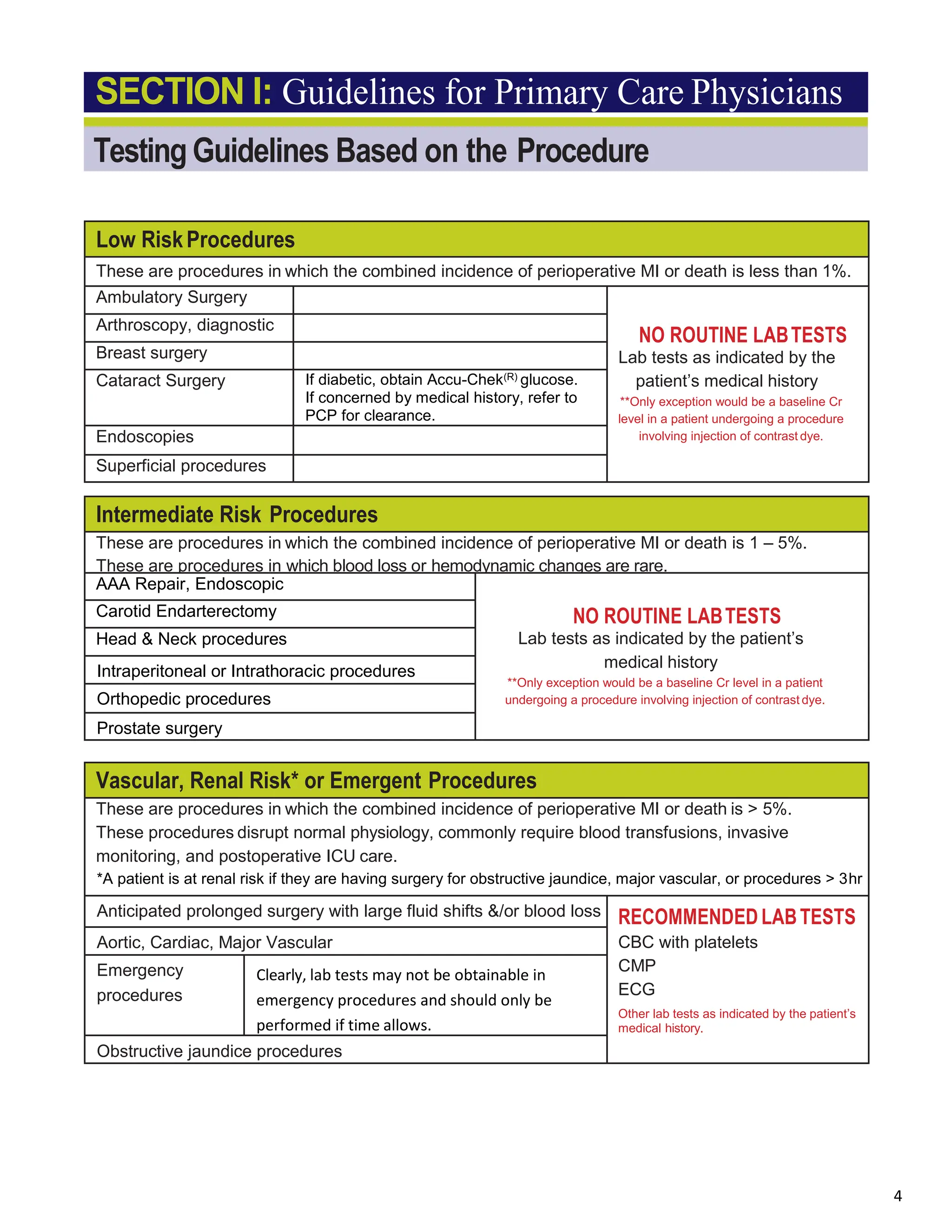
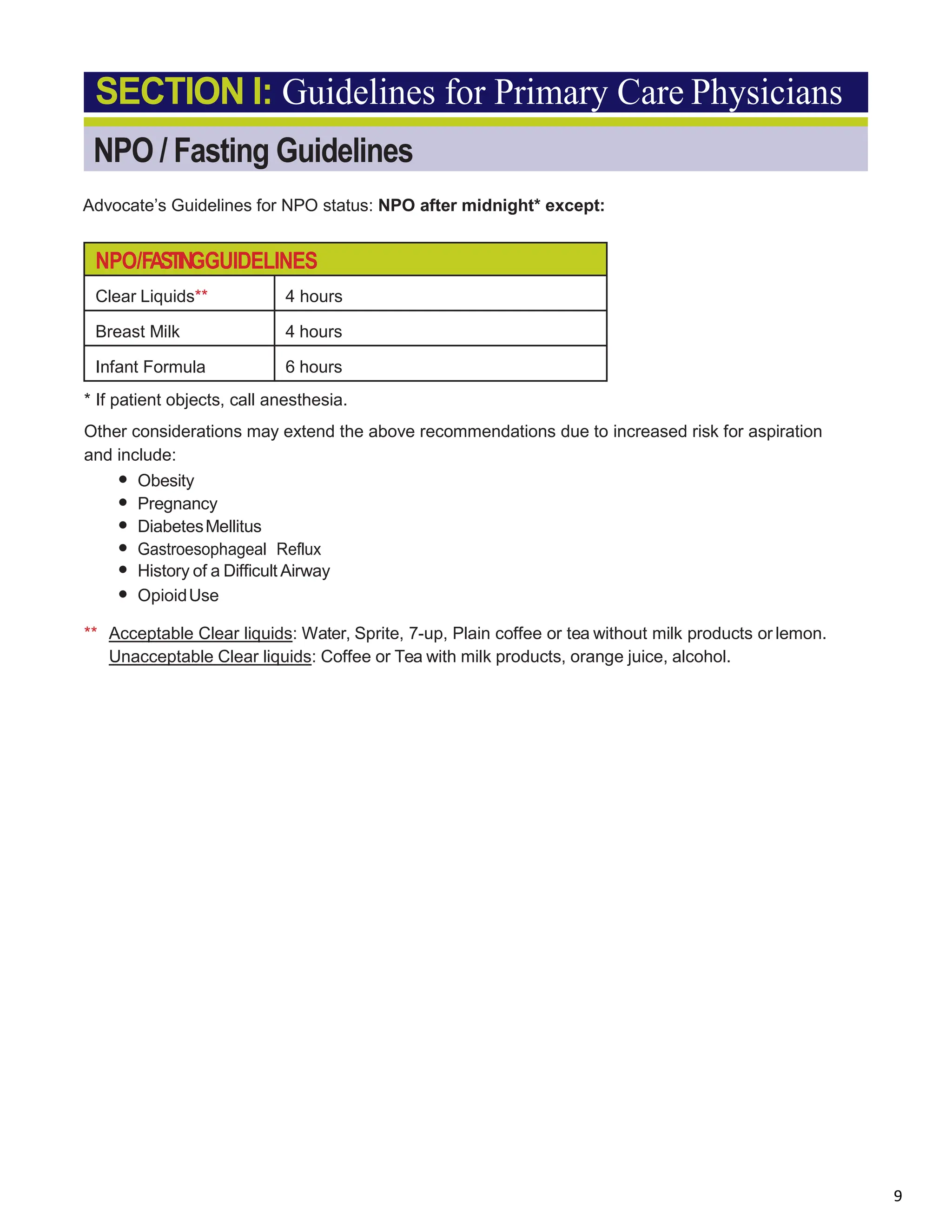
This document provides guidelines for pre-anesthesia evaluation created by Advocate Safer Surgery Council. It was last revised in March 2016 and is intended as a tool for the preoperative evaluation of surgical patients based on best evidence. The guidelines are not intended to supersede the judgment of individual physicians. It provides information on testing recommendations based on procedure risk, medical history, medications, and other factors. It also provides guidelines on preoperative fasting, smoking cessation, and cardiac evaluation.