tripled in the U.S., and today, the country has some of the highest obesity rates in the world: one out of six children is obese, and one out of three children is overweight or obese.” (Child obesity, n.d.). Physical diseases and conditions are often accompanying obesity. Also, obesity may have an adverse effect on various systems in a child’s body, such as heart, lungs, muscles and bones, kidneys, digestive tract, and hormones that control blood sugar and puberty. Furthermore, it can take a toll on social life because obese kids and teenagers are more likely to have low self-esteem. “Childhood obesity is one of the most serious threats to the health of our nation.” (Building evidence to prevent childhood obesity, n.d.). Children and youth who are obese and overweight will likely remain overweight or obese into adulthood.
References
Building evidence to prevent childhood obesity. (n.d.). Retrieved from https://www.rwjf.org/content/rwjf/en/how-we-work/grants-explorer/featured-programs/healthy-eating-research.html
Childhood obesity. (n.d.). Retrieved from https://www.hsph.harvard.edu/obesity-prevention-source/obesity-trends/global-obesity-trends-in-children/
Service providers who receive high nutrition risk referrals, particularly Registered Dietitians, need to be knowledgeable about general and clinical pediatric nutrition as well as counselling skills for working with families and children.
This is the second of five self-directed training modules available in PowerPoint presentations that have been developed and evaluated to respond to this need
A slide presentation on causes, effects and solutions of childhood obesity.
Created for eng102 course.
This presentation deal with the problems of obesity in childhood and probable solutions of obesity.
Presented as part of a Canadian Institutes of Health funded Knowledge Translation Supplement grant (KTB-112487). Recorded October 14, 2012 in Australia. Re-broadcast of an earlier recording. Recorded May 23, 2012.
Childhood obesity is a serious medical condition that affects children and adolescents. One of the best strategies to reduce childhood obesity is to improve the eating and exercise habits of your entire family. Treating and preventing childhood obesity helps protect your child's health now and in the future.
To know more facts related to obesity contact:
https://www.drmanishjoshi.com/
Presentation on childhood obesity prevention in early childhood settings. Presented April 28, 2011 at the DOD/USDA Family Resilience conference, Chicago, IL.
Latent Class Analysis of Adolescent Health Behaviorsasclepiuspdfs
Background: Behavior is one of the most important components in health. While the impacts of adolescent risky activities have been studied extensively, less attention has been paid to health. This study examines the patterning of health behaviors among adolescents age of 10–19 years. Methods: Latent class analysis identified homogeneous, mutually exclusive “classes” (patterns) of eight, leading health behaviors - sleep, alcohol consumption, cigarette smoking, physicians’ visits, meal autonomy, wearing braces, general health assessment, and having a permanent tattoo. Results: Resulting classes include (1) healthy, (2) moderately healthy, and (3) unhealthy. The characteristic behaviors and tendencies of each class differed by gender. Conclsion: This study attempts to classify adolescents by their own health behavior without including parental attributes. While adolescents do not typically prescribe to predictable behaviors and actions, the emphasis on healthy behaviors by some suggests an individual awareness of behavioral impacts and importance of healthy lifestyle choices
Childhood obesity, a very complex health issue that becomes a growing problem in the U.S. In fact, “over the past three decades, childhood obesity rates have tripled in the U.S., and today, the country has some of the highest obesity rates in the world: one out of six children is obese, and one out of three children is overweight or obese.” (Child obesity, n.d.). Physical diseases and conditions are often accompanying obesity. Also, obesity may have an adverse effect on various systems in a child’s body, such as heart, lungs, muscles and bones, kidneys, digestive tract, and hormones that control blood sugar and puberty. Furthermore, it can take a toll on social life because obese kids and teenagers are more likely to have low self-esteem. “Childhood obesity is one of the most serious threats to the health of our nation.” (Building evidence to prevent childhood obesity, n.d.). Children and youth who are obese and overweight will likely remain overweight or obese into adulthood.
