Fall in geriatrics
•
3 likes•239 views

causes of fall in geriatric along with physiotherapy prevention and management

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Fall in geriatrics
Similar to Fall in geriatrics (20)
More from Radhika Chintamani
More from Radhika Chintamani (20)
Recently uploaded
Recently uploaded (20)
Fall in geriatrics
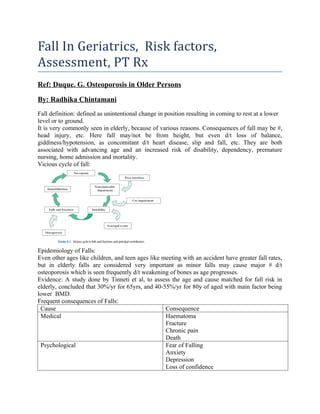
- 1. Fall In Geriatrics, Risk factors, Assessment, PT Rx Ref: Duque. G. Osteoporosis in Older Persons By: Radhika Chintamani Fall definition: defined as unintentional change in position resulting in coming to rest at a lower level or to ground. It is very commonly seen in elderly, because of various reasons. Consequences of fall may be #, head injury, etc. Here fall may/not be from height, but even d/t loss of balance, giddiness/hypotension, as concomitant d/t heart disease, slip and fall, etc. They are both associated with advancing age and an increased risk of disability, dependency, premature nursing, home admission and mortality. Vicious cycle of fall: Epidemiology of Falls: Even other ages like children, and teen ages like meeting with an accident have greater fall rates, but in elderly falls are considered very important as minor falls may cause major # d/t osteoporosis which is seen frequently d/t weakening of bones as age progresses. Evidence: A study done by Tinneti et al, to assess the age and cause matched for fall risk in elderly, concluded that 30%/yr for 65yrs, and 40-55%/yr for 80y of aged with main factor being lower BMD. Frequent consequences of Falls: Cause Consequence Medical Haematoma Fracture Chronic pain Death Psychological Fear of Falling Anxiety Depression Loss of confidence
- 2. Social Dependency Isolation Placement in Long-term Care Functional Immobility Deconditioning Disability and dependence Causes and Risk Factors: Domain Risk factor Assessment tools Neuromuscular Parkinson gait syndrome Balance and Gait problem Lower extremity weakness Gait Velocity Get UP and Go POMA Medical Dizziness or vertigo Visual impairement Peripheral neuropathy Hip problems or deformity Cognitive problems or depression Auditory tests, History and examination Visual acuity test NCV X-rays Depression scales Environmental Environmental fall hazards Assessment of environmental fall hazards Cardiovascular Orthostatic hypotension Post-prandial Hypotension Vaso-vagal syndrome Carotid sinus hypersensitivity Measurement of BP: Morning as soon as he wakes up, bed tilted at 45degs, supine-to-sit, etc. Assessment of JVP. Common causes of falls and abnormal mobility and gait in older adults Symptom Potential Cause Difficulty raising from chair Weakness Osteoarthritis Instability on first standing Hypotension Weakness Instability with eyes closed Problems related to proprioception Decreased step height and length Parkinsonism Frontal Lobe disease Fear of Falling According to Hierarchy Sensorimotor Level, Level of gait seen in elderly: Level Deficit/ Condition Gait Characteristics Low Peripheral sensory ataxia, vestibular and visual ataxia. Peripheral motor-deficits owing to hip problems Arthritis (antalgic gait, joint deformity) Peripheral motor deficits (owing to myopathic and neuropathic Unsteady and uncoordinated gait (esp without visual input) Avoids WB on affected side Painful knee flexed Painful spine produces=short, slow steps. Decreased lumbar lordosis, and increased thoracic kyphosis produces=stooped posture. Proximal motor neuropathy produces= waddling gait and foot slap.
