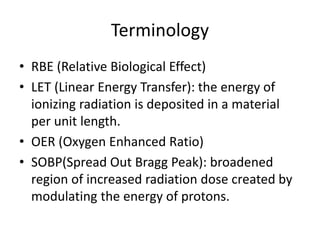
Terminology
• RBE (RelativeBiological Effect)
• LET (Linear Energy Transfer): the energy of
ionizing radiation is deposited in a material
per unit length.
• OER (Oxygen Enhanced Ratio)
• SOBP(Spread Out Bragg Peak): broadened
region of increased radiation dose created by
modulating the energy of protons.
Gunma_1
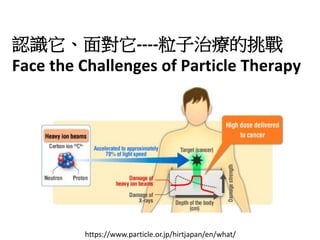
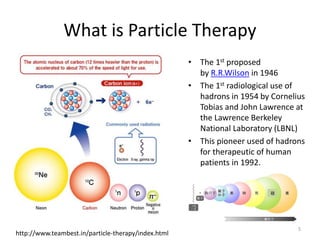
What is ParticleTherapy
• The 1st proposed
by R.R.Wilson in 1946
• The 1st radiological use of
hadrons in 1954 by Cornelius
Tobias and John Lawrence at
the Lawrence Berkeley
National Laboratory (LBNL)
• This pioneer used of hadrons
for therapeutic of human
patients in 1992.
5
http://www.teambest.in/particle-therapy/index.html
硅
6.
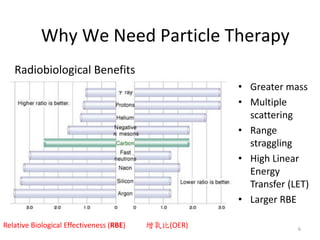
Radiobiological Benefits
• Greatermass
• Multiple
scattering
• Range
straggling
• High Linear
Energy
Transfer (LET)
• Larger RBE
6
Relative Biological Effectiveness (RBE) 增氧比(OER)
Why We Need Particle Therapy
8.
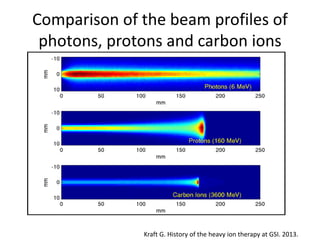
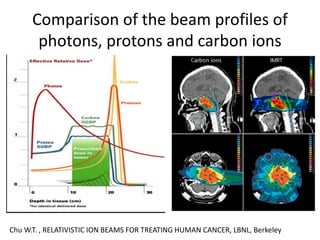
Comparison of thebeam profiles of
photons, protons and carbon ions
Kraft G. History of the heavy ion therapy at GSI. 2013.
9.
Comparison of thebeam profiles of
photons, protons and carbon ions
Chu W.T. , RELATIVISTIC ION BEAMS FOR TREATING HUMAN CANCER, LBNL, Berkeley
10.
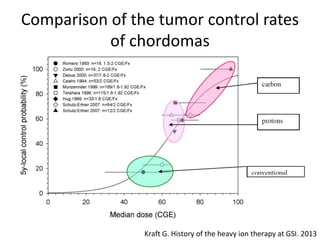
Comparison of thetumor control rates
of chordomas
Kraft G. History of the heavy ion therapy at GSI. 2013
Hirohiko Tsujii: Overviewof Particle Therapy- Past, Present and Future, Hualien Tzu-Chi General Hospital
53
54.
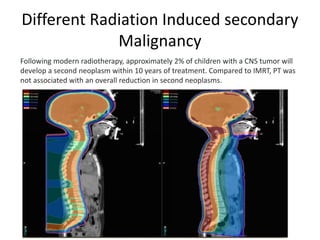
Different Radiation Inducedsecondary
Malignancy
Secondary Malignancy Risk Following Proton Radiation Therapy
Bree R Eaton 1,†,*, Shannon M MacDonald 1, Torunn I Yock 1, Nancy J Tarbell 1
•PMCID: PMC4659915 PMID: 26636040
Radiation induced secondary malignancies: a review article"
https://www.e-roj.org/journal/view.php?doi=10.3857/roj.2018.00290
Second cancer risk after primary cancer treatment with three-dimensional conformal,
intensity-modulated, or proton beam radiation therapy
Michael Xiang MD, PhD, Daniel T. Chang MD, Erqi L. Pollom MD, MS
First published: 19 May 2020 https://doi.org/10.1002/cncr.32938Citations: 145
Secondary Neoplasms in Children with Central Nervous System (CNS) Tumors Following
Radiotherapy in the Modern Era
Daniel Indelicato1, Kathryn Tringale2, Julie Bradley1, Raymond Mailhot Vega1, Christopher Morris1, Dana Casey3, Suzanne
Wolden2
1 University of Florida, Jacksonville, FL, USA. 2 Memorial Sloan-Kettering Cancer Center, New York, NY, USA. 3 University
of North Carolina, Chapel Hill, NC, USA
55.
Different Radiation Inducedsecondary
Malignancy
Following modern radiotherapy, approximately 2% of children with a CNS tumor will
develop a second neoplasm within 10 years of treatment. Compared to IMRT, PT was
not associated with an overall reduction in second neoplasms.
56.
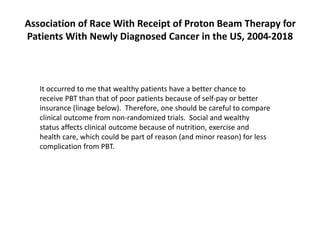
It occurred tome that wealthy patients have a better chance to
receive PBT than that of poor patients because of self-pay or better
insurance (linage below). Therefore, one should be careful to compare
clinical outcome from non-randomized trials. Social and wealthy
status affects clinical outcome because of nutrition, exercise and
health care, which could be part of reason (and minor reason) for less
complication from PBT.