References
Building evidence to prevent childhood obesity. (n.d.). Retrieved from https://www.rwjf.org/content/rwjf/en/how-we-work/grants-explorer/featured-programs/healthy-eating-research.html
Childhood obesity. (n.d.). Retrieved from https://www.hsph.harvard.edu/obesity-prevention-source/obesity-trends/global-obesity-trends-in-children/
Service providers who receive high nutrition risk referrals, particularly Registered Dietitians, need to be knowledgeable about general and clinical pediatric nutrition as well as counselling skills for working with families and children.
This is the second of five self-directed training modules available in PowerPoint presentations that have been developed and evaluated to respond to this need
A slide presentation on causes, effects and solutions of childhood obesity.
Created for eng102 course.
This presentation deal with the problems of obesity in childhood and probable solutions of obesity.
Presented as part of a Canadian Institutes of Health funded Knowledge Translation Supplement grant (KTB-112487). Recorded October 14, 2012 in Australia. Re-broadcast of an earlier recording. Recorded May 23, 2012.
Childhood obesity is a serious medical condition that affects children and adolescents. One of the best strategies to reduce childhood obesity is to improve the eating and exercise habits of your entire family. Treating and preventing childhood obesity helps protect your child's health now and in the future.
To know more facts related to obesity contact:
https://www.drmanishjoshi.com/
Presentation on childhood obesity prevention in early childhood settings. Presented April 28, 2011 at the DOD/USDA Family Resilience conference, Chicago, IL.
Obesity is quickly becoming one of the most common chronic.docxhopeaustin33688
Obesity is quickly becoming one of the most common chronic diseases among children. These rates have increased at an alarming rate and is a major public health problem because of related physical and psychological comorbidities, including type II diabetes, insulin resistance, metabolic syndrome, cardiovascular disease and mental health disorders. Dramatic increase in the number of overweight and obese children in recent years.
Studies indicate that children's lives may be shortened as a result of this alarming health problem. Estimates state that for any degree of overweight/obesity, younger adults (20-30 years of age) may have greater years of life lost due to obesity than older adults. Childhood obesity has been determined to be an independent risk factor for adult overweight/obesity.
To combat childhood obesity, there is a great need for public health interventions as well as education parents regarding childhood obesity and its consequences. Parents differ on causation of obesity, and differ in focus on nutrition and physical exercise. Many parents in the research do not see obesity as a barrier to physical activity. The parents need to recognize their child as overweight. Prevention is the most effective method for dealing with this growing health concern. The evidence reviewed, confirmed that family-centered interventions were associated with short-term reduction in obesity and improved medical parameters. The goal should be to involve community resources and provider referrals. Nurse Practitioners have a unique role in being the best facilitators to deliver health messages and are able to educate parents and increase awareness about the causes and consequences of childhood obesity.
Parents of young children need to interact with their child's primary healthcare provider for health advice and preventive health information during regularly scheduled physical examinations. It is up to the parents of these young children to combat intervention strategies such as:
a combination of nutritional and activity information, a cognitive-behavioral aspect to the intervention parent-directed activities
limiting sedentary child behaviors, provide positive approaches with children by parents and practitioners (e.g., emphasize positive rewards for healthy behaviors, encourage self-efficacy)
Future research is required to identify moderators and mediators to produce enduring changes in weight status of children.
The Objective was to determine in children who are at risk for becoming overweight or obese, does education with parental involvement on exercise and nutrition compared to individual education with the child alone decrease the risk of developing obesity and the health problems associated with obesity?
(P) In overweight, obese, or at risk young children (2-18years of age) Is family centered education/treatment interventions
(C) versus control or comparison interventions
(O) more effective in decreasing childhood obesity and compli.
Child-health practitioners in Iowa must find better ways to address family, neighborhood and economic factors that shape children' health and well being, according to CFPC executive director Charles Bruner and Debra Waldron, director and chief medical officer of the Child Health Specialty Clinics at the University of Iowa. They presented at the Iowa Governor's Conference on Public Health in Ames on April 5.
NEED BY 061220 CST Chicago, IL time . NO PLAGIARISM ALLOWED!!.docxTanaMaeskm
NEED BY 06/12/20 CST Chicago, IL time . NO PLAGIARISM ALLOWED!!
