MANAGEMENT OF METASTATICSOFT
MANAGEMENT OF METASTATIC SOFT
TISSUE SARCOMA AND RECENT
TISSUE SARCOMA AND RECENT
ADVANCES
ADVANCES
Dr. G. Anitha
Dr. G. Anitha
PG in Surgical oncology
PG in Surgical oncology
Department of Surgical oncology
Department of Surgical oncology
Government Royapettah Hospital
Government Royapettah Hospital
PROF R. RAJARAMAN UNIT
2.
METASTATIC STS
METASTATIC STS
50% develop metastases
50% develop metastases
Most common Site of
Most common Site of
metastases: lung
metastases: lung
Other sites: liver, lymph nodes
Other sites: liver, lymph nodes
3.
Myxoid liposarcoma
Myxoidliposarcoma is an exception
is an exception
which metastatize to areas containing
which metastatize to areas containing
fat
fat
Isolated soft tissue masses in pelvis,
Isolated soft tissue masses in pelvis,
retroperitoneum, mediastinum,
retroperitoneum, mediastinum,
paraspinal and subcutaneous soft
paraspinal and subcutaneous soft
tissue and bone marrow
tissue and bone marrow are hallmark
are hallmark
of this subtype
of this subtype
4.
Soft tissue sarcomaswith
Soft tissue sarcomas with
predilection for
predilection for lymph node
lymph node
mets
mets
Rhabdomyosarcoma
Rhabdomyosarcoma
Clear cell sarcoma
Clear cell sarcoma
Epitheloid sarcoma
Epitheloid sarcoma
Synovial sarcoma
Synovial sarcoma
Angiosarcoma
Angiosarcoma
Incidence of nodal metastases is < 3%
5.
PRESENTATION
PRESENTATION
Synchronous in30%
Synchronous in 30%
80% present within 2 years
80% present within 2 years
Usually asymptomatic until imaging
Usually asymptomatic until imaging
reveals metastases
reveals metastases
Occasionally endobronchial involvement
Occasionally endobronchial involvement
leads to stridor, atelectasis or
leads to stridor, atelectasis or
postobstructive pneumonia
postobstructive pneumonia
6.
Median survival: 12 months
Median survival : 12 months
2yr survival: 20%- 25%
2yr survival: 20%- 25%
Exception is
Exception is alveolar soft part
alveolar soft part
sarcoma
sarcoma where the survival is
where the survival is
prolonged even with metastases
prolonged even with metastases
7.
Treatment is individualised
Treatmentis individualised
based on
based on
patient factors
patient factors
disease factors
disease factors
limitations imposed by prior treatment
limitations imposed by prior treatment
SURGICAL RESECTION OFPULMONARY METS
SURGICAL RESECTION OF PULMONARY METS
Surgical resection is the
Surgical resection is the
cornerstone of treatment
cornerstone of treatment
3yr overall survival rate of 30%- 54%
3yr overall survival rate of 30%- 54%
5yr overall survival rate of 25% -
5yr overall survival rate of 25% -
38%
38%
10.
40%- 80%will have recurrence
40%- 80% will have recurrence after
after
resection
resection
Repeat resection can be done
Repeat resection can be done
Chemotherapy has no survival benefit
Chemotherapy has no survival benefit
in patients with pulmonary mets
in patients with pulmonary mets
irrespective of resection
irrespective of resection
11.
CRITEREA FOR PATIENTSELECTION
CRITEREA FOR PATIENT SELECTION
The primary tumour is controlled
The primary tumour is controlled
or controllable
or controllable
There is no extrathoracic disease
There is no extrathoracic disease
Adequate predicted postoperative
Adequate predicted postoperative
pulmonary reserve
pulmonary reserve
Complete resection of all disease
Complete resection of all disease
appears possible
appears possible
Resection can be done even if there are
multiple ipsilateral or bilateral mets
12.
CONTRAINDICATIONS FOR RESECTION
CONTRAINDICATIONSFOR RESECTION
Poor pulmonary reserve indicated by
Poor pulmonary reserve indicated by
predicted postop FEV1 <0.8L or <35%
predicted postop FEV1 <0.8L or <35%
predicted postop DLCO <40%
predicted postop DLCO <40%
hypercarbia >45mm
hypercarbia >45mm
hypoxemia <60mm
hypoxemia <60mm
Presence of hilar and mediastinal
Presence of hilar and mediastinal
lymphadennopathy
lymphadennopathy
Presence of malignant pleural effusion
Presence of malignant pleural effusion
13.
