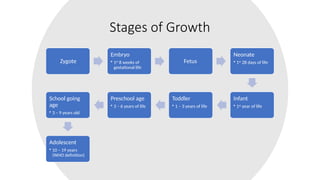
Stages of Growth
Zygote
Embryo
•1st
8 weeks of
gestational life
Fetus
Neonate
• 1st
28 days of life
Infant
• 1st
year of life
Toddler
• 1 – 3 years of life
Preschool age
• 3 – 6 years of life
School going
age
• 3 – 9 years old
Adolescent
• 10 – 19 years
(WHO definition)
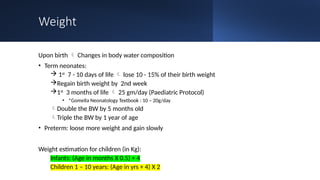
Weight
Upon birth Changes in body water composition
• Term neonates:
1st
7 - 10 days of life lose 10 - 15% of their birth weight
Regain birth weight by 2nd week
1st
3 months of life 25 gm/day (Paediatric Protocol)
• *Gomella Neonatology Textbook : 10 – 20g/day
Double the BW by 5 months old
Triple the BW by 1 year of age
• Preterm: loose more weight and gain slowly
Weight estimation for children (in Kg):
Infants: (Age in months X 0.5) + 4
Children 1 – 10 years: (Age in yrs + 4) X 2
9.
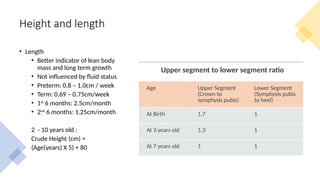
Height and length
•Length
• Better indicator of lean body
mass and long term growth
• Not influenced by fluid status
• Preterm: 0.8 – 1.0cm / week
• Term: 0.69 – 0.75cm/week
• 1st
6 months: 2.5cm/month
• 2nd
6 months: 1.25cm/month
2 - 10 years old :
Crude Height (cm) =
(Age(years) X 5) + 80
Upper segment to lower segment ratio
Age Upper Segment
(Crown to
symphysis pubis)
Lower Segment
(Symphysis pubis
to heel)
At Birth 1.7 1
At 3 years old 1.3 1
At 7 years old 1 1
10.
Head
Circumference
• 0.5-0.8cm /week
Intrauterinehead growth
• Reduces with age.
• Follows that of term infants when chronological
age reaches term
• If >1.25cm/week abnormal (hydrocephalus/IVH)
Preterm infants 1 cm/week
• 6 cm in first 3 months
• 3 cm in second 3 months
• 3 cm in last 6 months
Increases by 12 cm in the 1st year of life
11.
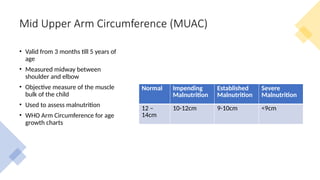
Mid Upper ArmCircumference (MUAC)
• Valid from 3 months till 5 years of
age
• Measured midway between
shoulder and elbow
• Objective measure of the muscle
bulk of the child
• Used to assess malnutrition
• WHO Arm Circumference for age
growth charts
Normal Impending
Malnutrition
Established
Malnutrition
Severe
Malnutrition
12 –
14cm
10-12cm 9-10cm <9cm
12.
Osseous Maturation
• Basedon number of Carpal Bones that appear (Request X-ray of wrist)
• She - Scaphoid – appear at 6 months
• Looks - Lunate – appear at 1 year
• Too - Triquetral - @ 2 yo
• Pretty - Pisiform - @ 3 yo
• Try - Trapezium - @ 4 yo
• To - Trapezoid - @ 5 yo
• Catch - Capitate - @ 6 yo
• Her - Hammate - @ 7 yo
• Bone age = chronological age + 1
• E.g. 3yo bone age 4 (i.e. 4 carpal bones have developed)
10yo ?
13.
Abnormal Bone Age
RetardedBone Age (e.g. 3 yo bone age 3 ) Advanced Bone Age
Prematurity Post maturity
Protein energy malnutrition Adrenogenital syndrome
Hypothyroidism Hyperthyroidism
Hypopituitarism Hyperpituitarism
14.
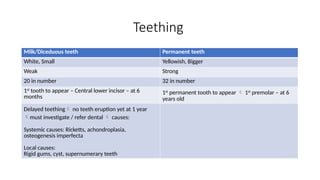
Teething
Milk/Diceduous teeth Permanentteeth
White, Small Yellowish, Bigger
Weak Strong
20 in number 32 in number
1st
tooth to appear – Central lower incisor – at 6
months
1st
permanent tooth to appear 1st
premolar – at 6
years old
Delayed teething no teeth eruption yet at 1 year
must investigate / refer dental causes:
Systemic causes: Ricketts, achondroplasia,
osteogenesis imperfecta
Local causes:
Rigid gums, cyst, supernumerary teeth
15.