SHOULD PARENTS DETERMINE FAMILY EATING HABITS WHEN THE CHILD IS OBESE
Describes statistical significance to pediatric nursing grounded in scholarly literature. Collates utilized references and summarizes key points.
· Statistical significance-
· Key Points
***Need 1 scholarly source
Use the article attached the title is for this presentation:
SHOULD PARENTS DETERMINE FAMILY EATING HABITS WHEN THE CHILD IS OBESE?"
KEYPOINTS: answer theses questions and describe statistical data
· Childhood Obesity- What is their growth/BMI?
· Is there a pathophysiological dilemma such as Binge Eating Disorder (BED)?
· What are the cultural differences and customs to provide client centered quality care?
· How can we observe and assess what beliefs the client has on food choices and psychosocial needs?
· What are their cognitive level/ learning needs?
· What are their educational needs?
· What availability does client have to food and nutrition (economical status)?
· What are some healthy food choices and activity for better living?
· What can we provide as resources to client when there is economical hardships involved?
· What beliefs or morals are ok with you on this topic?
STATISTICAL SIGNIFICANCE:
** use the article attached and another scholarly source of choice if needed
APA FORMAT and intext citation
NEED BY
06/12/20 CST Chicago
, IL
t
ime
. NO
PLAGIARISM ALLOWED!!
SHOULD PARENTS DETERMINE FAMILY EATING HABITS WHEN THE CHILD IS OBESE
Describes statistical significance to pediatric nursing grounded in scholarly literature. Collates utilized
references and summarizes key points.
·
Statistical significance
-
·
Key
Points
***
Need
1
scholarly source
Use the article attached the title is for this presentation
:
SHOULD PARENTS DETERMINE FAMILY EATING HABITS WHEN THE CHILD IS OBESE?"
K
EYPOI
NTS:
answer the
ses questions and describe stati
s
tical data
·
Childhood Obesity
-
What is their growth/BMI?
·
Is there a pathophysiological dilemma such as Binge Eating Disorder (BED)?
·
What are the
cultural differences and cus
toms to provide client centered quality care?
·
How can we observe and assess what beliefs the client has on food choices and psychosocial
needs?
·
What are their cognitive level/ learning needs?
·
What are their educational needs?
·
What availability does client have to food and nutrition (economical status)?
·
What are some healthy food choices and activity for better living?
·
What can we provide as resources to client when there is economical hardships involved?
·
W
hat
bel
iefs or morals are ok wi
th you on this t
opic?
STATISTIC
AL SIGNIF
ICANCE
:
** use the article attached and
another sch
olarly source o
f choice
if nee
ded
APA FORMAT and intext citation
NEED BY 06/12/20 CST Chicago, IL time . NO PLAGIARISM ALLOWED!!
SHOULD PARENTS DETERMINE FAMILY EATING HABITS WHEN THE CHILD IS OBESE
De.
NEED BY 061220 CST Chicago, IL time . NO PLAGIARISM ALLOWED!!.docxhallettfaustina
NEED BY 06/12/20 CST Chicago, IL time . NO PLAGIARISM ALLOWED!!
SHOULD PARENTS DETERMINE FAMILY EATING HABITS WHEN THE CHILD IS OBESE
Describes statistical significance to pediatric nursing grounded in scholarly literature. Collates utilized references and summarizes key points.
· Statistical significance-
· Key Points
***Need 1 scholarly source
Use the article attached the title is for this presentation:
SHOULD PARENTS DETERMINE FAMILY EATING HABITS WHEN THE CHILD IS OBESE?"
KEYPOINTS: answer theses questions and describe statistical data
· Childhood Obesity- What is their growth/BMI?
· Is there a pathophysiological dilemma such as Binge Eating Disorder (BED)?
· What are the cultural differences and customs to provide client centered quality care?
· How can we observe and assess what beliefs the client has on food choices and psychosocial needs?
· What are their cognitive level/ learning needs?
