What is Asthma?
Acondition that
• is chronic
• produces recurring episodes of
breathing problems
• is potentially life-threatening
• is not contagious
• cannot be cured, but can be
controlled
08/19/25
3.
Burden of Asthma
Asthma is one of the most common chronic
diseases worldwide with an estimated 300
million affected individuals
Prevalence increasing in many countries,
especially in children
A major cause of school/work absence
4.
How common isasthma?
• Asthma is a frequent disease in most countries
of the world including African countries
• It is common in both rich and poor countries
• In Zambia, official statistics on asthma are not
available
• An unpublished study (Somwe et al, 2013)
suggested it affects about 6-8 % of school
going children in Lusaka.
08/19/25 4
5.
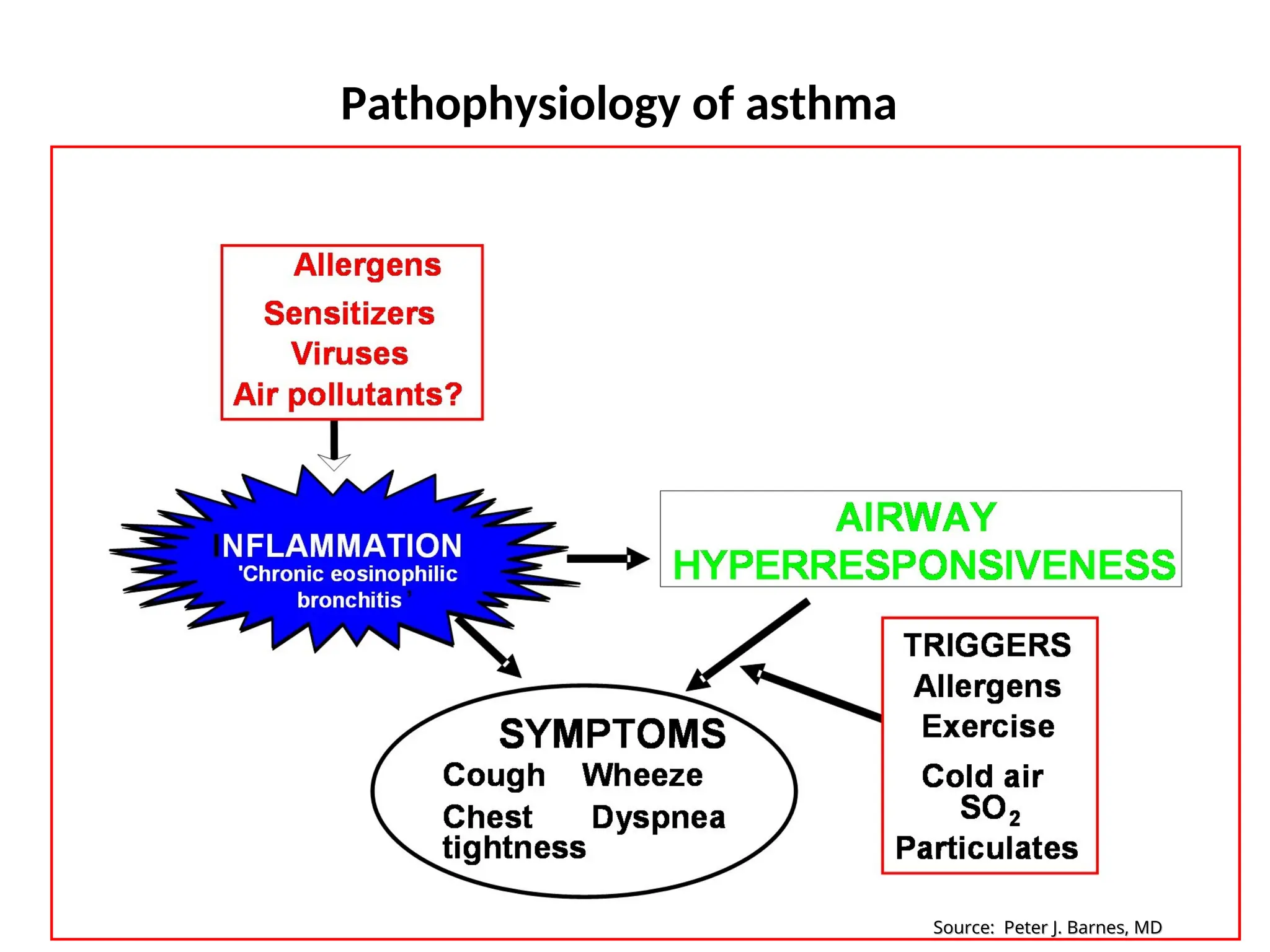
Risk Factors forAsthma
Host factors: predispose individuals to, or
