
Recommended
More Related Content
What's hot
What's hot (20)
Similar to PERICARDITIS: CAUSES, SYMPTOMS AND DIAGNOSIS
Similar to PERICARDITIS: CAUSES, SYMPTOMS AND DIAGNOSIS (20)
More from Priya
More from Priya (20)
Recently uploaded
Recently uploaded (20)
PERICARDITIS: CAUSES, SYMPTOMS AND DIAGNOSIS
- 2. INTRODUCTION The incidence of acute pericarditis is approximately 27.7 per 100,000 individuals annually. The recurrence of disease is seen in almost 30% of patients after first episode. The mortality rate of acute pericarditis is approximately 1.1% in developed countries. Patients of all age groups may develop acute pericarditis. Although it commonly affects men in 20 to 50 years of age. Pericarditis in developed countries is most commonly due to malignancy or viral infection. It usually follows respiratory infections, most commonly echovirus or coxsackie virus. In children, it is most commonly caused by adenovirus or coxsackie virus. In developing countries pericarditis is usually secondary to tuberculosis or HIV infection. Tuberculous pericarditis, caused by Mycobacterium tuberculosis, is found in approximately 1% of all autopsied cases of TB and in 1% to 2% of instances of pulmonary TB
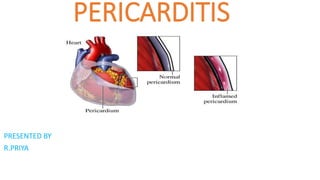
- 3. DEFINITION Pericarditis is an inflammation of the pericardium.The condition usually clears up after 3 months, but sometimes attacks can come and go for years.When you have pericarditis, the membrane around your heart is red and swollen, like the skin around a cut that becomes inflamed. Sometimes there is extra fluid in the space between the pericardial layers, which is called pericardial effusion. Pericarditis can affect anyone, but it is most common in men aged 16 to 65.
- 4. TYPES according to the pattern of symptoms and how long symptoms last. •Acute pericarditis begins suddenly but doesn't last longer than three weeks. Future episodes can occur. It may be difficult to tell the difference between acute pericarditis and pain due to a heart attack. •Recurrent pericarditis occurs about four to six weeks after an episode of acute pericarditis with no symptoms in between. •Incessant pericarditis lasts about four to six weeks but less than three months. The symptoms are continuous. •Chronic constrictive pericarditis usually develops slowly and lasts longer than three months.
- 5. TYPES Pericarditis Based on Causes Constrictive pericarditis When the pericarditis is associated with a thickening or scarring of the pericardial layers, this starts constricting the heart within the thoracic cavity, which in turn limits its effective functioning. This condition is known as constrictive pericarditis. Pericardial effusion In a normal person, the pericardial cavity is filled with about 20–50 ml of fluid. Sometimes, in patients with specific medical conditions (for example, severe hypothyroidism or kidney failure), or in those who have undergone invasive cardiac procedures, there may be a gradual accumulation of fluid within the pericardial cavity. Such gradual fluid accumulation may often be asymptomatic until the surrounding structures (lung, stomach, phrenic nerve) start getting compressed, in which case symptoms related to such compressions (for example, dyspnea, nausea, fullness of the abdomen) may manifest.
- 6. TYPES Cardiac tamponade Steady pericardial effusion can cause the pericardial fluid volume to increase up to 80 ml, or even 200 ml. Such high rises in the pericardial fluid volume can lead to malfunction of the pericardium; therefore, this condition has to be treated as an emergency. Viral pericarditis Viruses that may cause viral pericarditis include coxsackieviruses, influenza virus, agents of viral enteritis, human immunodeficiency virus (HIV), and echovirus. Infection in the upper airways is the early symptom upon the onset of this ailment. This kind of pericarditis is simple and can be handled as an outpatient procedure. Purulent pericarditis This is a rare disease caused by aerobic and anaerobic bacteria. Before the discovery of antibiotics, pneumonia was believed to be the main cause of this infection. Recent studies show that procedures such as surgery in the chest region, hemodialysis, immunosuppression, and chemotherapy are dominant causes that lead to this type of pericarditis.
- 7. TYPES Tuberculous pericarditis This condition is also seen in a very minor percentage of patients having pulmonary tuberculosis. Some of the developing countries remain the leading risk groups of tuberculous pericarditis. Another population at risk is HIV-positive patients. There is a gradual progression in symptoms of night sweats, dyspnea, fever, and chill, but any suspected patient needs to be given emergency treatment in the hospital. Radiation Pericarditis This type of pericarditis is caused due to recent mediastinal radiation at any time from weeks to months after the exposure. Traumatic pericarditis Sharp or blunt trauma causes traumatic pericarditis. Invasive cardiac procedures also may give rise to this type of pericarditis, which includes cardiac diagnostic catheterization and electrophysiological ablation procedure. Malignancy Malignancy pericarditis is mainly caused by metastatic (i.e. spread of cells to new areas of the body) disease. It is common in metastasized bronchogenic or breast carcinoma, Hodgkin’s disease and lymphoma, albeit it is rare in primary mesothelioma and angiosarcoma.