· What are their educational needs?
· What availability does client have to food and nutrition (economical status)?
· What are some healthy food choices and activity for better living?
· What can we provide as resources to client when there is economical hardships involved?
· What beliefs or morals are ok with you on this topic?
STATISTICAL SIGNIFICANCE:
** use the article attached and another scholarly source of choice if needed
APA FORMAT and intext citation
NEED BY
06/12/20 CST Chicago
, IL
t
ime
. NO
PLAGIARISM ALLOWED!!
SHOULD PARENTS DETERMINE FAMILY EATING HABITS WHEN THE CHILD IS OBESE
Describes statistical significance to pediatric nursing grounded in scholarly literature. Collates utilized
references and summarizes key points.
·
Statistical significance
-
·
Key
Points
***
Need
1
scholarly source
Use the article attached the title is for this presentation
:
SHOULD PARENTS DETERMINE FAMILY EATING HABITS WHEN THE CHILD IS OBESE?"
K
EYPOI
NTS:
answer the
ses questions and describe stati
s
tical data
·
Childhood Obesity
-
What is their growth/BMI?
·
Is there a pathophysiological dilemma such as Binge Eating Disorder (BED)?
·
What are the
cultural differences and cus
toms to provide client centered quality care?
·
How can we observe and assess what beliefs the client has on food choices and psychosocial
needs?
·
What are their cognitive level/ learning needs?
·
What are their educational needs?
·
What availability does client have to food and nutrition (economical status)?
·
What are some healthy food choices and activity for better living?
·
What can we provide as resources to client when there is economical hardships involved?
·
W
hat
bel
iefs or morals are ok wi
th you on this t
opic?
STATISTIC
AL SIGNIF
ICANCE
:
** use the article attached and
another sch
olarly source o
f choice
if nee
ded
APA FORMAT and intext citation
NEED BY 06/12/20 CST Chicago, IL time . NO PLAGIARISM ALLOWED!!
SHOULD PARENTS DETERMINE FAMILY EATING HABITS WHEN THE CHILD IS OBESE
De.
Service providers who receive high nutrition risk referrals, particularly Registered Dietitians, need to be knowledgeable about general and clinical pediatric nutrition as well as counselling skills for working with families and children.
This is the first of five self-directed training modules available in PowerPoint presentations that have been developed and evaluated to respond to this need
External validation of an electronic phenotyping algorithm to detect attentio...TÀI LIỆU NGÀNH MAY
Để xem full tài liệu Xin vui long liên hệ page để được hỗ trợ
: https://www.facebook.com/thuvienluanvan01
HOẶC
https://www.facebook.com/garmentspace/
https://www.facebook.com/thuvienluanvan01
https://www.facebook.com/thuvienluanvan01
tai lieu tong hop, thu vien luan van, luan van tong hop, do an chuyen nganh
Early Childhood Risk and Obesity in Preschool-age Children via Salivary Testing UCLA CTSI
Principal Investigators: Francisco Ramos-Gomez (UCLA) and Robert Jones (University of Minnesota)
UCLA CTSI and University of Minnesota Cross-Institutional Award Projects
The overall goal of our study is to develop an integrated care plan that effectively addresses the shared risk factors of early childhood dental decay, early childhood cavities (ECC) and obesity. It encourages parents of disadvantaged and of minority backgrounds to adopt broad self-management goals and overall comprehensive health-promoting habits. There is a pressing need for community-based participatory early intervention approaches to prevent both early childhood dental decay and obesity at a younger age. Within the recent healthcare environment, oral health (dentistry) may play an important role within the whole community approach to obesity prevention as an entry point for discussing diet and nutrition early on. Some key reasons for the importance of oral health integration into obesity prevention is that children’s oral health diseases share key risk factors with early obesity. In our study, the Infant Oral health visit promotes dietary guidance early in childhood, and oral health promotion is done in a culturally manner, which we use to discuss other broad health-promoting habits. Our immediate goal utilizes a university and community-based team to improve the ability to predict future dental decay in children and integrate oral health risk assessment with broad health-promoting habits that may one day prevent obesity in the key early years of the child development.