protect them from, developing asthma
Environmental factors: influence
susceptibility to development of asthma in
predisposed individuals, precipitate asthma
exacerbations, and/or cause symptoms to
persist
• Exercise
• Changesin
weather and
temperature
• Infections in the upper
airways, such as colds
• Physical expressions
of strong feelings
(crying or laughing
hard, yelling)
Common triggers of asthma
08/19/25 11
12.
Allergens such as
•Furred and
feathered animals
• Dust mites
• Cockroaches
• Pollens
from grass and
trees
• Molds (indoors
and outdoors)
08/19/25 12
13.
Irritants such as
•Environmental
tobacco smoke
• Scented
products
• Strong fumes or
odors
• Outdoor air
pollution
08/19/25 13
14.
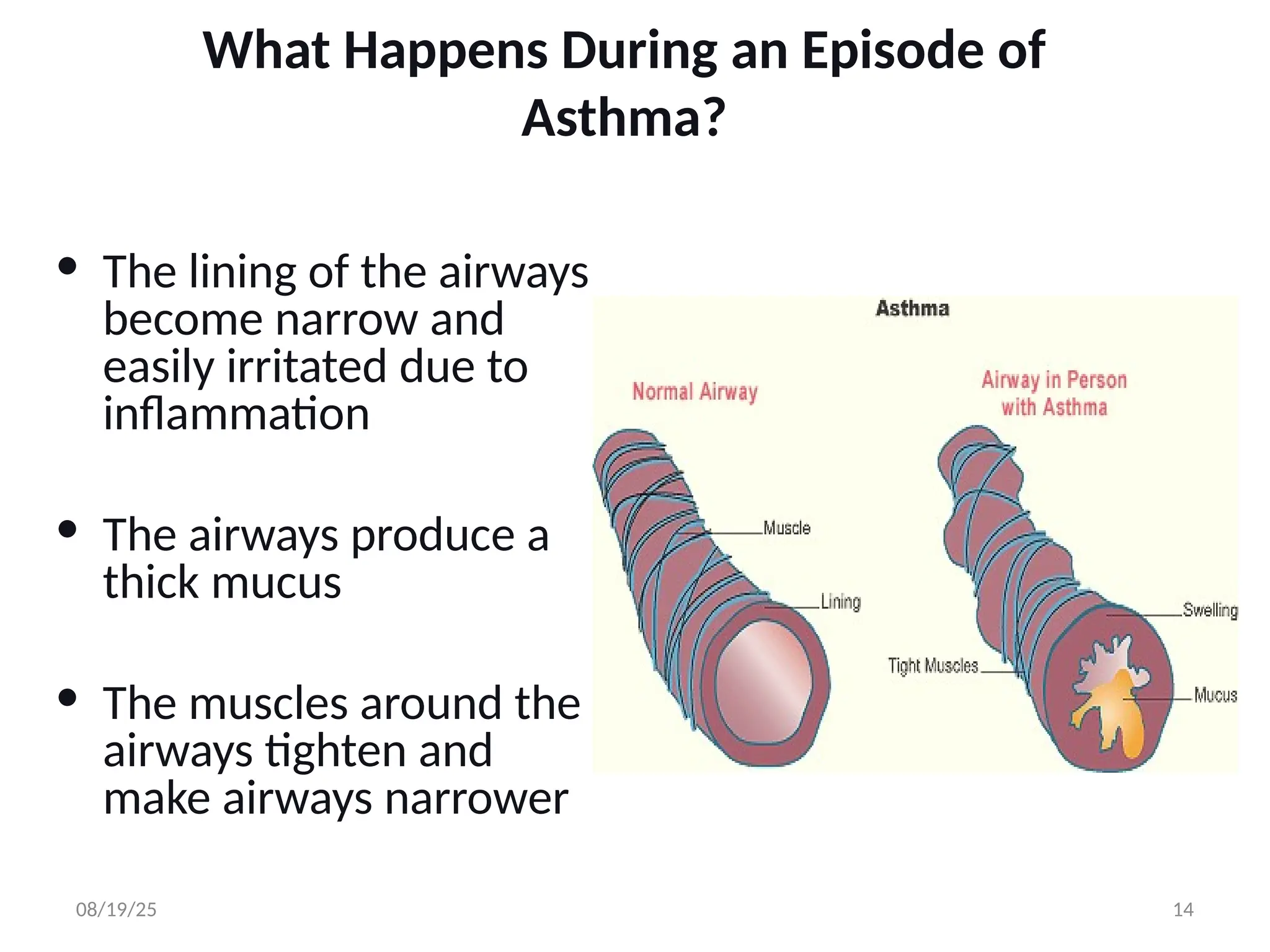
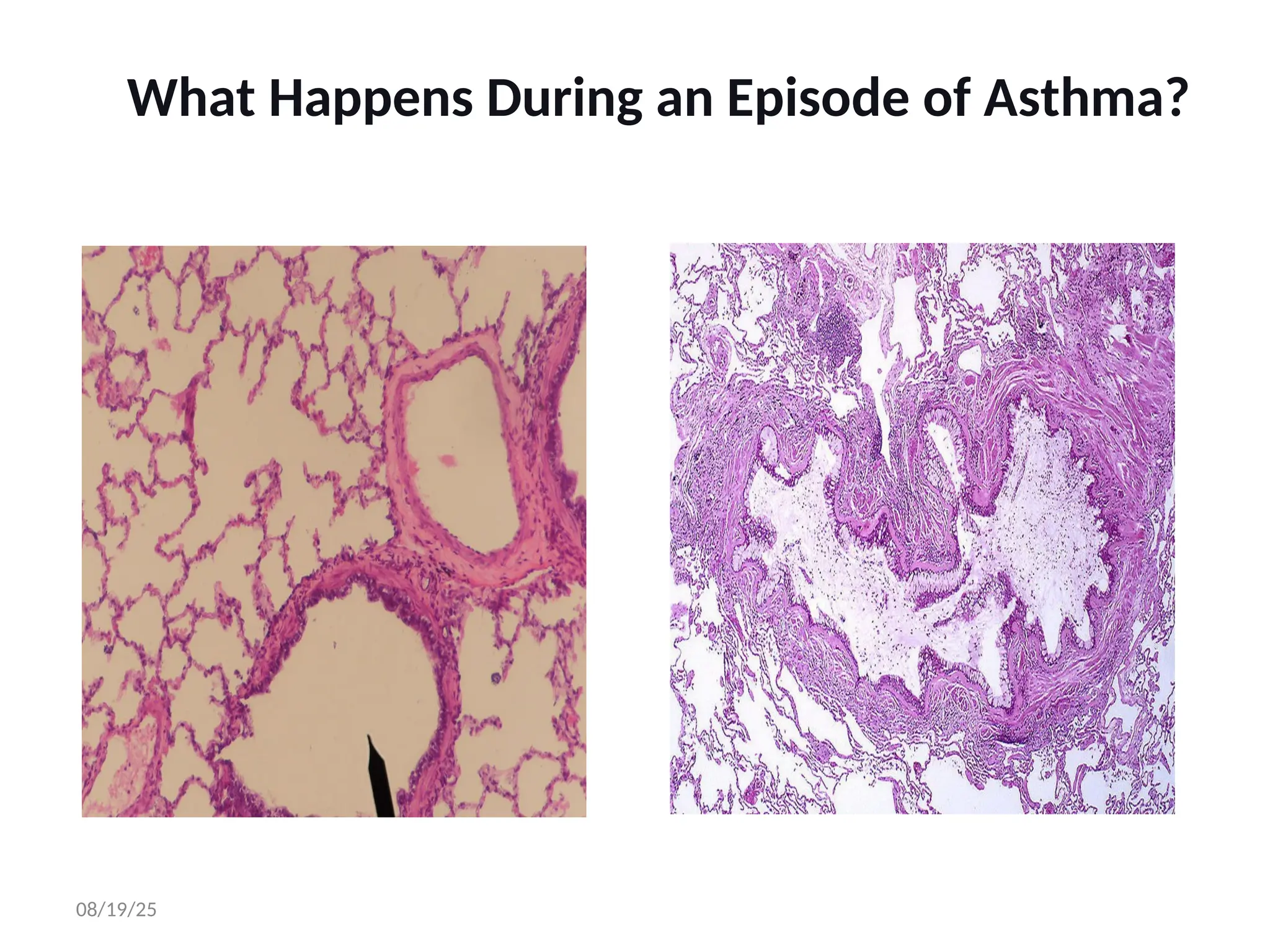
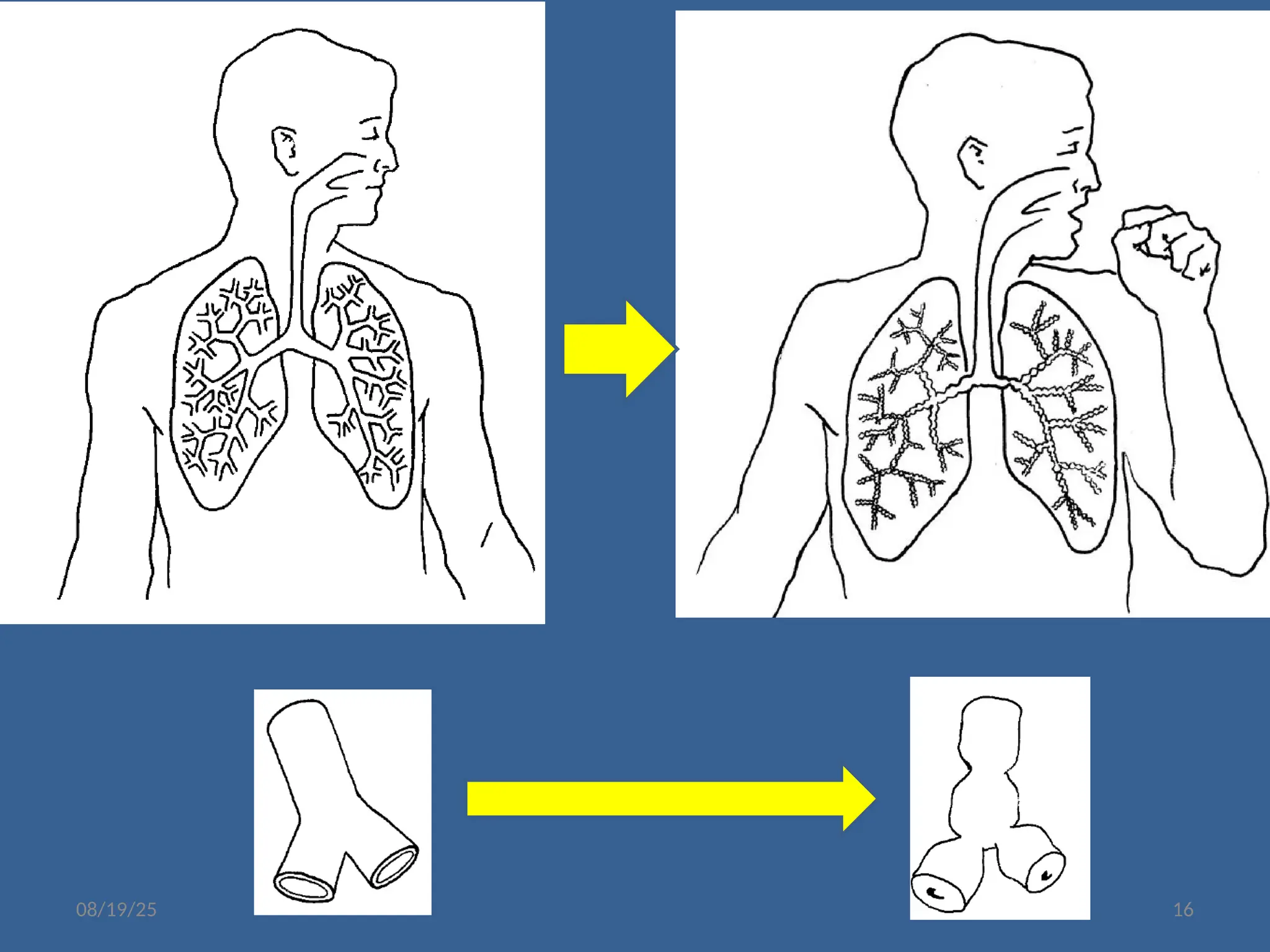
What Happens Duringan Episode of
Asthma?