- 8. CAUSES The cause of pericarditis is unknown or unproven in many cases. It mostly affects men ages 20 to 50 years. Pericarditis is often the result of an infection such as: •Viral infections that cause a chest cold or pneumonia •Infections with bacteria (less common) •Some fungal infections (rare) The condition may be seen with diseases such as: •Cancer (including leukemia) •Disorders in which the immune system attacks healthy body tissue by mistake •HIV infection and AIDS •Underactive thyroid gland • Rheumatic fever • Tuberculosis infections •Heart surgery •Heart attack
- 9. CAUSES •Tumors •Autoimmune disease(such as rheumatoid arthritis, lupus, or scleroderma ) •For some people, no cause can be found. Other causes include: •Heart attack •Heart surgery or trauma to the chest, esophagus, or heart •Certain medicines, such as procainamide, hydralazine, phenytoin, isoniazid can cyclosporine, hydralazine, warfarin, and heparin, and some drugs used to treat cancer or suppress the immune system •Swelling or inflammation of the heart muscle •Radiation therapy to the chest •. injury to the chest, such as after a car accident (traumatic pericarditis), other health problems such as kidney failure (uremic pericarditis), tumors, genetic diseases such as Familial Mediterranean Fever (FMF), or rarely.
- 10. PATHOPHYSIOLOGY
- 11. SIGNS AND SYMPTOMS Chest pain is almost always present. The pain: •May be felt in the neck, shoulder, back, or abdomen •Often increases with deep breathing and lying flat, and may increase with coughing and swallowing •Can feel sharp and stabbing •Is often relieved by sitting up and leaning or bending forward You may have fever, chills, or sweating if the condition is caused by an infection. Other symptoms may include: Ankle , feet, and leg swelling Anxiety Breathing difficulty when lying down •Dry cough •Fatigue
- 12. DIAGNOSTIC EALUTION History collection Physical examination doctor will listen to your heart. Pericarditis can cause a rubbing or creaking sound, caused by the rubbing of the inflamed lining of the pericardium.This is called the “pericardial rub” and is best heard when you lean forward, hold your breath and breathe out. Depending on how bad the inflammation is, your doctor may also hear crackles in your lungs, which are signs of fluid in the space around the lungs or extra fluid in the pericardium. Laboratory values can show increased urea (BUN), or increased blood creatinine in cases of uremic pericarditis. Generally, however, laboratory values are normal, but if there is a concurrent myocardial infarction (heart attack) or great stress to the heart, laboratory values may show increased cardiac markers like Troponin (I, T), CK- MB, Myoglobin, and LDH1 (lactase dehydrogenase isotype 1),increased WBC,esr increased,CRP Increased ECG, Findings which may demonstrate a 12-lead electrocardiogram with diffuse, nn-specific, concave ("saddle-shaped"), ST-segment elevations in all leads except aVR and V1 and PR-segment depression possible in any lead except aVR; sinus tachycardia, and low-voltage QRS complexes can also be seen if there is subsymptomatic levels of pericardial effusion. The PR depression is often seen early in the process as the thin atria are affected more easily than the ventricles by the inflammatory process of the pericardium.
- 13. DIAGNOSTIC EVALUATION •Chest X-ray to see the size of your heart and any fluid in your lungs. •Electrocardiogram (ECG or EKG) to look for changes in your heart rhythm. In about half of all patients with pericarditis, the heart rhythm goes through a sequence of four distinct patterns. Some patients do not have any changes, and if they do, they may be temporary. •Echocardiogram (echo) to see how well your heart is working and check for fluid or pericardial effusion around the heart. An echo will show the classic signs of constrictive pericarditis, including a stiff or thick pericardium that constricts the heart’s normal movement. •Cardiac MRI to check for extra fluid in the pericardium, pericardial inflammation or thickening, or compression of the heart. A contrast agent called gadolinium is used during this highly specialized test. •CT scan to look for calcium in the pericardium, fluid, inflammation, tumors and disease of the areas around the heart. Iodine dye is used during the test to get more information about the inflammation.This is an important test for patients who may need surgery for constrictive pericarditis. •Cardiac catheterization to get information about the filling pressures in the heart.This is used to confirm a diagnosis of constrictive pericarditis. •Blood tests can be used to make sure you are not having a heart attack, to see how well your heart is working, test the fluid in the pericardium and help find the cause of pericarditis. If you have pericarditis, it is common for your sedimentation rate (ESR)and ultra sensitive C reactive protein levels (markers of inflammation) to be higher than normal.You may need other tests to check for autoimmune diseases like lupus and rheumatoid arthritis.
- 14. MANAGEMENT •Pain relievers. Pericarditis pain can usually be treated with over-the- counter pain relievers, such as aspirin or ibuprofen (Advil, Motrin IB, others). Prescription-strength pain relievers also may be used. •Colchicine (Colcrys, Mitigare). This drug reduces inflammation in the body. It's used to treat acute pericarditis or if your symptoms tend to come back. You should not take this drug if you have liver or kidney disease. Colchicine can also interfere with other drugs. Your doctor will carefully check your health history before prescribing colchicine. •Corticosteroids. Corticosteroids are strong medications that fight inflammation. Your doctor may prescribe a corticosteroid such as prednisone if your symptoms don't get better with other medications, or if symptoms keep returning.
- 15. MANAGEMENT Surgeries or other procedures If pericarditis causes fluid buildup around the heart, you may need drainage or surgery. Treatments include: •Pericardiocentesis. In this procedure, a doctor uses a sterile needle or a small tube (catheter) to remove and drain the excess fluid from the pericardial cavity. You'll receive a numbing medication (local anesthetic) before the procedure. The doctor uses ultrasound and echocardiogram images to guide the needle and tube to the correct location in the body. This drain stays in place for several days while you are in the hospital. •Pericardiectomy. This surgery removes the entire pericardium. It may be done if the sac surrounding your heart has become permanently rigid due to constrictive pericarditis.