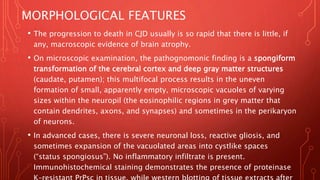
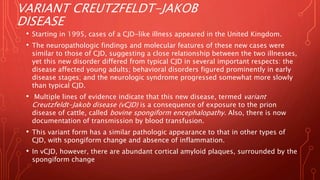
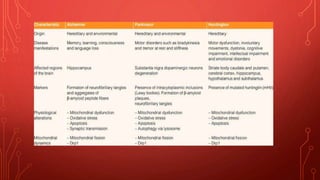
The document discusses neurodegenerative diseases including Alzheimer's disease, Parkinson's disease, and prion disease. It notes that neurodegenerative diseases are characterized by the progressive loss of neurons affecting functional groups. Alzheimer's disease is the most common cause of dementia and involves the accumulation of amyloid beta and tau proteins forming plaques and tangles respectively. The pathogenesis involves these proteins as well as inflammatory reactions. Morphological features include cortical atrophy, enlarged ventricles, neuritic plaques, and neurofibrillary tangles in neurons.

![• Over time, this self-amplifying process leads to the accumulation
of a high burden of pathogenic PrPsc molecules in the brain.
• Certain mutations in the gene encoding PrPc (PRNP) accelerate the
rate of spontaneous conformational change; these variants are
associated with early-onset familial forms of prion disease
(familial Creutzfeldt-Jakob disease [fCJD]).
• PrPc also may change its conformation spontaneously (but at an
extremely low rate), accounting for sporadic cases of prion
disease (sporadic Creutzfeldt-Jakob disease [sCJD]).
• Accumulation of PrPsc in neural tissue seems to be the cause of
cell injury, but the mechanisms underlying the cytopathic changes
and eventual neuronal death are still unknown.](https://image.slidesharecdn.com/alzheimerdisease-230216023451-a3101be0/85/Alzheimer-disease-pptx-22-320.jpg)