Ear IV
The complicationsof acute and chronic otitis media
Objectives :
y The predisposing factors for complications
y The pathways for spreading the infections beyond
the ear?
y To know the classifications of complications
y To know presentations ,clinical findings
,investigations and management of each complication.
2.
The complications ofacute and
chronic otitis media
Predisposing factors :
y Virulent organisms.
y Chronicity of disease
y Presence of Cholesteatoma and bone erosion.
y Obstruction of natural drainage e.g. by a polyp.
y Low resistance of the patient
Some patients come so late
at 25 years or so
3.
The complications ofacute and
chronic otitis media
Pathways of infection :
y Extension of infection is by bone erosion due to a
cholesteatoma.
y Vascular extension (retrograde thrombophlebitis).
y Congenital dehiscence.
y Fracture lines.
y Round or oval window membrane to the labyrinth.
y Dehiscence due to previous surgery.
Unsafe type
Abnormal skin due to repetitive infections
4.
The complications ofacute and
chronic otitis media
Classification :
Intra-cranial complications.
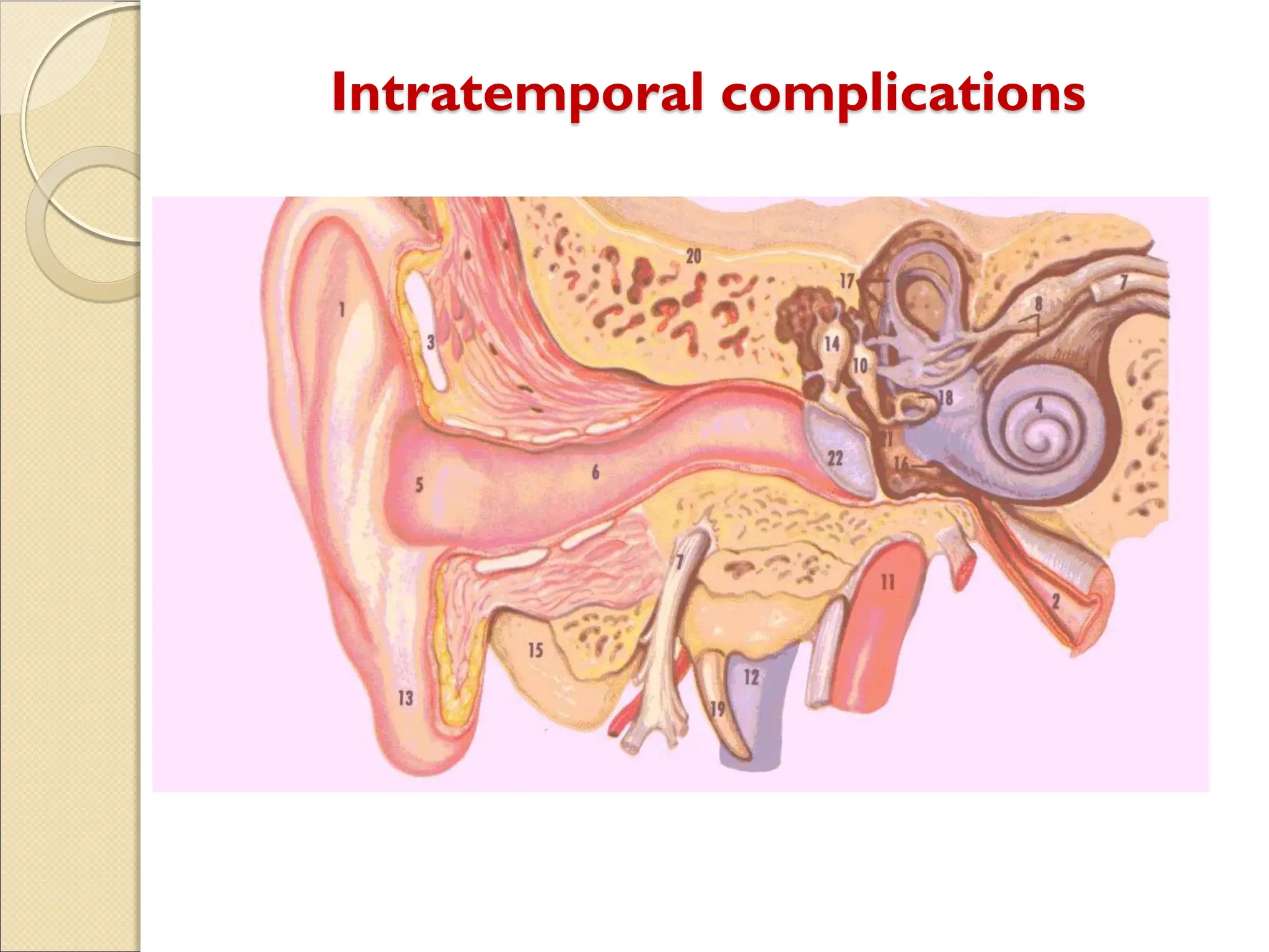
Intratemporal complications.