- 3. conditions) Distal produces= distal weakness Middle Spasticty from hemiplegia, or hemiparesis Parkinsonism Cerebellar ataxia Circumductory gait. Shuffling gait/festinating gait Drunked gait High Cautious gait Ignition failure Fear of falling with appropriate postural response, normal to widened gait base, shortened stride, Slower turning, and performance improve with assistance. Frontal Gait disorders, difficulty initiating gait, short shuffling steps, but normal wide base, upright posture and with arm swing. -Nutt et al Approaches for assessing falls: The first approach should include taking a history of previous falls, because this is the most important predictor for future falls. A complete fall evaluation should include an assessment of balance and gait, vision acuity, and documentation of the individual’s medication history. This triad is considered to have a high predictive value for detecting older adults at higher risk for falls in the community. A hemodynamic episode such as postural hypotension and vasovagal symptoms, these entities should also be considered. Falls after taking certain medications identification of drugs associated to falls (e.g., diuretics, vasodilators, and benzodiazepines). Environmental factors that may have contributed to the fall (e.g., a loose carpet, poor lighting, or a displaced piece of furniture). Gait can be assessed from either a quantitative or qualitative perspective. the Get Up and Go consists of rising from a chair, walking 3 m, turning around, walking back to the start point, and sitting down again. A later modification by Podsialo and Richardson incorporated a timed component to the performance measure of the test, thus providing extra information for analysis and clinical interpretation. Because this test was initially created to evaluate frail elderly with disability, a problem faced when evaluating older persons in the community is a ceiling effect, because high-functioning older adults generally perform well on the task. Therefore, for these individuals a cut-off time of 12 seconds has been proposed in order to detect those vulnerable to suffer future falls. More complex tests such as the Performed Oriented Mobility Assessment (POMA) test and the Berg Balance Scale has been described and validated for assessing risk of falling in different scenarios. Powerful test that can be used in different settings is the gait velocity test. It has been demonstrated to be very sensitive test for detecting mobility problems and to predict falls, even in high-functioning older people. Gait velocity is measured as the time taken to walk a known and predetermined distance (e.g., the middle 8 m of 10 m) and it is usually timed by a chronometer (38), with the participants being instructed to “walk at a comfortable and secure pace.” The only limitation of the gait velocity test appears when it is used in people using assistive devices. In this situation, changes in the functionality may show less effect on gait velocity. It has been suggested to use a gait velocity cut off of 1 m/second in community elderly
- 4. without disability, 0.8 m/second in older persons with disabilities, and 0.6 m/second in older persons living in nursing homes. Berg Balance test: To assess for the balance of an individual. Has 8 components, or activities to be performed. The more important factors for fracture risk are the history of previous osteoporosis fracture, the use of psychotropic medication, and the presence of sarcopenia and impaired mobility. Recent Advances: PT Rx: 1. The Otago Exercise Programme is a regimen of home exercises using a combination of strength and balance exercises supplemented with a walking program. It is designed to be individually prescribed by a trained professional, undertaken 2–3 times per week, and progressed over time. Evidence: In the original study, among women aged over 80 years (1), there was a significant reduction in falls over a 12-month period (between group difference = 0.47, 95% confidence interval [CI] 0.04–0.90). At the end of a second year (with 69% of intervention and 74% of control group continuing from the original study), the reduction in falls rates remained significant (relative risk [RR] 0.69, 95% CI 0.49–0.97 2. Group exercise: This is an important concept, as many older people enjoy the socialization and opportunity to leave the home that a group exercise program offers. Group exercises may be individualized and tailored to the needs of the older person or involve all participants undertaking the same exercises and at the same intensity. Evidence: Barnett et al. found that group-based balance and strength exercises signifi cantly reduced falls in community-dwelling people (IRR 0.60, 95% CI 0.36–0.99). 3. Reducing Hazards in Home: cient to cause falls. The interaction between an older person’s physical abilities and their exposure to environmental stressors appears to be more important. Evidence: Cumming et al. (37) conducted a study among 530 community-dwellers, most of whom had been recently hospitalized. The intervention group received a home visit by an occupational therapist who assessed the home for environmental hazards and facilitated any necessary home modifi cations. There was no signifi cant reduction in falls in the intervention group as a whole. There was however a signifi cant reduction in the rate of falls among those who had fallen in the year prior to the study (RR 0.64, 95% CI 0.50–0.83). Falls in this group were signifi cantly reduced both inside and outside of the home, suggesting that the home modifi cations alone may not have been the major factor in the reduction in falls rates. 4. Preventing Hip Fractures With Hip Protectors: Hip protectors are designed to absorb energy and to transfer load from the bone to the surrounding soft tissues (55). The original hip protectors (56) incorporated a fi rm outer shell and an inner foam section. Other versions are made of dense plastic without an outer shell (57). Hip protectors either fi t into pockets of underwear or are built into underwear.
- 5. Evidence: A further study in Sweden (58) tested a different model of hip protector and also found a decreased fracture rate among residents of a randomly selected nursing home that was offered hip protectors compared with a control nursing home (RR 0.33).