• The lining of the airways
become narrow and
easily irritated due to
inflammation
• The airways produce a
thick mucus
• The muscles around the
airways tighten and
make airways narrower
08/19/25 14
How is asthmadiagnosed?
• Medical history
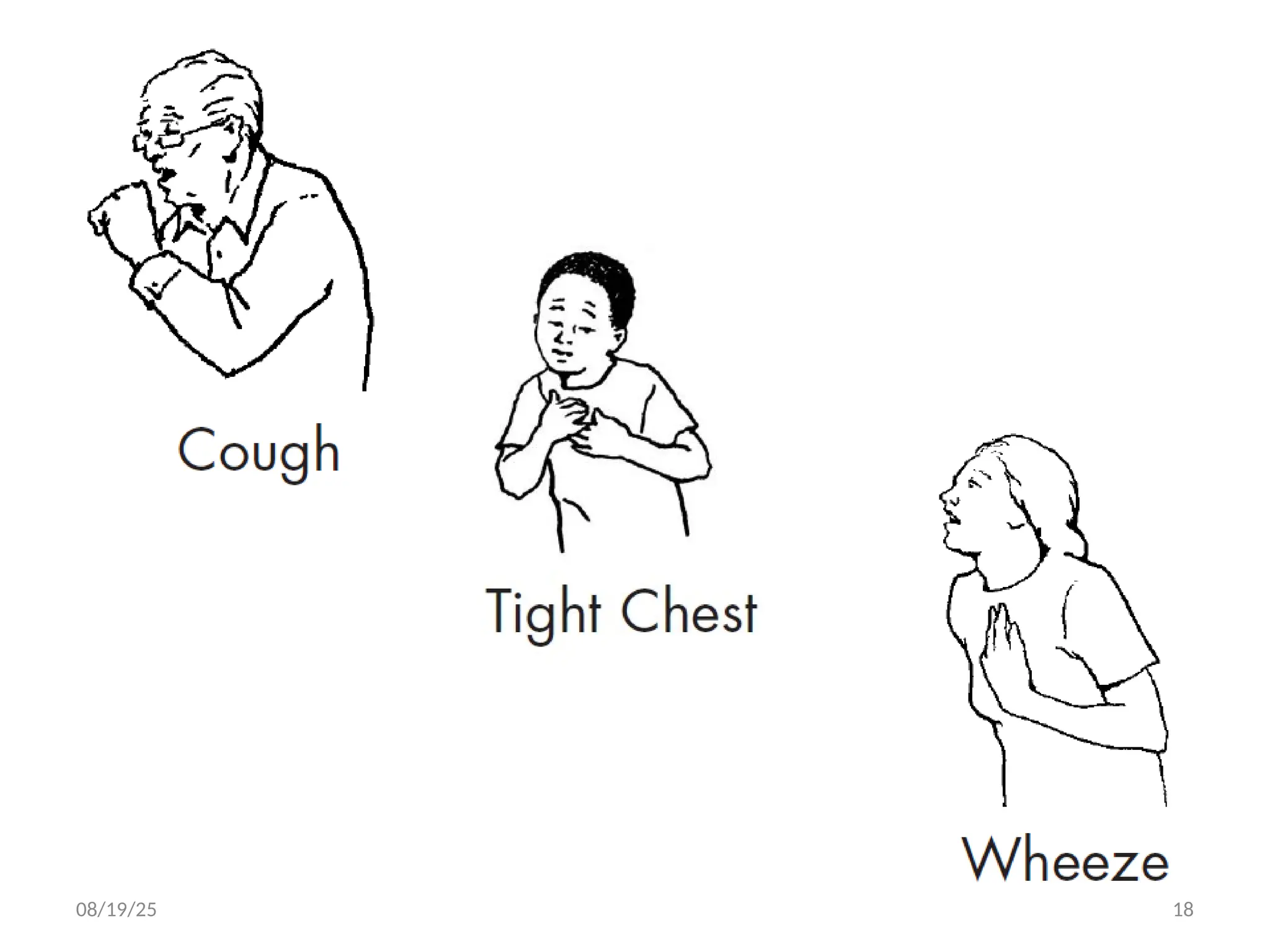
– Recurring cough, wheeze, difficulty breathing
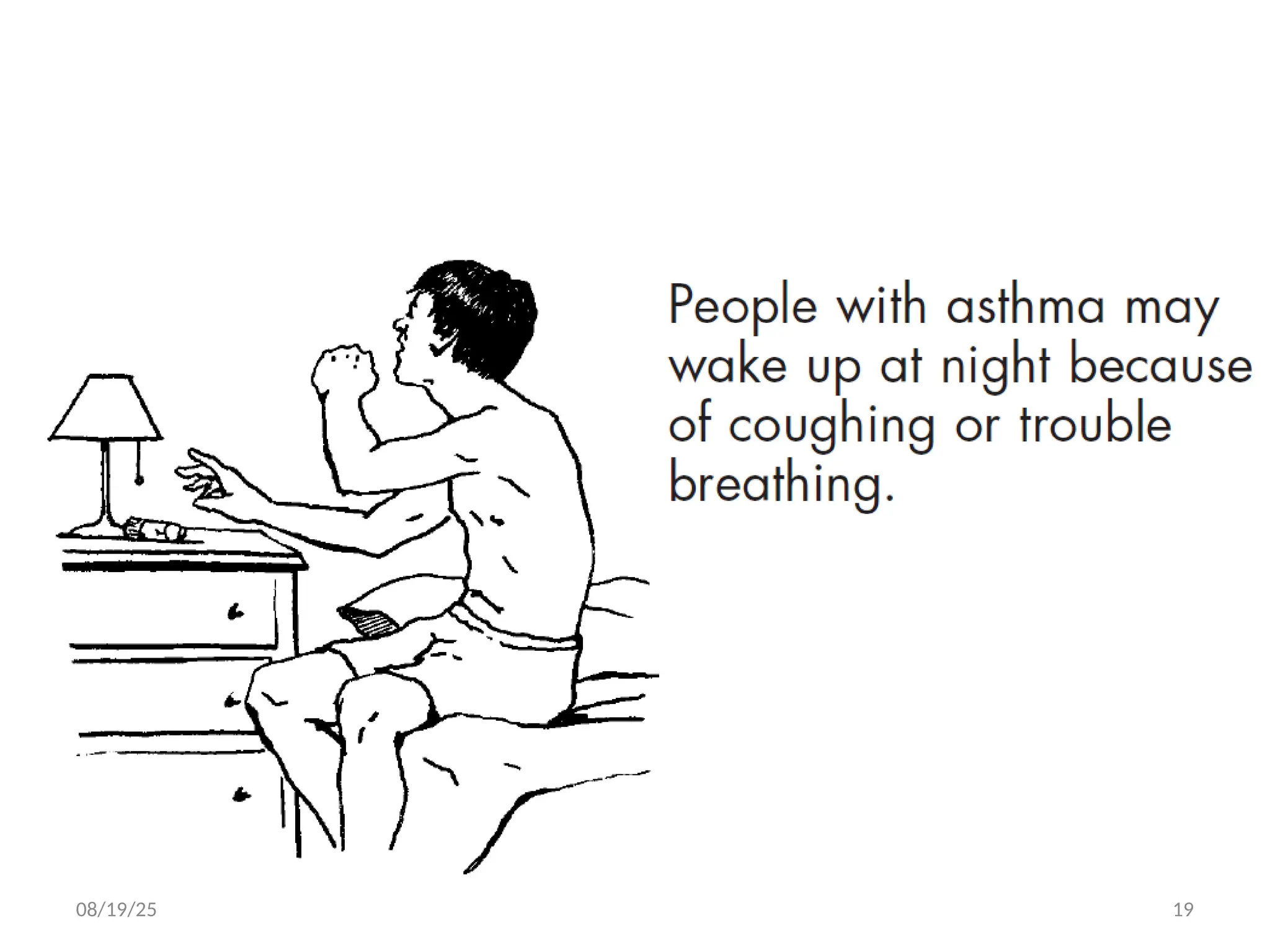
– Night cough, chest tightness
– Family history of asthma
– Allergies, eczema
• Physical examination
• Tests
– Test for lung function
– Test for allergies
– ? X-ray
08/19/25 21
Most of the times doctors rely on accurate description of
the symptoms and examination in making the diagnosis.