Natal and neonatal
teeth
•Cause:
• Idiopathic
• Underlying syndromes: Soto’s syndrome(cerebral
gigantism), chondro ectodermal dysplasia ( Ellis
Van Crevald $)
• Baby born with 1 or 2 tooth – natal tooth
• 1 or 2 incisors erupt anytime during neonatal period –
neonatal tooth
• If there is no root for these teeth remove to prevent
risk of aspiration
• If root present can keep the teeth
16.
Fontanelles
• 6 fontanelles
•Anterior
• Posterior
• Rt and Lt Sphenoid
fontanelle
• Rt and Lt mastoid fontanelle
• Ant. Fontanelle –at birth 3FB
every 3 months, reduces in size
by 1 FB closes by 18 months
old
• Abnormal
• Wide / Closed early
• Bulging /Depressed
• Post. Fontanelle normal closes
at birth can be present up till 2
months and not more that 0.5cm
wide
• Abnormal
• Open after 2 months
old, regardless of size
• > 0.5cm regardless of
age
17.
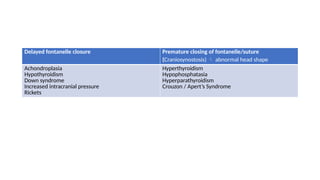
Delayed fontanelle closurePremature closing of fontanelle/suture
(Craniosynostosis) abnormal head shape
Achondroplasia
Hypothyroidism
Down syndrome
Increased intracranial pressure
Rickets
Hyperthyroidism
Hypophosphatasia
Hyperparathyroidism
Crouzon / Apert’s Syndrome
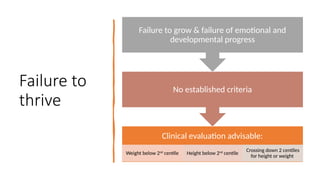
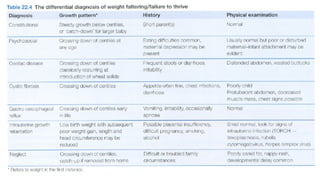
Failure to
thrive
Clinical evaluationadvisable:
Weight below 2nd
centile Height below 2nd
centile
Crossing down 2 centiles
for height or weight
No established criteria
Failure to grow & failure of emotional and
developmental progress
23.
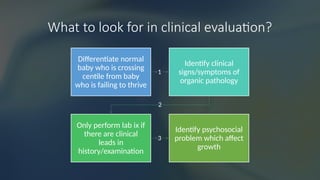
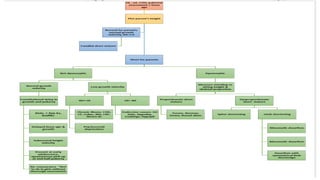
What to lookfor in clinical evaluation?
1
Differentiate normal
baby who is crossing
centile from baby
who is failing to thrive
2
Identify clinical
signs/symptoms of
organic pathology
3
Only perform lab ix if
there are clinical
leads in
history/examination
Identify psychosocial
problem which affect
growth
24.
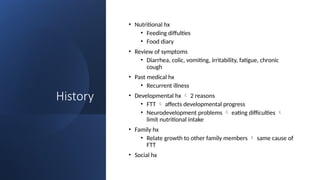
History
• Nutritional hx
•Feeding diffulties
• Food diary
• Review of symptoms
• Diarrhea, colic, vomiting, irritability, fatigue, chronic
cough
• Past medical hx
• Recurrent illness
• Developmental hx 2 reasons
• FTT affects developmental progress
• Neurodevelopment problems eating difficulties
limit nutritional intake
• Family hx
• Relate growth to other family members same cause of
FTT
• Social hx
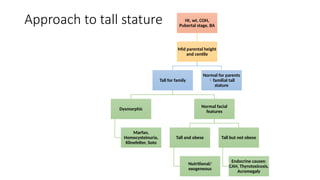
Approach to tallstature Ht, wt, COH,
Pubertal stage, BA
Mid parental height
and centile
Tall for family
Dysmorphic
Marfan,
Homocysteinuria,
Klinefelter, Soto
Normal facial
features
Tall and obese
Nutritional/
exogeneous
Tall but not obese
Endocrine causes:
CAH, Thyrotoxicosis,
Acromegaly
Normal for parents
familial tall
stature
33.
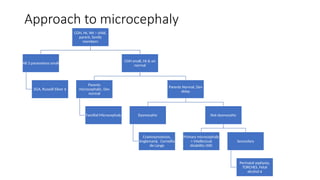
Approach to microcephaly
COH,Ht, Wt – child,
parent, family
members
All 3 parametres small
SGA, Russell Silver $
COH small, Ht & wt
normal
Parents
microcephalic, Dev
normal
Familial Microcephaly
Parents Normal, Dev
delay
Dysmorphic
Craniosynostosis,
Angleman$, Cornellia
de Lange
Not dysmorphic
Primary microcephaly
+ Intellectual
disability (AR)
Secondary
Perinatal asphyxia,
TORCHES, Fetal
alcohol $















![NORMAL GROWTH AND DEVELOPMENT- part 1 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/normalgrowthanddevelopment-part1autosaved-241024155104-94ab4150-thumbnail.jpg?width=640&height=640&fit=bounds)