PROGNOSTIC FACTORS
PROGNOSTIC FACTORS
Disease free interval > 1 year
Disease free interval > 1 year
Number of nodules < 3 nodules
Number of nodules < 3 nodules
Low grade histology
Low grade histology
Complete resection
Complete resection
Favourable
factors
Unfavourable factors
Age > 50yrs
Histologies like liposarcoma, MPNST
14.
TYPE OF SURGICALRESECTION
TYPE OF SURGICAL RESECTION
Wedge excision with
Wedge excision with
negative margin
negative margin
adequate for isolated
adequate for isolated
pulmonary mets
pulmonary mets
Lobectomy or
Lobectomy or
pneumonectomy if mets
pneumonectomy if mets
is adjacent to
is adjacent to
pulmonary artery , vein,
pulmonary artery , vein,
or major bronchus
or major bronchus
15.
APPROACHES FOR UNLATERALMETS
APPROACHES FOR UNLATERAL METS
VATS Vs Thoracotomy
VATS Vs Thoracotomy
Advantages of VATS
Advantages of VATS: less pain
: less pain
short hospital stay
short hospital stay
reoperation is
reoperation is
easi
easier
er
Dis advantages:
lesions < 5mm will be
missed
Only solitary
peripheral lesions
are amenable
16.
APPROACHES FOR BILATERALMETS
APPROACHES FOR BILATERAL METS
Staged thoracotomy
Staged thoracotomy
(4-8 weeks interval)
(4-8 weeks interval)
Median sternotomy
Median sternotomy
Adv: Less postop pain
Adv: Less postop pain
Dis adv: Exposure
Dis adv: Exposure
suboptimal
suboptimal
Clamshell approach
Clamshell approach
Adv: execellent exposure
Adv: execellent exposure
Disadv: more postop pain
Disadv: more postop pain
Probe is introducedinto the tumour under
image guidance
High frequency alternating current
is transmitted through tip
Excitation of molecules
Heating of tissues
Coagulative necrosis
20.
INDICATIONS FOR RFA
INDICATIONSFOR RFA
Elderly patients
Elderly patients
Poor surgical candidates
Poor surgical candidates
Other options have been
Other options have been
exhausted
exhausted
21.
PRE REQUISITES
PRE REQUISITES
Number of lesions should be < 4
Number of lesions should be < 4
Size of lesion should be < 3cm in diameter
Size of lesion should be < 3cm in diameter
Lesion should not be adjacent to hilar or
Lesion should not be adjacent to hilar or
vascular structures
vascular structures
Emphysematous blebs should not be
Emphysematous blebs should not be
present around the lesion
present around the lesion
STEREOTACTIC BODY RADIOTHERAPY
STEREOTACTICBODY RADIOTHERAPY
Focussed radiation beams are delivered
Focussed radiation beams are delivered
exclusively around tumour nidus
exclusively around tumour nidus
High dose RT in single session or few
High dose RT in single session or few
fractionated sessions
fractionated sessions
Can be given both with curative and
Can be given both with curative and
palliative intent
palliative intent
Indicated in tumours < 5 cm and in
Indicated in tumours < 5 cm and in
patients who are poor candidates for
patients who are poor candidates for
surgery
surgery
24.
CONTRAINDICATIONS
CONTRAINDICATIONS
Lesions closeto airways
Lesions close to airways
Centrally located tumours
Centrally located tumours
Lesions close to mediastinal
Lesions close to mediastinal
structures
structures
26.
A high potentbiological dose of
radiation is delivered to the tumor.
Multiple radiation beams directed to the
tumor.
Respiratory gating technology
Respiratorygating technology
Fiducials act as localizing and tracking
devices.
Accurate and precise tumor
localization at the time of
radiation simulation.
29.
ADVANTAGES
ADVANTAGES
Can beused in patients with
Can be used in patients with
emphysema and COPD
emphysema and COPD
Patients who are extensively
Patients who are extensively
pretreated with chemotherapy which
pretreated with chemotherapy which
affects the pulmonary reserve
affects the pulmonary reserve
High local control rate is achieved
High local control rate is achieved
Minimal complications
Minimal complications
30.
There isno current consensus
There is no current consensus
about the optimal dosage
about the optimal dosage
Though better local control and
Though better local control and
low toxicity are observed in various
low toxicity are observed in various
trials, assessment of survival is
trials, assessment of survival is
not well studied
not well studied
Future trials are expected in this
Future trials are expected in this
regard
regard
31.