22.
Asthma Diagnosis
Historyand patterns of symptoms
Measurements of lung function
- Spirometry
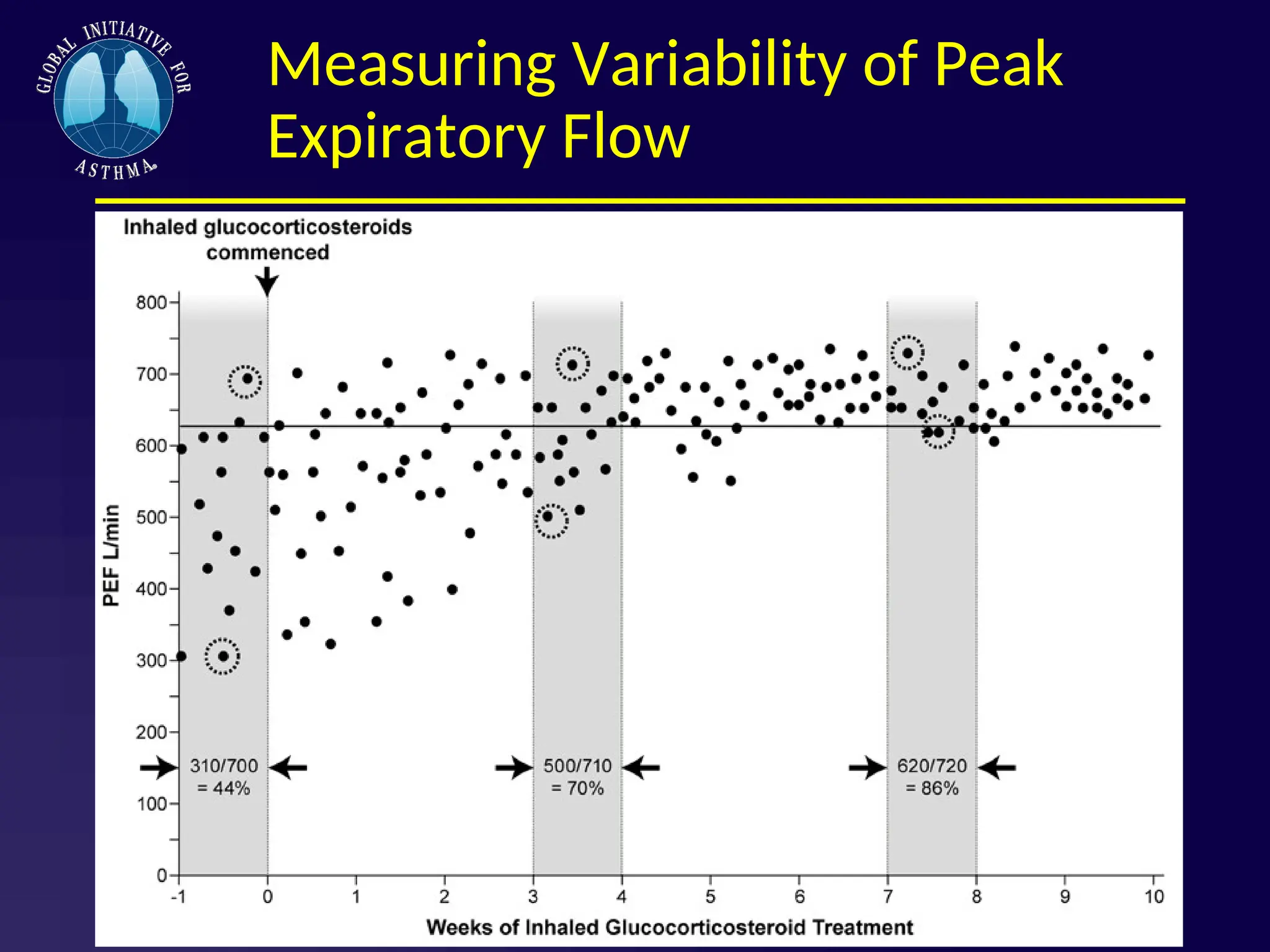
- Peak expiratory flow
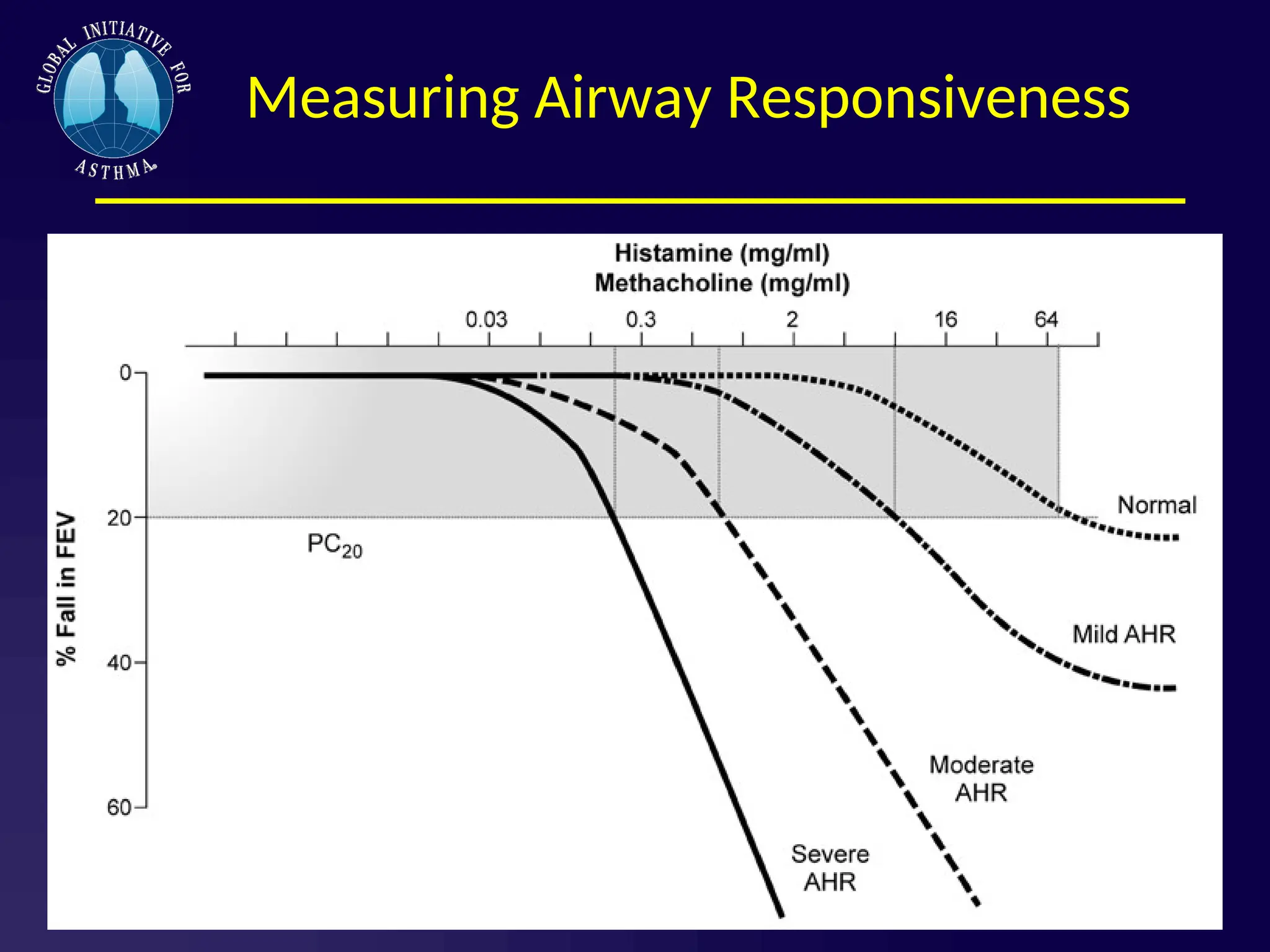
Measurement of airway responsiveness
Measurements of allergic status to identify risk
factors
Extra measures may be required to diagnose asthma
in children 5 years and younger and the elderly
23.