Extra-cranial complications.
Extradural abscess
y Collectionof pus against the dura.
y middle or posterior cranial fossa.
y Extradural abscess is the commonest
intracranial complication of otitis media.
It starts as extramural abscess then might
progress and become subdural or other type of
complication
8.
Extradural abscess
Clinical Picture:
Persistent headache on the side of otitis media.
Pulsating discharge.
Fever
Asymptomatic (discovered during surgery) Rare
9.
Extradural abscess
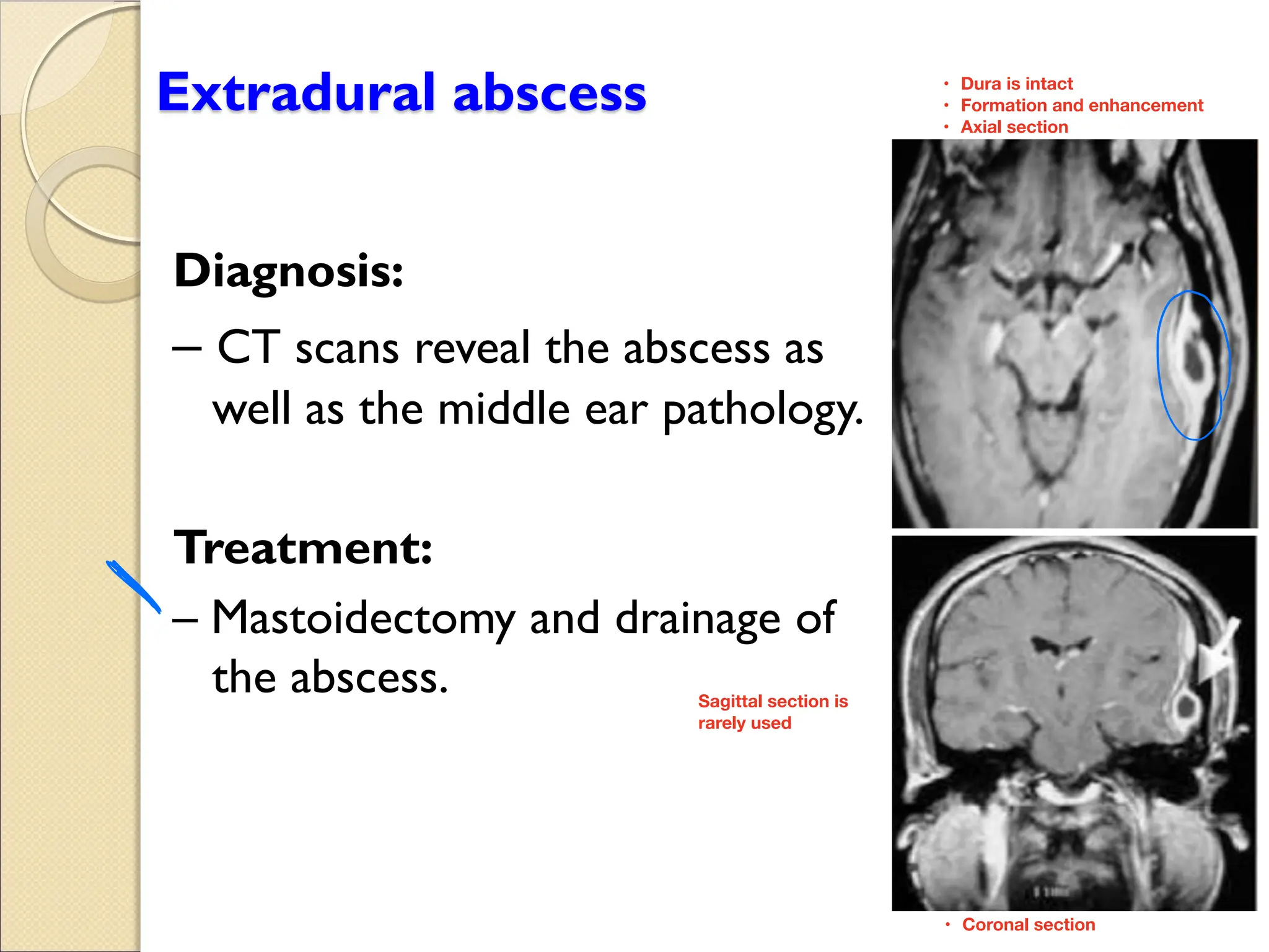
Diagnosis:
CT scansreveal the abscess as
well as the middle ear pathology.
