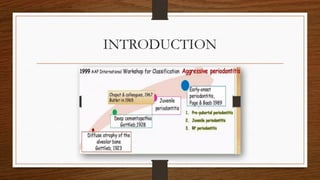
This presentation showcases the Introduction of Aggressive periodontitis its classification and how as a periodontist and general practitioner one should approach towards planning treatment for this disease entity
• Aggressive periodontitisis defined as group of rare, severe, rapidly progressing forms of
periodontitis characterized by an early age of clinical manifestation and a distinctive
tendency for cases to aggregate in families.
- Jan Lindhe
5.
Baer’s 7 Criteria
•Baer proposed 7 criteria to define the disease:
• 1. Age of onset
• 2. Sex ratio
• 3. Familial background
• 4. Lack of relationship between etiologic factors and periodontal pocket
• 5. Distinctive roentgenographic pattern of alveolar bone loss
• 6. Rate of progression
• 7. Primary teeth
6.
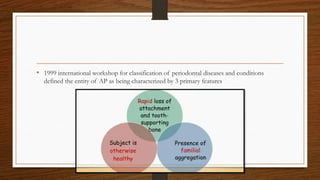
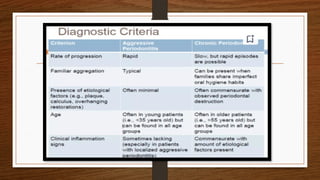
• 1999 internationalworkshop for classification of periodontal diseases and conditions
defined the entity of AP as being characterized by 3 primary features
7.
• Workshop definedseveral secondary features:
• 1. Amount of microbial deposits are inconsistent with the severity of periodontal tissue
destruction.
• 2. Elevated proportions of A.a
• 3. Hyper-responsive macrophage phenotype, including elevated production of PGE2, and
IL-β in response to bacterial endotoxins.
• 4. Progression of attachment loss/bone loss may be self arresting
8.
American Academy ofPeriodontology Workshop, 1999
Aggressive Periodontitis
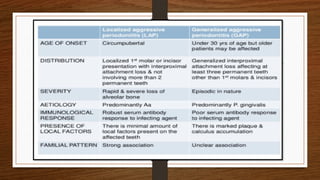
Localized Aggressive Generalized Aggressive
• Age ofonset around puberty
• Clinically its characterized as having;
• “localized molar/incisor presentation with interproximal attachment loss on at least
two permanent teeth, one of which is a first molar, and involving no more than two
teeth other than first molar and incisors”.
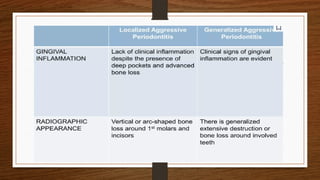
• Amount of plaque on the affected teeth is minimal, which seems inconsistent with the
amount of periodontal destruction present.
• Evidence suggests that the rate of bone loss is 3-4 times faster than in chronic periodontitis
11.
• Increased mobilityof the first molars
• Sensitivity of the root surfaces to thermal and tactile stimuli
• Deep, dull, radiating pain during mastication, probably because of irritation of the
supporting structures by mobile teeth and impacted food
• Periodontal abscess formation may occur along with regional lymph node enlargement
• Vertical lossof alveolar bone around the first molars and incisors
• Beginning around puberty in otherwise healthy teenagers, is a classic diagnostic sign of LAP
• Arc shaped loss of alveolar bone extending from distal surface of the second premolar to
the mesial surface of the second molar
• Usually affectsindividuals under the age of 30, but older patients also may be affected
• Evidence suggests that persons affected with GAP produces poor antibody response to the
pathogens present
• Characterized by;
• “generalized interproximal attachment loss affecting at least three permanent teeth
other than first molars and incisors”
• Radiographs often show bone loss that has progressed since the previous evaluation
17.
• Quantitatively, theamount of plaque seems inconsistent with the amount of periodontal
destruction
• Qualitatively, P. gingivalis, A. actinimycetemcomitans and T. forsythia are frequently detected
in the plaque that is present
18.
• Two gingivaltissue responses can be found:
• 1. Severe, acutely inflamed tissue, often proliferating, ulcerated and fiery red. Bleeding may
occur spontaneously or on slight stimulation
• 2. Gingival tissue may appear pink, free of inflammation and occasionally with some degree
of stippling, although the last feature may be absent
20.
• Despite theapparently mild clinical gingival appearance, deep pockets can be demonstrated
by probing
• Systemic manifestations such as weight loss, mental depression and general malaise.
• Generalized aggressive periodontitis patients must have their medical histories updated and
reviewed.