CHEMOTHERAPY
CHEMOTHERAPY
Single agent
Singleagent doxorubicin
doxorubicin is the reasonable
is the reasonable
first line option for palliative chemo
first line option for palliative chemo
For patients who progress or relapse after
For patients who progress or relapse after
response to doxorubicin,
response to doxorubicin, ifosfamide
ifosfamide is
is
indicated as 2
indicated as 2nd
nd
line drug
line drug
Single agent chemo is better than
Single agent chemo is better than
combination chemo
combination chemo
Various trials revealed no survival benefit
Various trials revealed no survival benefit
with combination chemo
with combination chemo
Gemcitabine
Gemcitabine and
and docetaxel
docetaxel combination
combination
is useful in leiomyosarcomas
is useful in leiomyosarcomas
32.
OTHER PALLIATIVE MEASURES
OTHERPALLIATIVE MEASURES
Endobronchial laser debulking to
Endobronchial laser debulking to
establish airway patency in tumours
establish airway patency in tumours
obstructing main stem bronchus
obstructing main stem bronchus
EBRT for low grade hemoptysis
EBRT for low grade hemoptysis
Bronchial artery embolization for
Bronchial artery embolization for
severe hemoptysis
severe hemoptysis
MOLECULAR GENETIC TESTING
MOLECULARGENETIC TESTING
Sarcomas with specific genetic alterations
Sarcomas with specific genetic alterations
(simple karyotype)
(simple karyotype)
chromosomal translocations
chromosomal translocations
point mutations
point mutations
Sarcomas with non specific genetic
Sarcomas with non specific genetic
alterations
alterations
(complex unbalanced karyotypes)
(complex unbalanced karyotypes)
37.
Useful indiagnosis of certain
Useful in diagnosis of certain
subtypes of STS where morphological
subtypes of STS where morphological
and IHC findings are equivocal
and IHC findings are equivocal
To predict prognosis
To predict prognosis
Identification of fusion genes aid in
Identification of fusion genes aid in
developing targeted therapies
developing targeted therapies
38.
MOLECULAR IMAGING
MOLECULAR IMAGING
Imaging the key molecules and molecular
Imaging the key molecules and molecular
events that are fundamental to the
events that are fundamental to the
development and progression of cancer
development and progression of cancer
Nuclear based imaging techniques are
Nuclear based imaging techniques are
used mainly PET scan
used mainly PET scan
F18 labelled FLT (deoxy fluoro thymidine)
F18 labelled FLT (deoxy fluoro thymidine)
PET is currently under investigation for
PET is currently under investigation for
STS
STS
39.
F18 FLUORO DEOXYTHYMIDINE PET SCAN
F18 FLUORO DEOXY THYMIDINE PET SCAN
F18 labelled FLT
F18 labelled FLT
FLT monophosphate
FLT monophosphate
Thymidine kinase activity is more in
Thymidine kinase activity is more in
malignant cells
malignant cells
Uptake corresponds to proliferation index
Uptake corresponds to proliferation index
Useful in evaluating response to therapy
Useful in evaluating response to therapy
rather than in diagnosis
rather than in diagnosis
Thymidine kinase
NEAR INFRA REDOPTICAL IMAGING
NEAR INFRA RED OPTICAL IMAGING
Consists of imaging hardware for visualisation
if near infrared light couple with iv injected
chemical probes that allow in vivo detection of
specific protease activity
44.
OPTICAL IMAGING
OPTICAL IMAGING
Useful to detect micrometastases
Useful to detect micrometastases
Response assessment after
Response assessment after
chemotherapy
chemotherapy
Aids in developing targeted therapies
Aids in developing targeted therapies
Recently tried in detection of
Recently tried in detection of
microscopic residual sarcoma during
microscopic residual sarcoma during
surgery
surgery
Currently this modality is under trial in
mouse model
45.
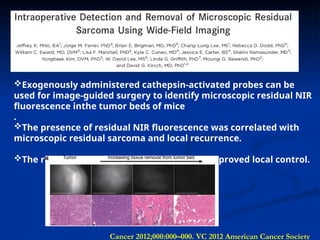
Cancer 2012;000:000–000. VC2012 American Cancer Society
Exogenously administered cathepsin-activated probes can be
used for image-guided surgery to identify microscopic residual NIR
fluorescence inthe tumor beds of mice
.
The presence of residual NIR fluorescence was correlated with
microscopic residual sarcoma and local recurrence.
The removal of residual NIR fluorescence improved local control.