Treatment:
Mastoidectomy and drainage of
the abscess.
o
Dura is intact
•
Formation and enhancement
•
Axial section
•
Coronal section
•
Sagittal section is
rarely used
10.
Subdural abscess
Definition :
Collectionof pus between the dura and the
arachnoid.
It’s a rare pathology
Clinical picture :
Headache without signs of meningeal irritation
Convulsions
Focal neurological deficit (paralysis, loss of
sensation, visual field defects)
11.
Subdural abscess
Investigations :
CTscan, MRI
Treatment:
Drainage (neurosurgeons)
Systemic antibiotics
Mastoidectomy
dura is thickened but not pushed inside
•
Collection of pus
•
Treat by drainage (with neurosurgeon)
•
12.
Meningitis
Definition :
Inflammation ofmeninges (pia & arachinoid).
Pathology:
Occurs during acute exacerbation of chronic
unsafe middle ear infection.
Commonly seen in children
•
But can happen with
•
acute too
Meningitis
Diagnosis :
y Lumbarpuncture is diagnostic.
Treatment:
Treatment of the complication itself and control
of ear infection:
Specific an ibio ics.
An ip re ics and s ppor i e meas res
Mas oidec om o con rol he ear infec ion.
15.
Venous SinusThrombosis
Definition :
yThrombophlebitis of the venous sinus.
Etiology:
y It usually develops secondary to direct extension.
As it is close to mastoid bone, direct extension
Venous SinusThrombosis
Clinical picture:
Headache,vomiting, and papilledema(increase
intracranial pressure ).
Signs of blood invasion:
(spiking) fe er i h rigors and chills .
persis en fe er (sep icemia).
Positive Greissinger’s sign which is edema
and tenderness over the area of the mastoid
emissaryVein. Superficial pain that goes through the skull, so any Palpation
causes pain.
18.
Venous SinusThrombosis
Diagnosis
y CTscan with contrast.
y MRI, MRA, MRV
y Angiography, venography.
y Blood cultures is positive during the febrile
phase.
19.
Venous SinusThrombosis
Treatment :
Medical:
Anibio ics and s ppor i e rea men .
An icoag lan s.
Surgical:
Mas oidec om i h e pos re of he affec ed
sinus and the intra-sinus abscess is drained.
If mastoid is involved
20.
Brain Abscess
Definition :
yLocalized suppuration in the brain substance.
y It is most lethal complication of suppurative otitis
media.
Incidence:
y 50% is Otogenic brain abscess.
Brain abscess is generally rare but most of
them are caused by ear pathology
Brain Abscess
Treatment :
Medical:
Ss emic an ibio ics.
Meas re o decrease in racranial press re.
Surgical:
Ne ros rgical drainage of he abscess .
mas oidec om opera ion af er s bsidence of he
acute stage.
Lumbar puncture & drainage
Labyrinthine fistula
Definition :
ycommunication between middle and inner ear
Atiology :
y It is caused by erosion of boney labyrinth due
cholesteatoma.
27.
Labyrinthine fistula
Clinical picture:
y Hearing loss.
y Attack of vertigo mostly during straining ,sneezing
and lifting heavy object.
y Positive fistula test.Putting pressure in EAC the
patient will develop vertigo
28.
Labyrinthine fistula
Diagnosis:
y Highindex of suspicion
y longstanding disease
y fistula test
y Ct scan of temporal bone
Treatment :
Mastoidectomy.
0
coronal section
•
Advanced not our level
•
29.
Facial nerve paralysis
yCongenital or acquired dehiscence of nerve canal.
y It is possibly a result of the inflammatory response
within the fallopian canal to the acute or chronic
otitis media.
y Tympanic segment is the most commom site to be
involved. What are the segment of facial nerve?
Labyrinthine
•
tympanic
•
Mastoidal
•
30.
Facial nerve paralysis
Diagnosis:
y Clinically
y May occur in acute or chronic ottis media.
y CT scan.
UMNL & LMNL
To differentiate look at the
forehead, if it is involved then
it is a LMNL but in UMNL the
forehead is spared.
31.