Microbiologic Factors
• A.ahas been implicated as primary pathogen with associated with the disease.
• According to Tonneti & Mombelli, this link is based on following evidence:
• 1. A.a found in high frequency in lesions characteristics of LAP.
• 2. Sites with evidence of disease progression often shows elevated levels of A.a.
• 3. Many patients with the clinical manifestations of LAP have significantly elevated serum antibody
titers towards A.a.
• 4. Clinical studies shows co-relation between reduction in subgingival load of A.a. during treatment
and a successful clinical response.
• 5. A.a. produces a number of virulence factors that may contribute to the disease process.
28.
• Another studyfound elevated levels of P.gingivalis, P. intermedia, F. nucleatum etc.
• SEM analysis of LAP have revealed bacterial invasion of connective tissue.
29.
Immunologic Factors
• Humanleucocyte antigen (HLA), which regulates immune responses, have been evaluated as
candidate markers for aggressive periodontitis.
• Patients with aggressive periodontitis display functional defects of PMNs, monocytes or both.
• These defects can either impair chemotactic attractions or PMN to the site of infection or
their ability to phagocytose and kill microorganisms.
• Hyper responsiveness of monocytes from LAP patients with respect to their production of
PGE2 in response to LPS.
• This hyper responsive phenotype could lead to increase CT destruction or bone loss due to
excessive production of these catabolic factors.
30.
• Additionally, poorlyfunctional inherited forms of monocyte FcγRII, the receptor for
human IgG2 antibodies, have been shown to be disproportionately present in patients with
LAP.
• These PMN and monocyte defects may be induced by the bacterial infection or genetic in
origin.
31.
Environmental Factors
• Theamount and duration of smoking are variables that can influence the extent of
destruction seen in young patients.
• Patients with GAP who smoke have more affected teeth and more loss of clinical
attachment than non-smoking patients with GAP.
32.
Genetic Factors
• Allindividuals are not equally susceptible to aggressive periodontitis.
• Familial pattern of alveolar bone loss, which have implicated genetic implications.
• LAP suggests that a major gene plays a role in this disease, which is transmitted
through an autosomal dominant mode of inheritance.
• Familial clustering of neutrophil abnormalities seen in LAP.
• The antibody response to periodontal pathogens, particularly A.a., is under genetic
control and that the ability to mount high titers of specific, protective antibody
against A.a may be race dependent.
• Early detectionis critically important in the treatment of aggressive periodontitis.
• Because preventing further destruction is more preventable than attempting to regenerate
lost supporting tissues.
• At the intial diagnosis it is helpful to obtain any previously taken radiographs to assess the
rate of progression of disease
• Educate the patient about the disease, including causes and risk factors.
35.
Management of AggressivePeriodontitis
Non surgical therapy
Antimicrobial
therapy, LDD
Full mouth
disinfection
Host modulation
therapy
Conventional
periodontal
therapy
36.
Non-Surgical Therapy
• Itsclear effect on aggressive periodontitis is less clear.
• GAP responds to PMPR in short term (upto 6 months)
• However, after 6 months relapse and disease progression has been reported (Gunsolley et
al 2007, Haas et al 2008)
• PMPR reduced the total subgingival bacterial count and some gram –ve bacteria but no
periodontal pocket became free of A.a.
37.
Anti-microbial Therapy
• Systemictetracycline (250 mg of tetracycline hydrochloride 4 times/day for at least 1 week)
in conjunction with mechanical therapy.
• Tetracycline resistant A.a: Amoxicillin + Metronidazole
Ciprofloxacin + Metronidazole
• Chlorhexidine should be prescribed to enhance better plaque control
39.
Full Mouth Disinfection
•The concept was given by Quirynen et al:
• 1. Full mouth debridement completed in two appointments within 24 hour period.
• 2. Tongue is brushed with chlorhexidine gel (1%) for 1 minute
• 3. Mouth is rinsed with chlorhexidine solution (0.2%) for 2 minutes.
• 4. Periodontal pockets are irrigated with chlorhexidine solution (1%)
• Significant reduction in pathogens up to 8 months after therapy was recorded
Periodontal Maintenance
• Whenthe patients with AP are transferred to maintenance care, their periodontal conditions
must be stable.
• Frequent maintenance visits appears to be the most important factors in the control of
disease and the success of treatment.
• The duration between these recall visits is usually short during the first period after the
patients completion of therapy, generally no longer than 3 months intervals.
• Monitoring as frequently as every 3-4 weeks may be necessary when the disease is thought
to be active.