Is it Asthma?
Recurrent episodes of wheezing
Troublesome cough at night
Cough or wheeze after exercise
Cough, wheeze or chest tightness after
exposure to airborne allergens or pollutants
Colds “go to the chest” or take more than
10 days to clear
24.
24
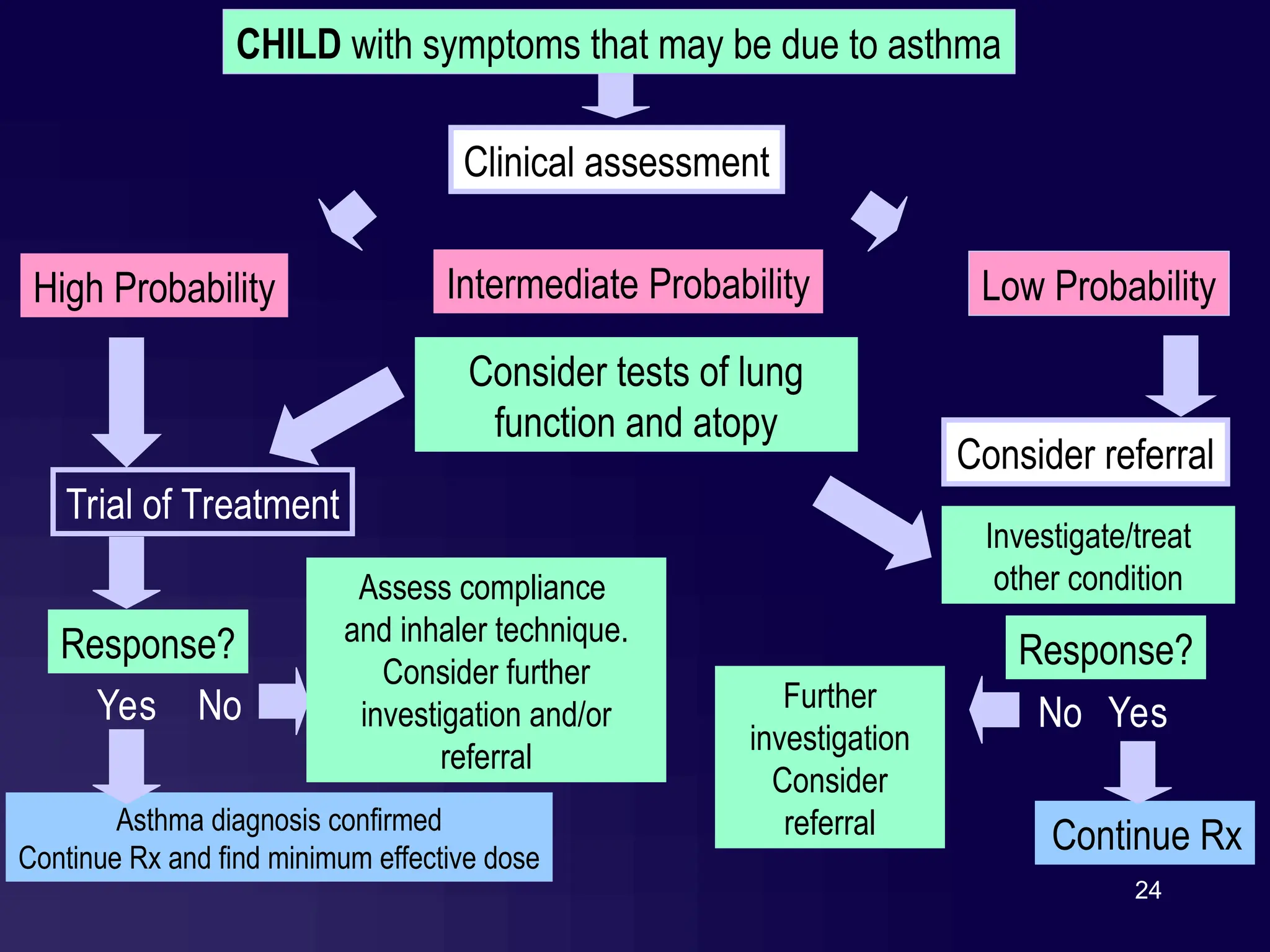
CHILD with symptomsthat may be due to asthma
Clinical assessment
High Probability Low Probability
Intermediate Probability
Yes No
Continue Rx
Response?
Consider referral
Yes
Trial of Treatment
Response?
Asthma diagnosis confirmed
Continue Rx and find minimum effective dose
No
Assess compliance
and inhaler technique.
Consider further
investigation and/or
