Call Girl Surat Madhuri 7001305949 Independent Escort Service Surat
Patient Care Seminar - Case Report
1. www.postersession.com
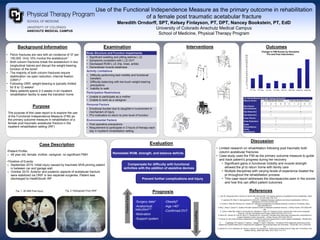
Use of the Functional Independence Measure as the primary outcome in rehabilitation
of a female post traumatic acetabular fracture
Meredith Orndorff, SPT, Kelsey Finlayson, PT, DPT, Nancey Bookstein, PT, EdD
University of Colorado Anschutz Medical Campus
School of Medicine, Physical Therapy Program
Background Information
Purpose
The purpose of this case report is to explore the use
of the Functional Independence Measure (FIM) as
the primary outcome measure in rehabilitation of a
female post traumatic acetabular fracture in the
inpatient rehabilitation setting (IRF)
Case Description
•Patient Profile:
o 49 year old, female, mother, caregiver, no significant PMH
•Timeline of Events:
o September 2015: Initial injury caused by traumatic MVA pinning patient
in between car and garage wall
o October 2015: Anterior and posterior aspects of acetabular fracture
were stabilized via ORIF in two separate surgeries. Patient was
discharged to HealthSouth IRF
Interventions Outcomes
Discussion
References
• Pelvic fractures are rare with an incidence of 37 per
100,000. Only 10% involve the acetabulum1
• Both column fractures break the acetabulum in two
longitudinal halves and disrupt the weight-bearing
function of the bone2
• The majority of both column fractures require
stabilization via open reduction, internal fixation
(ORIF) 2
• Following ORIF, weight-bearing is typically limited
for 8 to 12 weeks2
• Many patients spend 2-3 weeks in an inpatient
rehabilitation facility to ease the transition home
Examination
Evaluation
Fig. 1: 3D MRI Post injury Fig. 2: Radiograph Post ORIF
Body Structure and Function Impairments
• Significant swelling and pitting edema L LE
• Symptoms consistent with L LE DVT
• Decreased ROM L LE (hip, knee, ankle)
• Generalized muscle weakness
Activity Limitations
• Difficulty performing bed mobility and functional
transfers
• Difficulty balancing with toe touch weight-bearing
precautions
• Inability to walk
Participation Restrictions
• Unable to participate as a mother
• Unable to work as a caregiver
Personal Factors
• Emotional burden due to daughter’s involvement in
mechanism of injury
• Pt’s motivation to return to prior level of function
Environmental Factors
• Post operative precautions
• Requirement to participate in 3 hours of therapy each
day in inpatient rehabilitation setting
-Surgery date3
-Anatomical
reduction4,5
-Motivation
-Support system
-Obesity6
-Age >403
-Confirmed DVT
PositiveFactors
NegativeFactors
Remediate ROM, strength, and balance deficits
Compensate for difficulty with functional
activities with the addition of assistive devices
Prevent further complications and injury
Prognosis
0
7
14
21
28
35
42
49
56
63
70
77
84
91
98
105
112
119
126
PT Pre PT Post OT Pre OT Post RN Pre RN Post Total Pre Total Post
Change in FIM Scores by Discipline
Pre and Post Intervention
(L) Group Muscle Strength Testing Outcomes
Muscle Action Pre Intervention Score Post Intervention Score
0 1 2 3 4 5 0 1 2 3 4 5
Hip Flexion - +
Hip Extension + /
Hip Abduction + +
Hip Adduction + /
Knee Flexion + /
Knee Extension + /
Ankle
Plantarflexion
+ /
Ankle
Dorsiflexion
+ /
• Limited research on rehabilitation following post traumatic both
column acetabular fractures
• Case study used the FIM as the primary outcome measure to guide
and track patient’s progress during her recovery
• Significant gains in functional mobility and muscle strength
allowed the pt to return home with family care
• Multiple disciplines with varying levels of experience treated the
pt throughout the rehabilitation process
• This case report addresses the discrepancies seen in the scores
and how this can affect patient outcomes
1. Hutt JR, Ortega-Briones A, Daurka JS, Bircher MD, Rickman MS. The ongoing relevance of acetabular fracture classification. Bone
Joint J. 2015;97-B(8):1139-1143.
2. Lawrence DA, Menn K, Baumgaertner M, Haims AH. Acetabular fractures: anatomic and clinical considerations. AJR Am J
Roentgenol. 2013;201(3):W425-436.
3. Kumar A, Shah NA, Kershaw SA, Clayson AD. Operative management of acetabular fractures. A review of 73 fractures. Injury.
2005;36(5):605-612.
4. Borg T, Berg P, Larsson S. Quality of life after operative fixation of displaced acetabular fractures. J Orthop Trauma. 2012;26(8):445-
450.
5. Lichte P, Sellei RM, Kobbe P, Dombroski DG, Gänsslen A, Pape HC. Predictors of poor outcome after both column acetabular
fractures: a 30-year retrospective cohort study. Patient Saf Surg. 2013;7(1):9.
6. Sems SA, Johnson M, Cole PA, Byrd CT, Templeman DC, Group MOT. Elevated body mass index increases early complications of
surgical treatment of pelvic ring injuries. J Orthop Trauma. 2010;24(5):309-314.
7. Cournan M. Use of the functional independence measure for outcomes measurement in acute inpatient rehabilitation. Rehabil Nurs.
2011;36(3):111-117.
8. Engelberger RP, Aujesky D, Calanca L, Staeger P, Hugli O, Mazzolai L. Comparison of the diagnostic performance of the
original and modified Wells score in inpatients and outpatients with suspected deep vein thrombosis. Thromb Res. 2011;127(6):535-
539.
9. Silveira PC, Ip IK, Goldhaber SZ, Piazza G, Benson CB, Khorasani R. Performance of Wells Score for Deep Vein Thrombosis in the
Inpatient Setting. JAMA Intern Med. 2015;175(7):1112-1117