Speaker presentation from U.S. News Healthcare of Tomorrow leadership summit, Nov. 17-19, 2019 in Washington, DC. Find out more about this forum at www.usnewshot.com.
Speaker presentation from U.S. News Healthcare of Tomorrow leadership summit, Nov. 17-19, 2019 in Washington, DC. Find out more about this forum at www.usnewshot.com.
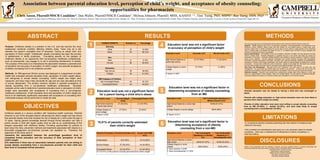
1. Association between parental education level, perception of child’s weight, and acceptance of obesity counseling:
opportunities for pharmacists
Chris Anson, PharmD/MSCR Candidate1; Dan Waller, PharmD/MSCR Candidate1; Melissa Johnson, PharmD, MHS, AAHIVE 1,2; Tina Tseng, PhD, MSPH1; Ray Tseng, DDS, PhD1,3,4
1Campbell University School of Pharmacy, Buies Creek, NC; 2Division of Infectious Diseases, Duke University Medical Center, Durham, NC; 3Dept. Of Nutrition, Gillings School of Global Public Health, 4Dept. of Pediatric Dentistry, School of Dentistry, University of North Carolina at Chapel Hill, Chapel Hill, NC.
ABSTRACT
OBJECTIVES
Authors of this presentation have the following to disclose concerning possible financial or personal relationships with
commercial entities that may have a direct or indirect interest in the subject matter of this presentation:
Christopher Anson: nothing to disclose
Daniel Waller: nothing to disclose
Melissa Johnson: nothing to disclose
Ray Tseng: nothing to disclose
Tina Tseng: nothing to disclose
Purpose: Childhood obesity is a problem in the U.S. and has become the most
widespread nutritional condition affecting children today. There may be a link
between the parent’s completed level of education, having an obese child, and
perception of child’s weight. Traditionally, obesity counseling has been the purview
of pediatricians or family physicians. Counseling parents on the dangers of
childhood obesity is an opportunity that non-physician healthcare professionals,
such as pharmacists, may engage in to aid in preventing development of obesity.
The purpose of this study is to characterize the association between a parental level
of education and accuracy of perception of child’s weight, and parental acceptance
of dietary counseling from a non-physician provider.
Methods: An IRB-approved 38-item survey was deployed in a department of public
health that evaluated parental education level, perception of child’s weight status,
and willingness to accept obesity counseling. Child’s weight and height were
measured, and body mass index percentile for age and sex was calculated at time
of survey deployment. The primary outcome variable is parental acceptance of
obesity counseling from a non-physician healthcare professional. Bivariate
analyses will be used to determine if parental education level or perception of child’s
weight were associated with acceptance of counseling from a non-physician
healthcare professional. If both education level and perception of child’s weight are
found to be statistically significantly associated with acceptance of counseling then
multivariate analysis will be performed to model the data.
75.51% of parents correctly estimated
their child’s weight
•Parental education was not related to having a child who was overweight or
obese.
•Parents with college education vs. high school education were not more likely to
perceive their child’s weight accurately.
•Parents of either education level were most willing to accept obesity counseling
from an MD (91-96%), a dentist (41-52%), and were least likely to accept
counseling from a schoolteacher (33-36%).
CONCLUSIONS
LIMITATIONS
DISCLOSURES
1
2
RESULTS METHODS
Childhood obesity is a serious condition with hazardous health outcomes. Parental
influence is one of the strongest factors influencing the child’s weight and has shown
that parental obesity more than doubles the risk of obesity for a child under the age of
10 years. Having general knowledge learned through formal education can help a
parent provide a child with higher quality food as well as an understanding of the
dangers associated with childhood obesity. Providing opportunities for parents to
learn about the risks, prevention methods and treatments associated with obesity is a
favourable engagement non-physician provider can capitalize on. Therefore, the
objectives of this study were to:
1)examine the association between the parent/legal guardians’ level of
completed formal education and the accuracy of their perception of their
child’s weight.