TRABECTEDIN
TRABECTEDIN
ET743, Ecteinascidin743
ET743, Ecteinascidin 743
DNA guanine specific
DNA guanine specific minor groove
minor groove
binding agent
binding agent
Proved to be effective in phase I and II
Proved to be effective in phase I and II
trials in advanced STS
trials in advanced STS
Approved 2
Approved 2nd
nd
line agent in
line agent in myxoid
myxoid
round cell liposarcomas
round cell liposarcomas
Side effect: increase in LFT occasionally
Side effect: increase in LFT occasionally
48.
ANGIOGENESIS INHIBITORS
ANGIOGENESIS INHIBITORS
Angiogenic drive (VEGF)correlates with tumour
Angiogenic drive (VEGF)correlates with tumour
grade
grade
Anecdotal reports of activity with VEGFR inhibitors,
Anecdotal reports of activity with VEGFR inhibitors,
including sorafenib, cediranib
including sorafenib, cediranib
Tumour shrinkage observed in patients with
Tumour shrinkage observed in patients with
alveolar soft part sarcoma (ASPS
alveolar soft part sarcoma (ASPS), a rare disease
), a rare disease
unresponsive to chemotherapy
unresponsive to chemotherapy
VEGFR inhibitor
VEGFR inhibitor pazopanib
pazopanib active against sarcomas
active against sarcomas
in EORTC trial, with exception of liposarcomas
in EORTC trial, with exception of liposarcomas
49.
MDM 2 ANTAGONISTS
MDM2 ANTAGONISTS
MDM2 amplification + in well differentiated and
MDM2 amplification + in well differentiated and
dedifferentiated liposarcomas
dedifferentiated liposarcomas
Nutlin –a prototype had only invitro effectiveness
Nutlin –a prototype had only invitro effectiveness
Spiro oxindoles
Spiro oxindoles (MI-219) binds to MDM2 with high
(MI-219) binds to MDM2 with high
affinity ; under phase I trial
affinity ; under phase I trial
50.
CDK 4 ANTAGONISTS
CDK4 ANTAGONISTS
CDK4amplification is present in well
differentiated and dedifferentiated
liposarcomas
Flavopiridol, seleciclib ( pan CDK inhibitors )
PD0332991 (selective for CDK4,6 ), PI446A05 (Only available
CDK4 selective inhibitor) are under phase I trial
51.
PPAR –
PPAR –γ
γ AGONISTS
AGONISTS
Peroxisome proliferator activated
Peroxisome proliferator activated
receptor
receptor γ
γ regulates the terminal
regulates the terminal
differentiation of adipocytic lineage
differentiation of adipocytic lineage
Troglitazone, rosiglitazone used in
Troglitazone, rosiglitazone used in
phase II trial in high grade liposarcoma
phase II trial in high grade liposarcoma
There is no convincing evidence
There is no convincing evidence
CONCLUSION
CONCLUSION
Lung isthe most common site of metastasis
Lung is the most common site of metastasis
Pulmonary metastatectomy can be done with
Pulmonary metastatectomy can be done with
curative intent if the primary is controllable
curative intent if the primary is controllable
RFA, stereotactic radiotherapy are
RFA, stereotactic radiotherapy are
alternatives to surgery
alternatives to surgery
Single agent chemotherapy is better in the
Single agent chemotherapy is better in the
palliative setting
palliative setting
Trabectedin is the approved 2
Trabectedin is the approved 2nd
nd
line agent in
line agent in
myxoid liposarcoma
myxoid liposarcoma
#2 Extrapulmonary mets are uncommon forms of first mets and usually occurs as late manifestation of widely disseminated disease
#9 Optimal treatment requires understanding the natural history of the disease .surgery renders the patient potentially disease free.recurrence is bços non proliferating tumor cells may not have reached detectable size at the time of initial surgical exploration
#14 Wedge resection leads to isolation of lung parenchyma, threatening both devitalization of tissue as well as rendering residual tissue without normal airway capacity to clear secretions and avoid infections.in general, pneumonectomy should be avoided unless absoluteky necessary for achieving an R0resection in the absence of alternate therapies
#16 With median sternotomy, exposure to hilar, postr, left lower lung fields are inadequate
#28 The software is integrated in the 4D CT machine. And strike zone is defined (period in the breathing cycle where the tumor moves the least) at which time the radiation beam is turned on
#37 Alveolar RMS with mets, PAX7-FOXO1 has favourable prognosis than PAX3-FOXO1
#47 Understanding the molecular pathogenesis of STS has aided in the development of targeted therapies for some subtypes of STS Does not affect transcription of fusion gene FUS-DDIT3 but dissociate the aberrant transcription factor from its target
#51 These agonists bind with PPAR-γ receptor and induce terminal differentiation of normal preadipocytes in human liposarcoma cell lines in vitro