referral
Consider tests of lung
function and atopy
Investigate/treat
other condition
Further
investigation
Consider
referral
25.
CONFIRM THE DIAGNOSIS
CONFIRMTHE DIAGNOSIS
REVERSIBLE
REVERSIBLE
OBSTRUCTION
OBSTRUCTION
Variability
Variability
POSITIVE BPT
THERAPEUTIC TEST
26.
Other investigations
Tests forairway hyperresponsiveness
. Metacholine
. Exercise
. Mannitol
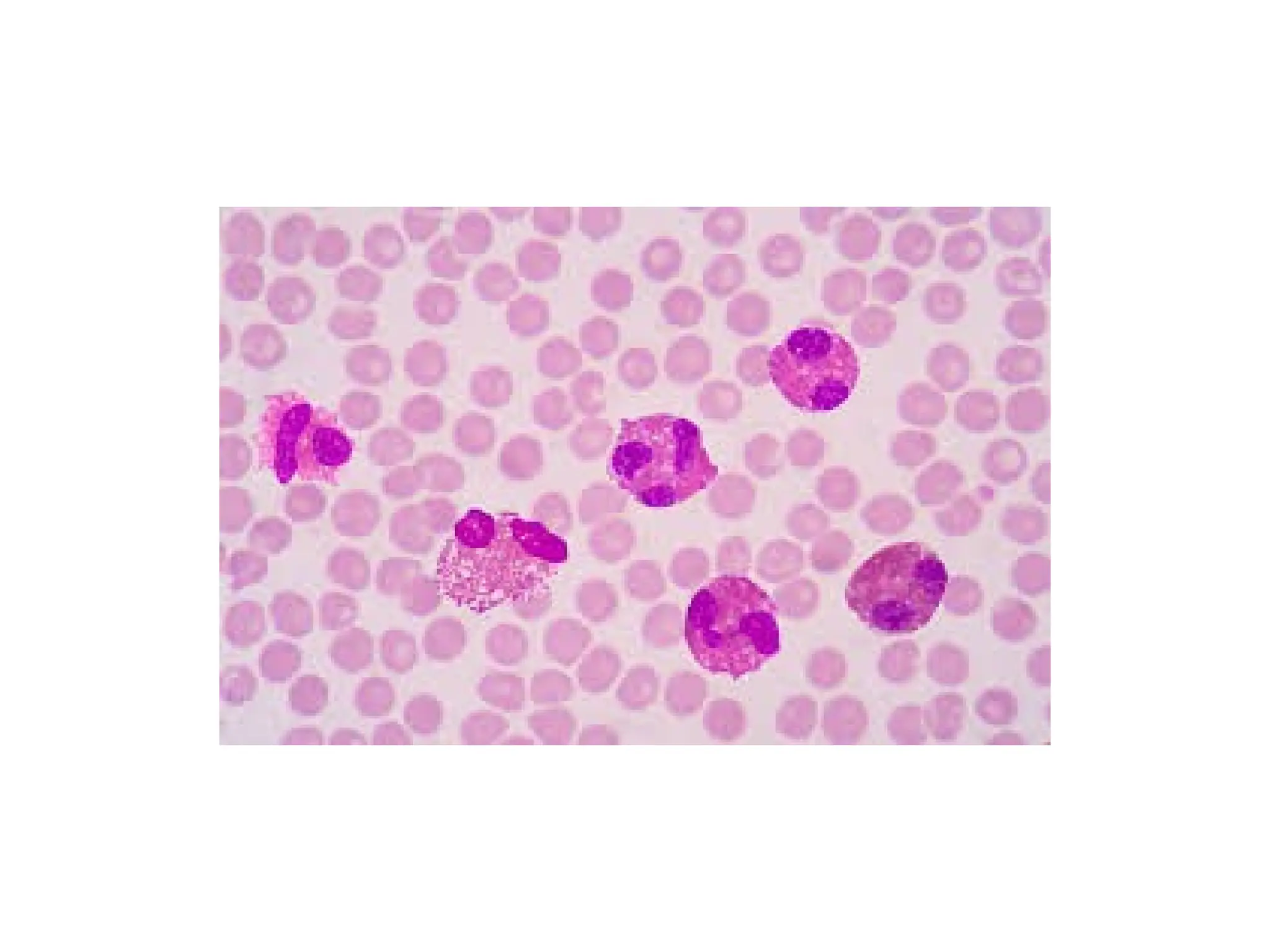
Tests for eosinophilic airway inflammation
. Induced-sputum
. [ FENO]
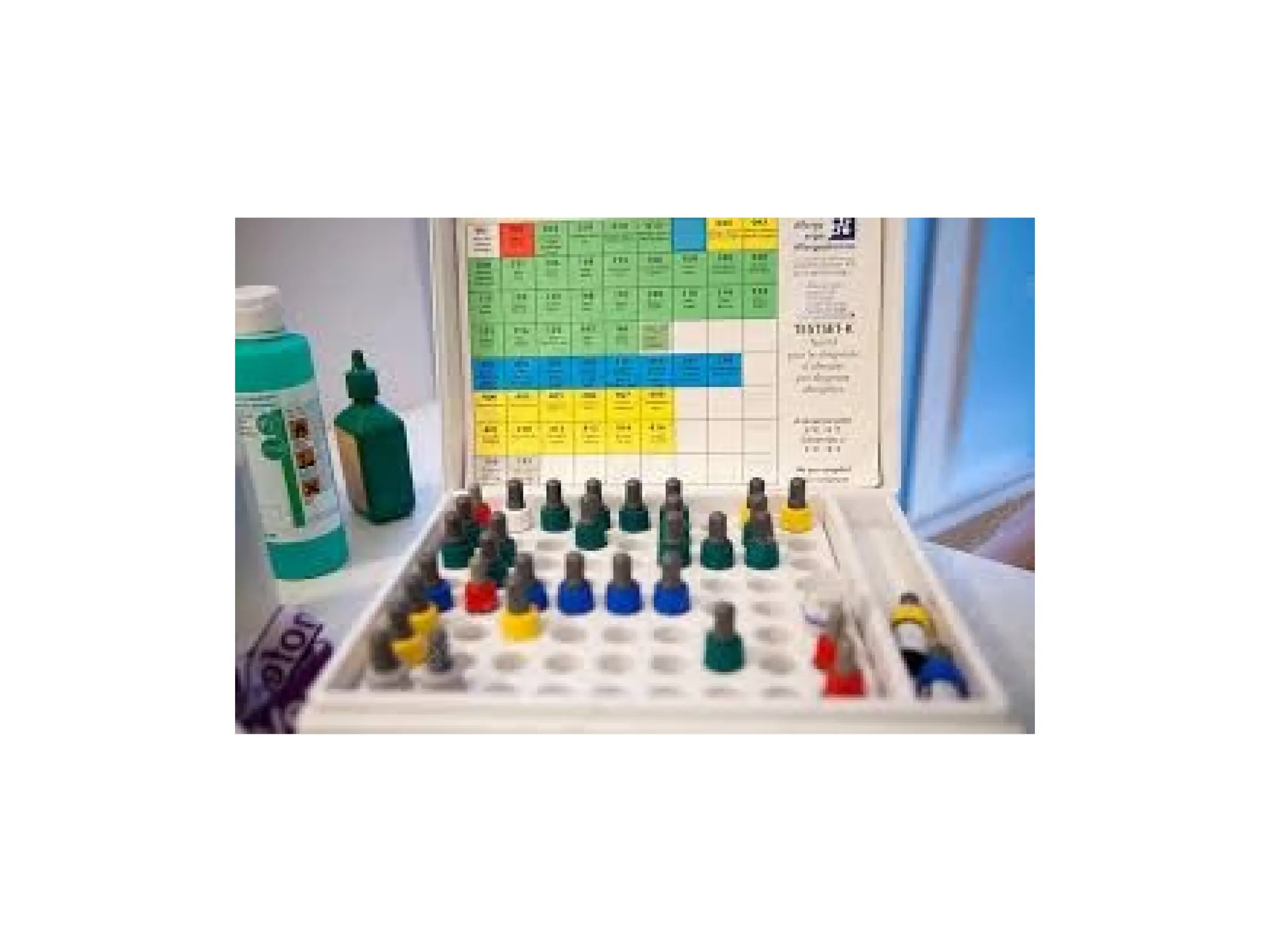
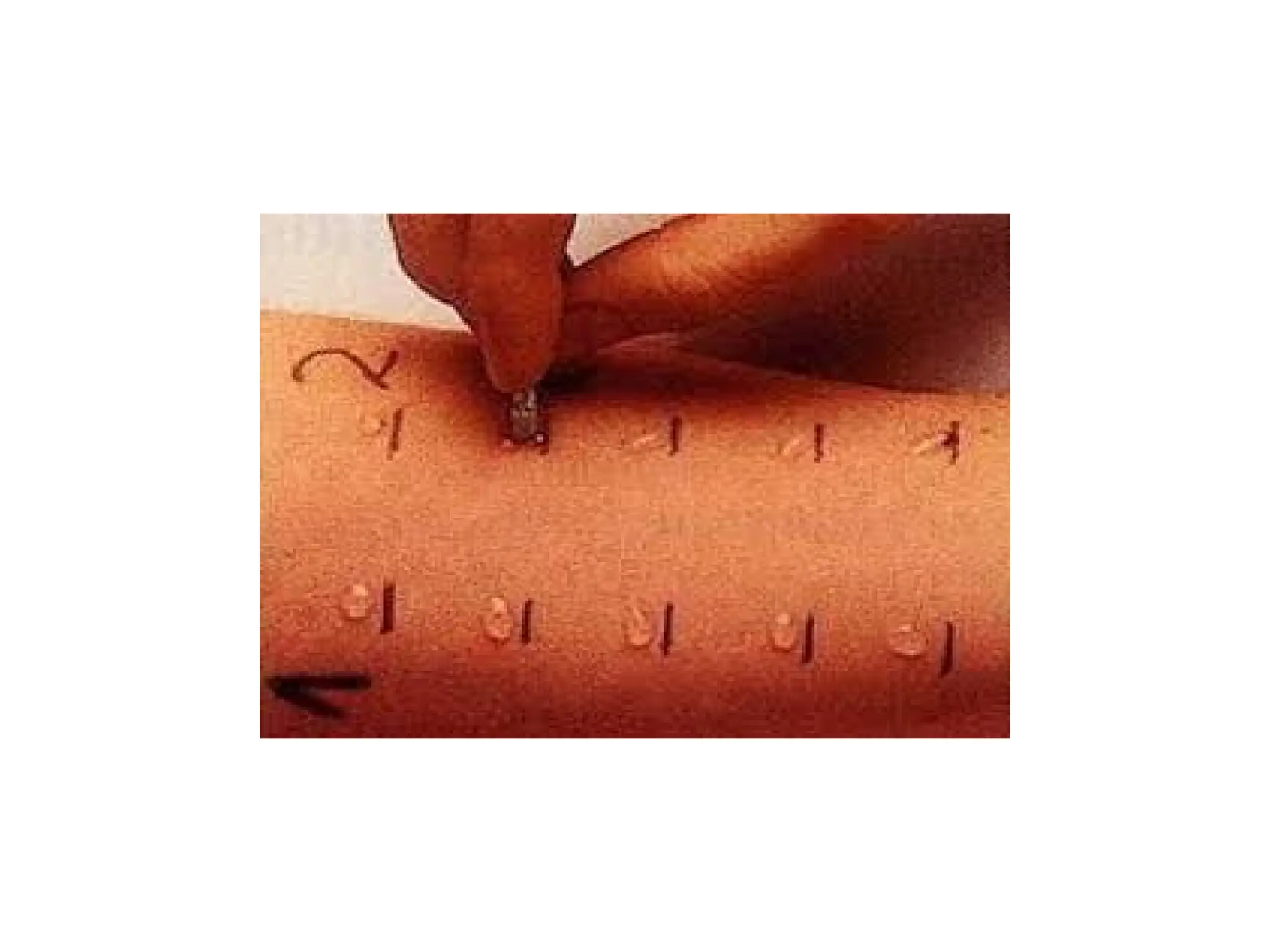
Tests of atopy
. Skin prick tests
. Blood eosinophilia
. RAST
CXR
32.