2)To determine if there was an association between parents who are willing to
accept obesity counselling from a non-physician provider for their child and
their level of completed formal education.
•A convenience sample of parents presenting with their children for treatment was
utilized for this study.
•Only a dentist and schoolteacher were given as a non-physician option for obesity
counseling - there was no assessment of willingness to receive counseling in a
pharmacy setting.
3
4 Education level was not a significant factor
in accuracy of perception of child’s weight
Education level was not a significant factor in
determining acceptance of obesity counseling
from an MD
Education Level Accurate n(%) Not Accurate n(%)
High School Diploma or
some high school
37 (77.08%) 11 (22.92%)
College Degree or some
college
37 (74%) 13 (26%)
P Value= 0.7227
Education Level Felt Comfortable Speaking to a
Medical Doctor n(%)
High School Diploma or some high
school
44/48 (91.67%)
College Degree or some college 48/50 (96%)
P Value= 0.3711
CHARACTERISTIC Number (n) Percentage
Ethnicity
White 43 43.88%
Black 55 56.12%
Sex
Male 9 9.18%
Female 89 90.82%
Education
High School 48 48.98%
College 50 51.02%
BMI Category of Children
Not Overweight/Obese 54 55.10%
Overweight/Obese 44 44.90%
Parent’s Perception Parental Estimate n(%) Actual Child BMI
n(%)
Underweight 9 (9.18%) 10 (10.20%)
Normal Weight 67 (68.34%) 44 (44.90%)
Overweight/Obese 22 (22.45%) 44 (44.90%)
74 (75.51%) of the parents correctly perceived their child's weight
5Education level was not a significant factor
for a parent having a child who’s obese
Education Level Normal Weight
Child
Overweight/Obese Child
High School Diploma
or some high school
27 (56.25%) 21 (43.75%)
College Degree or
some college
27 (54%) 23 (46%)
P Value= 0.823
6
Education Level Felt Comfortable
Speaking to a Dentist
(%)
Felt Comfortable
Speaking to a
Schoolteacher n(%)
High School Diploma or some
high school 20/48 (41.67%) 16/48 (33.33%)
College Degree or some
college 26/50 (52%) 18/50 (36%)
P Value Dentist= 0.3055
P Value Schoolteacher= 0.1209
Education level was not a significant factor in
determining acceptance of obesity
counseling from a non-MD
This study was approved by the Biomedical Review Board at the University of North Carolina Chapel Hill.
Subjects. Eligible subjects came from a convenience population of parents/guardians who presented at the
Alamance County Children’s Dental Center with their children for new patient exams or dental recall visits.
Inclusion criteria were 1) Adults completing the survey had to be the parent or legal guardian of the presenting
child, 2) children had to be between the ages of 2 and 17, 3) children had to be free of chronic diseases and
conditions, including food and/or drug allergies.
Survey Administration. A 38 question survey was available in Spanish or English, and was deployed from May
2009 to October 2009. Parental willingness to complete and turn in the survey was taken as consent for
participation in the study. A medically certified translator was available to answer questions in English or Spanish
during survey collection. Surveys obtained information from several domains including child demographic
information, parental demographic information, education level, general knowledge regarding overweight/obesity,
perceptions of his/her child’s weight classification, and his/her opinion of utilizing dietary counseling from a variety
of providers. Surveys were numbered in order of collection. Height (in) and weight (lb) information was collected
from the child’s medical record and used for calculation of the BMI percentile for age and sex.
Data Entry and Management. Microsoft Excel 2007 (Redmond, WA) was used for all data entry and
management. All survey data was double-coded and verified to be accurate. Surveys that did not have full
responses to all variables of interest were excluded from the analysis. Only one survey per parent was utilized.
Statistical Analysis. Education was recoded into a dichotomous variable (high school diploma or some high
school vs. college degree or some college). Stata 10.0 (College Station, TX) was used for all statistical analyses.
Descriptive statistics and pearson Chi Square analysis were calculated for all univariate analyses.