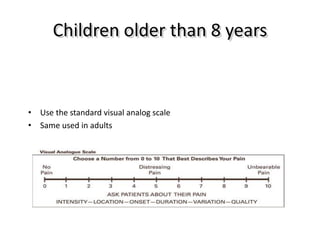
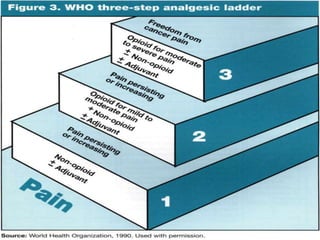
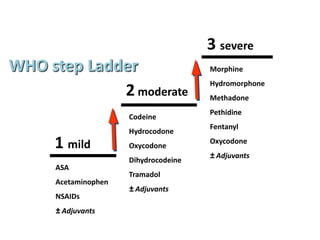
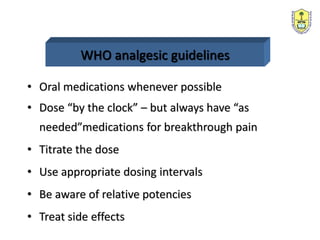
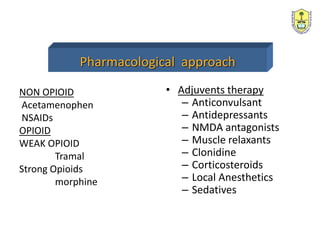
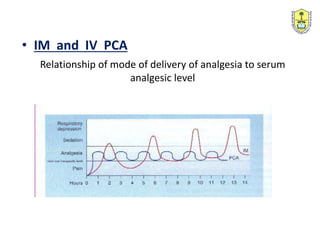
Dr. Fatma Al-Dammas is an anesthesiology professor and director of the anesthesia and acute/chronic pain management programs. She specializes in managing pain, which requires a multidisciplinary team approach. The goals of pain treatment are to improve quality of life, facilitate recovery, reduce morbidity, and allow for early hospital discharge. Pain management involves both pharmacological and non-pharmacological approaches, including the WHO pain ladder and various methods of drug delivery like epidural analgesia. Epidural analgesia provides effective post-operative pain relief, improves pulmonary function, and enables earlier ambulation.






















































![TB.PPT[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/tb-230315182737-c11eabf5-thumbnail.jpg?width=640&height=640&fit=bounds)



