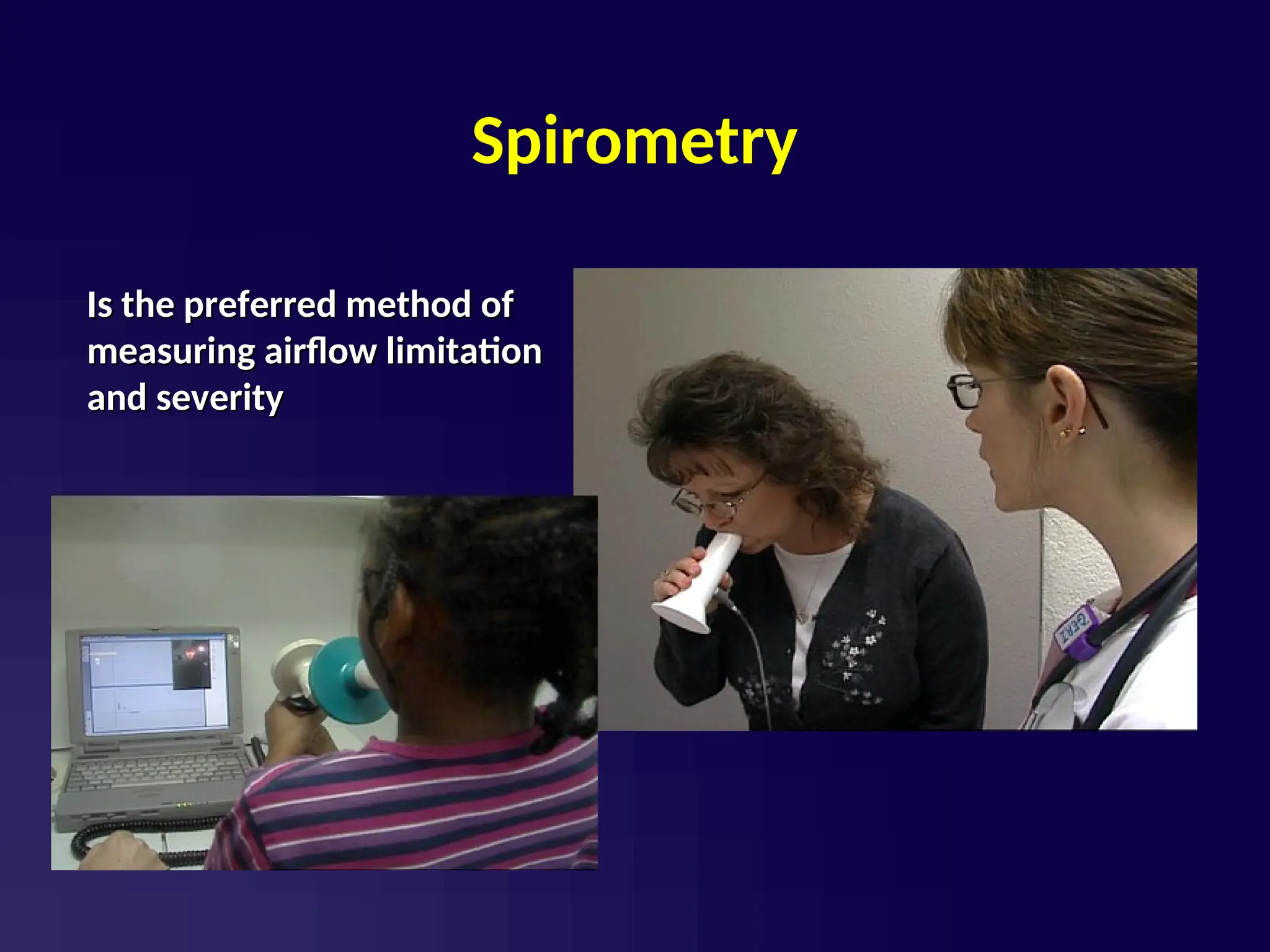
Spirometry
Is the preferredmethod of
Is the preferred method of
measuring airflow limitation
measuring airflow limitation
and severity
and severity
34.
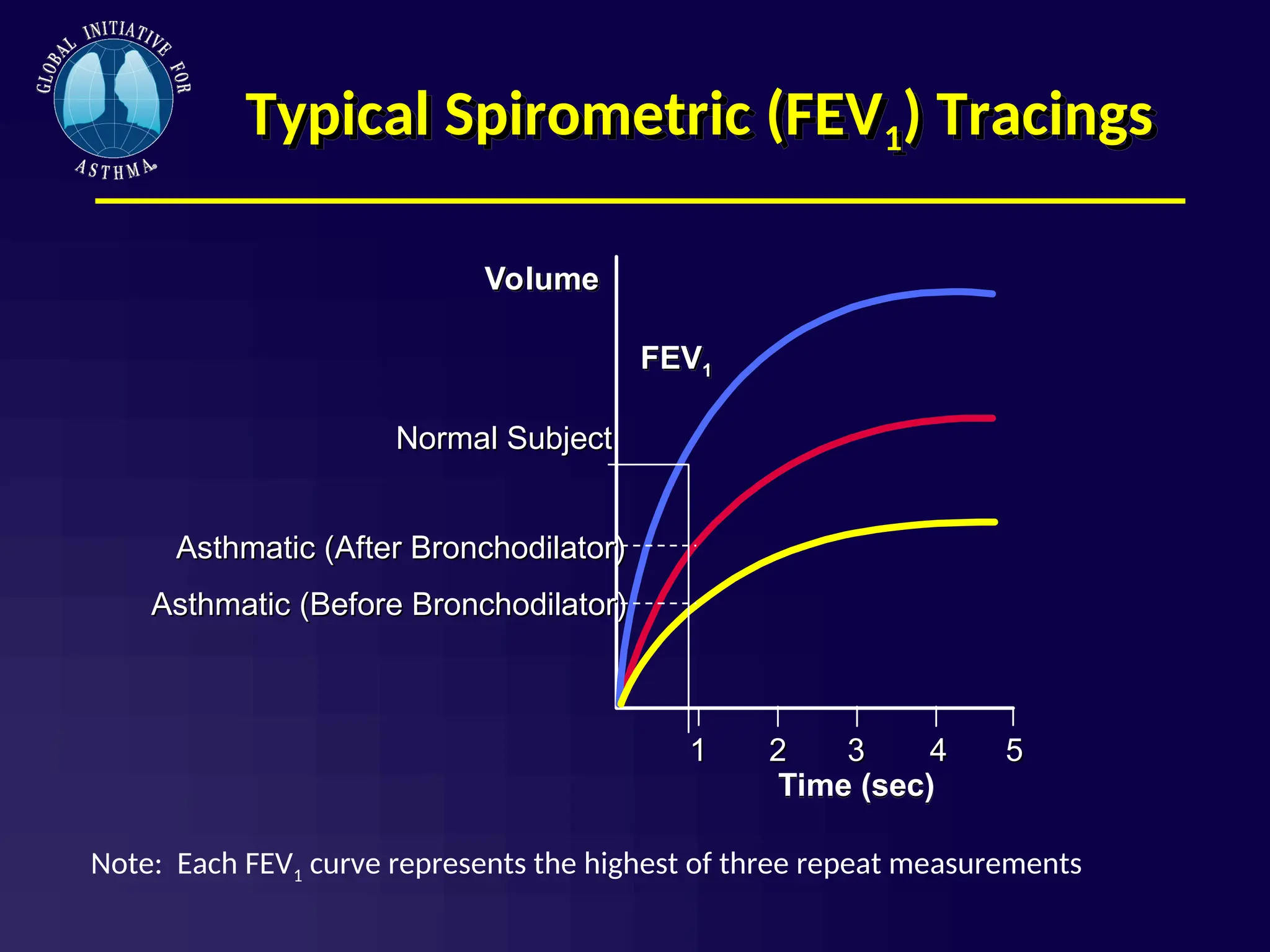
Typical Spirometric (FEV1)Tracings
1
1
Time (sec)
2
2 3
3 4
4 5
5
FEV1
Volume
Normal Subject
Normal Subject
Asthmatic (After Bronchodilator)
Asthmatic (After Bronchodilator)
Asthmatic (Before Bronchodilator)
Asthmatic (Before Bronchodilator)
Note: Each FEV1 curve represents the highest of three repeat measurements
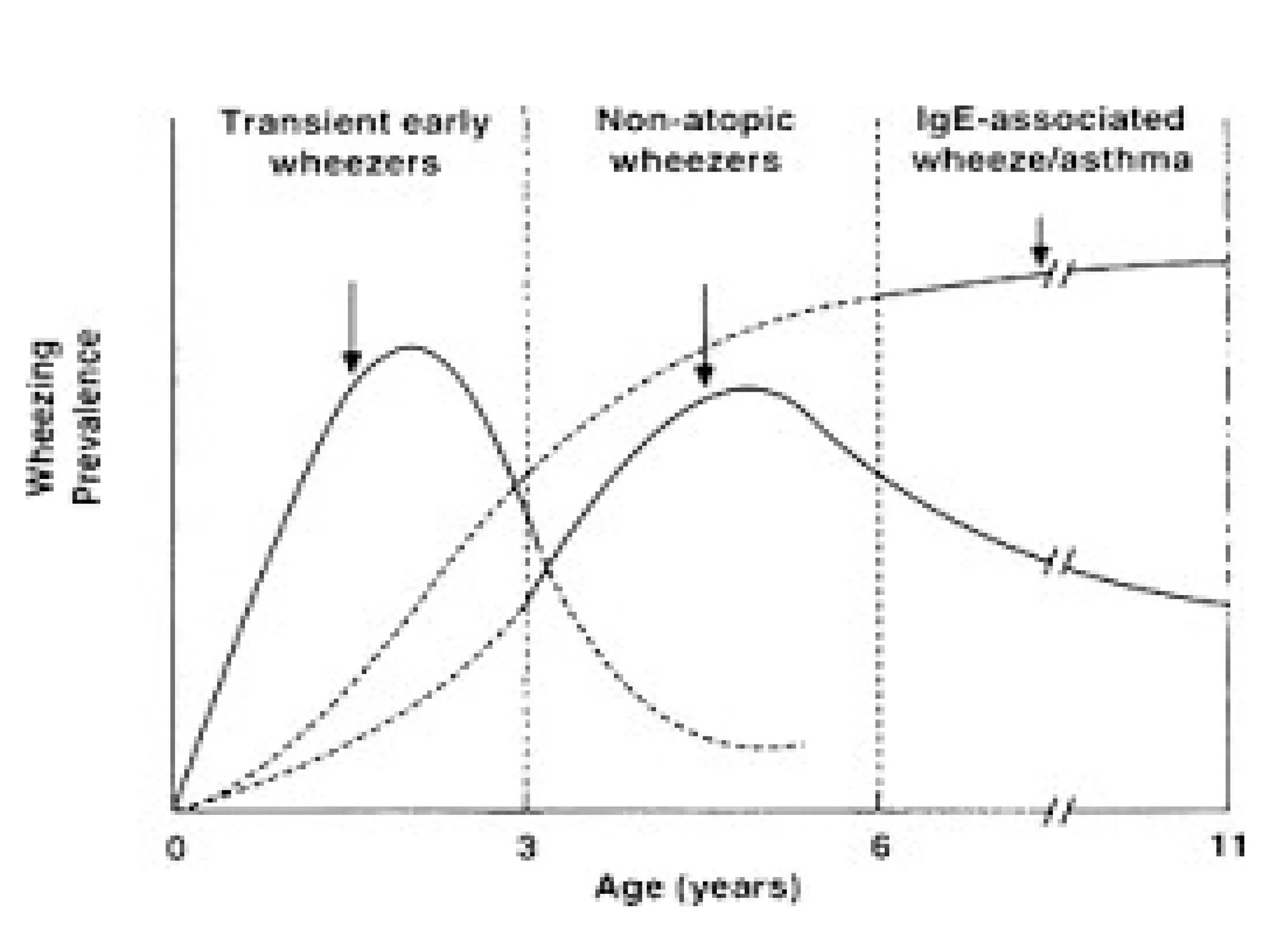
3 categories ofwheezers
(1) Transient early wheezing
. Prematurity
. Parental smoking
. Outgrown by 3 years of age
(2) Persistent early-onset wheezing < 3 years
. No atopy
. No family history of asthma/atopy
. Recurrent viral-induced wheeze
. Outgrown by 12 years
39.
3 categories ofwheezers, continued
(3) Late-onset wheezing/asthma
. Atopic
. Wheeze persists into adulthood
. Airway pathology characteristic of asthma
#2 Script Notes: Asthma is a condition that:
is chronic, meaning that it’s an on-going, long-term condition.
produces recurring episodes of breathing problems called asthma episodes
is potentially life-threatening
can occur at any age
is not contagious, meaning it cannot be spread from one student to another
cannot be cured, but can be controlled
The cause of asthma is unclear. It is probably caused by a mix of genetic and environmental factors.
Note for presenter: Some audiences may need a definition for genetic and environmental factors. Genetic factors are things passed down from your parents. Environmental factors are things in the environment around you that may contribute to the development of asthma.
#11 Script Notes:
Some things can make asthma worse and can initiate the onset of an asthma episode. Not all students with asthma are affected by the same factors, and their sensitivities can change over time.
The most common cause of asthma episodes is colds or other upper airway infections, which is just one more reason to emphasize the importance of good handwashing.
Some children only experience asthma symptoms during or after physical activity. This is referred to as exercise induced asthma (EIA).
Changes in weather and temperature can affect some students’ asthma as well.
Strong physical expressions of feelings, such as crying or laughing hard, or yelling, can cause some students’ asthma to flare up.
#12 Script Notes:
Classroom pets like rabbits, hamsters, gerbils, and parakeets may cause some students to have an asthma attack and should be removed.
Most homes and schools in humid areas have dust mites. They are found in carpets, clothes, stuffed toys and fabric-covered items.
