Downloaded 504 times
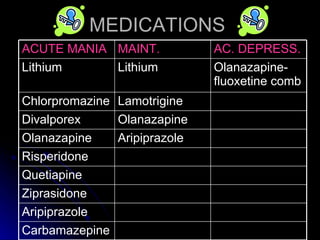
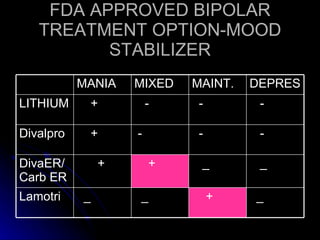
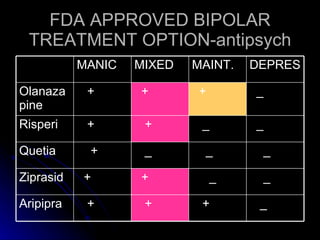
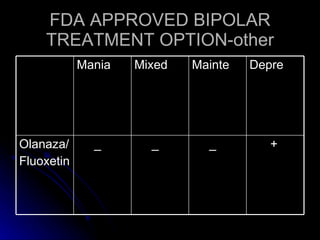
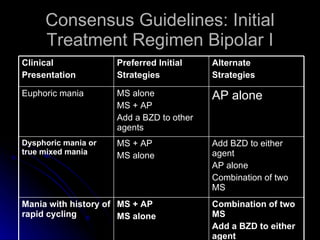
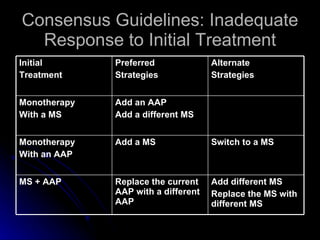
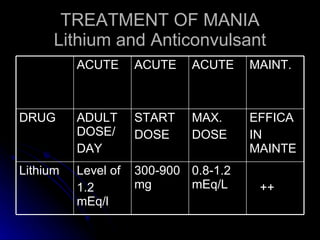
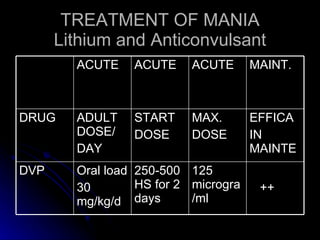
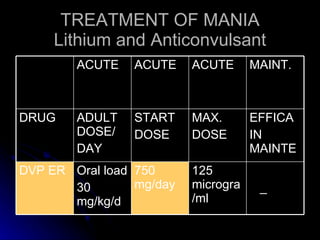
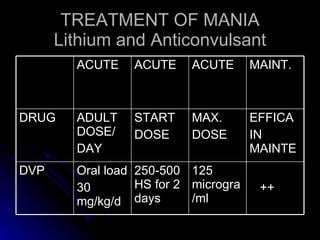
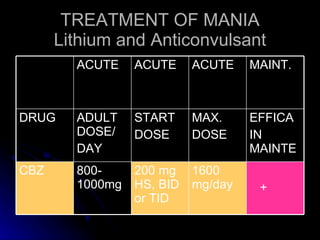
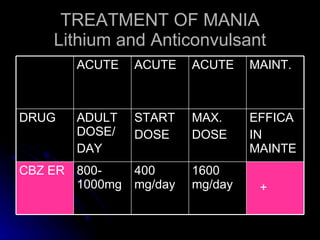
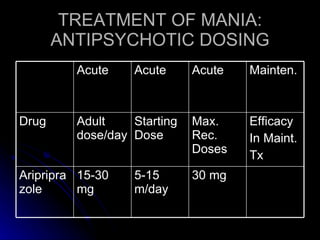
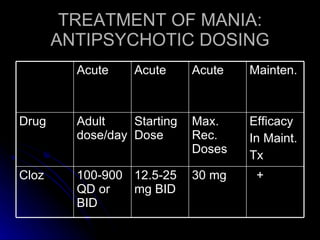
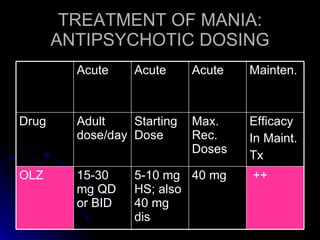
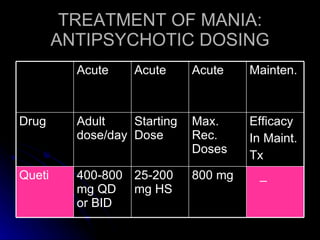
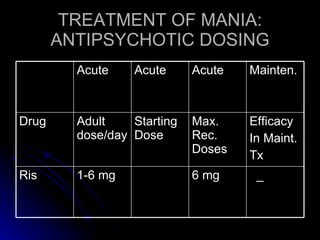
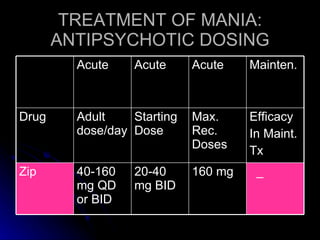
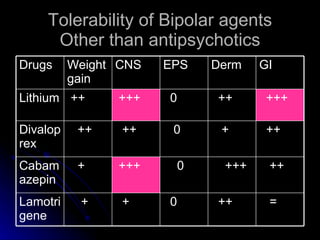



The document discusses the diagnosis and treatment of bipolar disorder, with a focus on mixed episodes. It provides information on the epidemiology, symptoms, course, and management strategies for mixed episodes. Regarding treatment, it outlines FDA-approved medication options and dosing guidelines for mood stabilizers, antipsychotics, and other agents. It also reviews consensus guidelines for initial treatment regimens and strategies for inadequate response. Combination therapies are discussed as an effective approach, especially for more severe cases.











































