Facial nerve paralysis
Treatment:
y Acute otitis media and acute mastoiditis :
(cortical mastoidectomy +ventilation tube).
y chronic otitis media with cholestetoma:
(mastoidecomy ± facial nerve decompresion )
Do it immediately to relieve the pressure +
give IV Abx and cortisol = fixed within a week
If you don’t do it immediately he might have
permanent damage
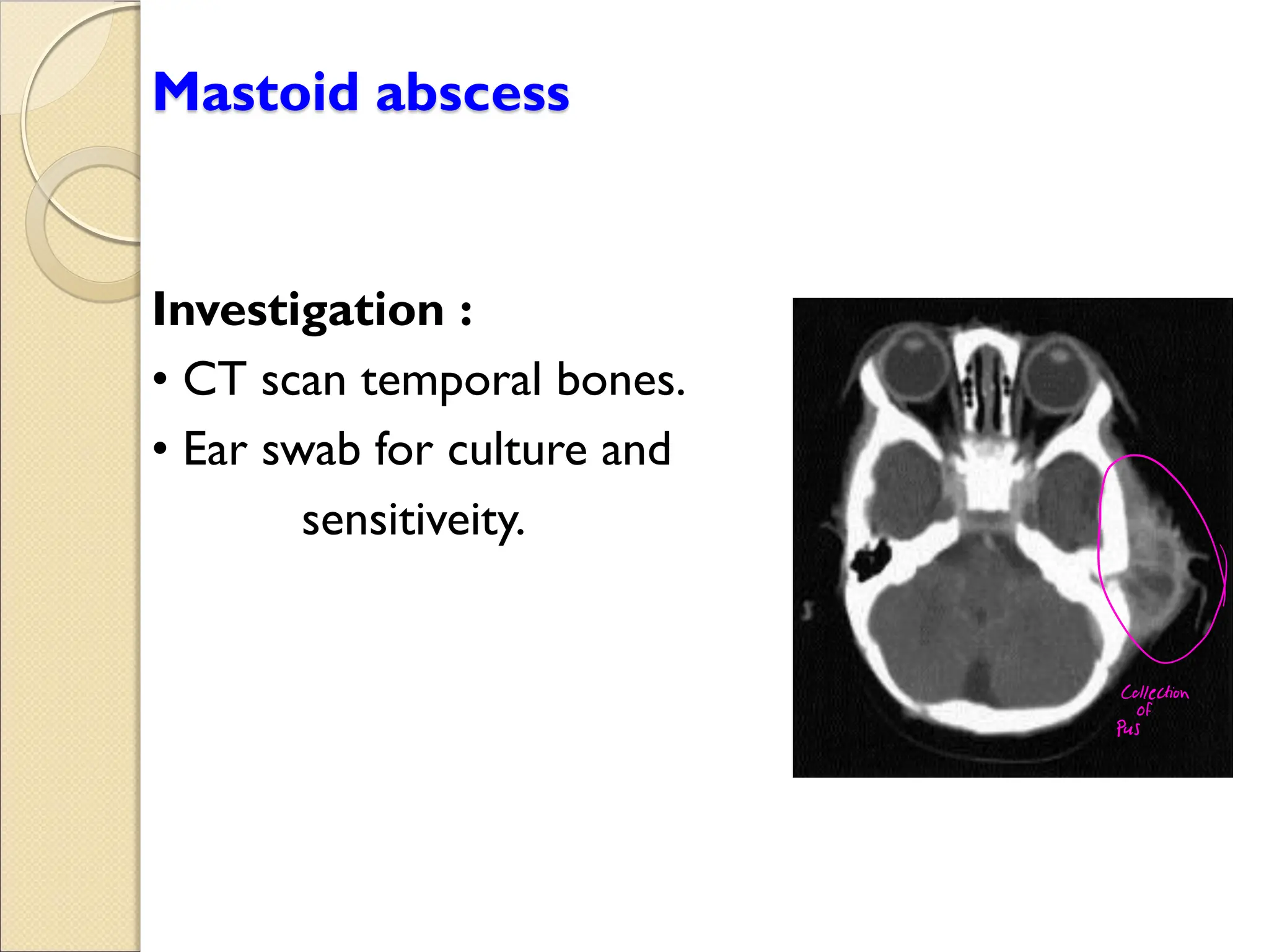
Extracranial complications
y Extensionof infection to the neck.
y Bezold abscess ( extension of infection
from mastoid to SCM).
Sternocleidomastoid muscle

































![EXTRACRANIAL COMPLICATIONS OF OTITIS MEDIA [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/extracranialcomplicationsofotitismediaautosaved-250922194437-495a40c8-thumbnail.jpg?width=640&height=640&fit=bounds)




