Association of Race With Receipt of Proton Beam Therapy for
Patients With Newly Diagnosed Cancer in the US, 2004-2018
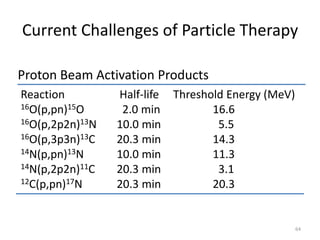
Proton Beam ActivationProducts
64
Reaction Half-life Threshold Energy (MeV)
16O(p,pn)15O 2.0 min 16.6
16O(p,2p2n)13N 10.0 min 5.5
16O(p,3p3n)13C 20.3 min 14.3
14N(p,pn)13N 10.0 min 11.3
14N(p,2p2n)11C 20.3 min 3.1
12C(p,pn)17N 20.3 min 20.3
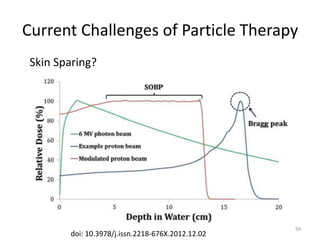
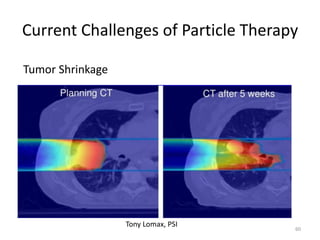
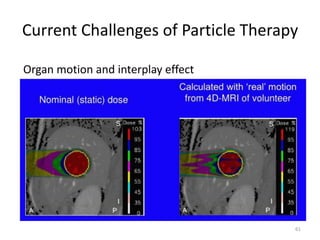
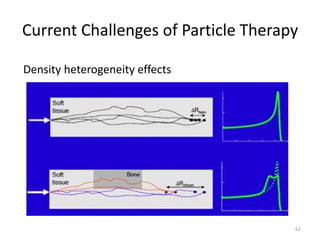
Current Challenges of Particle Therapy
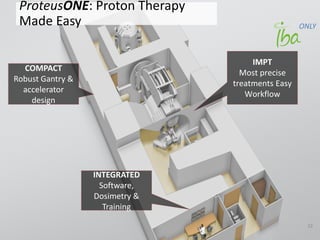
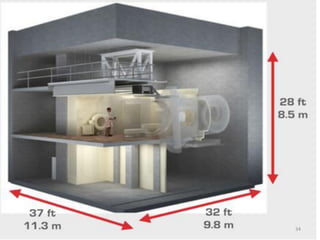
PROTON BEAM THERAPY(PBT)
This Model Policy* addresses coverage for Proton Beam Therapy.
DESCRIPTION
Proton Beam Therapy (PBT) is a technology for delivering conformal external beam radiation with positively
charged subatomic particles to a well-defined treatment volume. PBT is approved by the U.S. Food and Drug
Administration.
PBT has unique dose deposition characteristics and can deliver radiation to specified anatomic targets while giving
less collateral dose to surrounding normal tissues in comparison to photon/X-ray-based forms of external beam
radiotherapy.
Photon/X-ray beams deliver most of their energy in tissues just beneath the patient’s surface, with the remainder
deposited along the beams’ path as photons/X-ray pass through the target and exit the body. In contrast, the
physical profile of proton beams allows delivery of dose over a narrow range of depth in the body with no exit dose.
Compared to photon beams, proton beams deposit less dose upon entering the body, with subsequent dose
deposition then rapidly increasing over a narrow range of tissue at a desired depth to produce an intense dose
distribution pattern called the Bragg peak. Beyond the Bragg peak, energy and dose deposition rapidly decrease,
resulting in small, insignificant amounts of dose to normal tissues that lay beyond the target. A single proton beam
can offer uniform dose to target volume. Multiple beams can be combined and optimized to achieve
highly conformal dose distributions.
TREATMENT
PBT Treatment Planning
PBT can allow for radiation treatment plans that are highly conformal to anatomic targets and minimize dose to
normal tissues. Specifics of PBT planning include appropriate determination of device configuration (e.g.,
necessary field sizes, number of beams, gantry angles, beam energy selection, robust optimization) needed to
achieve the desired radiation dose distribution.
An assessment of patient suitability for PBT is an important step in the process of care. Anatomical changes,
such as patient weight, or alterations in the density and composition of tissues in the path of the beam can have
a much greater impact on the delivered dose and plan integrity for protons than photons/X-ray.
Harvard Publishes RelatedResearch
• At the International Conference on Radiation
Therapy (Sept 30, last year), Dr. Jason Efstathiou
from Massachusetts General Hospital (Harvard
Medical School) presented results of a controlled
clinical trial comparing photon and proton
therapy for localized prostate cancer.
• The study found that both treatments were
**equally effective**.
77.
Key Findings ofthe Study
• Controlled clinical trial on localized prostate
cancer patients.
• Comparison between **Photon Therapy**
and **Proton Therapy**.
• **Outcome:** No significant difference in
effectiveness between the two.
• Implication: Advanced technology (proton
therapy) may not always offer better results.
78.
Clinical Implications forPatients
Dr. Efstathiou highlighted that:
• About **70% of prostate cancer** cases in the U.S. are
localized.
• With appropriate treatment, **long-term survival** is
expected.
• Priority should be on minimizing long-term side effects:
- Bowel dysfunction
- Urinary incontinence
- Sexual dysfunction
Focus of therapy should be on quality of life, not technology
prestige.