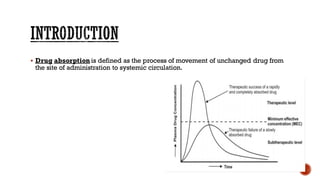
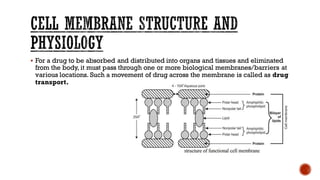
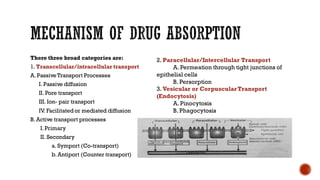
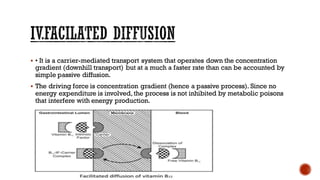
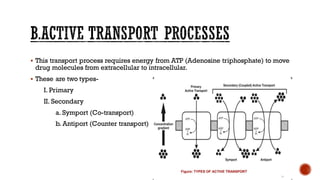
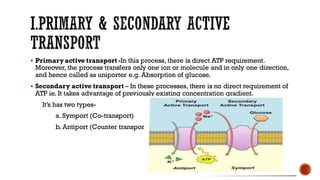
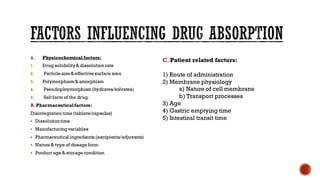
This document discusses drug absorption through the gastrointestinal tract. It begins with an introduction and overview of the major routes of drug administration. It then describes the structure of cell membranes and the various mechanisms of drug transport across membranes, including both passive and active processes. Specific mechanisms discussed include diffusion, pore transport, ion-pair transport, and facilitated transport. The document focuses on drug absorption through the GI tract, outlining the three steps of transcellular transport and describing various passive transport processes. Finally, it discusses factors that can influence drug absorption through the GI, including physicochemical properties of the drug and various patient-related factors.




























![Medication Absorption Breakthrough by Slidesgo [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/medicationabsorptionbreakthroughbyslidesgoautosaved-240123180914-80ac1152-thumbnail.jpg?width=640&height=640&fit=bounds)














![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