Droppings, saliva, and the body parts of cockroaches and other pests can cause asthma attacks for some students.
Some students’ asthma flares up when grass is cut at their school, especially if their classroom window is left open.
Mold grows where moisture is present. All molds that are found growing inside a school building should be removed immediately.
Note to presenter: The information found in this slide is found in the following sources:
www.epa.gov/iaq/asthma/index.html,
www.epa.gov/mold/mold_remediation.html,
www.cdc.gov/mold/faqs.htm and
www.aafa.org.
http://breatherville.org/breatheatschool/ has a Home, School & Play resource which describes these triggers and how to remediate them.
#13 Script Notes:
Tobacco smoke can actually contribute to causing asthma, in addition to causing many students with asthma to experience asthma symptoms.
Outdoor air pollution, including diesel exhaust from school buses, can cause asthma episodes. Poor outdoor air quality can also be a problem.
Scented products, such as perfumes, body creams, cause some students’ asthma to flare-up.
Some classrooms, such as art rooms, science labs, and career and technical education classrooms, have strong odors from chemicals used. Strong fumes or odors from chemicals such as cleaning products, pesticides, and paint can cause some students’ to have an asthma episode.
#14 Script Notes: Three things can happen during an asthma episode:
Swelling of the airways
Clogging- the mucus blocks the airways and thus allows less air to pass through the airways
Squeezing- the air passages are squeezed together by the muscles that surround the outside of each airway.
This combination of swelling, clogging, and squeezing dramatically reduces the size of the airways.
#32 Spirometer is the method of measuring lung function. Spirometry is a physiological test that measures how an
individual inhales or exhales volumes of air as a function of
time. forced vital capacity (FVC), which is the volume delivered
during an expiration made as forcefully and completely as
possible starting from full inspiration, and the forced expiratory
volume (FEV) in one second, which is the volume
delivered in the first second of an FVC manoeuvre. Breathe deepy and breath out sthrongly
![Other investigations
Tests for airway hyperresponsiveness
. Metacholine
. Exercise
. Mannitol
Tests for eosinophilic airway inflammation
. Induced-sputum
. [ FENO]
Tests of atopy
. Skin prick tests
. Blood eosinophilia
. RAST
CXR](https://image.slidesharecdn.com/anoverviewofchildhoodasthma-250819170349-ef97d7cf/75/An-overview-of-childhood-asthma-pp-presentation-26-2048.jpg)