
Recommended
Recommended
More Related Content
Similar to J Youth Adolescence (2007) 361048–1057DOI 10.1007s10964-00.docx
Similar to J Youth Adolescence (2007) 361048–1057DOI 10.1007s10964-00.docx (20)
More from priestmanmable
More from priestmanmable (20)
Recently uploaded
Recently uploaded (20)
J Youth Adolescence (2007) 361048–1057DOI 10.1007s10964-00.docx
- 1. J Youth Adolescence (2007) 36:1048–1057 DOI 10.1007/s10964-006-9163-1 O R I G I N A L PA P E R Construct Validity of Adolescent Antisocial Personality Disorder Jeanette Taylor · Irene J. Elkins · Lisa Legrand · Dawn Peuschold · William G. Iacono Received: 4 October 2006 / Accepted: 14 December 2006 / Published online: 17 January 2007 C© Springer Science+Business Media, LLC 2007 Abstract This study examined the construct validity of antisocial personality disorder (ASPD) diagnosed in adoles- Jeanette Taylor is an Assistant Professor at Florida State University. She received her Ph.D. in 1999 from the University of Minnesota. Her research examines biological, cognitive, and environmental influences on personality disorders and substance use disorders. Irene J. Elkins is a Co-investigator at the Minnesota Center for Twin and Family Research. She received her Ph.D. in 1993 from the University of Kansas and is a member of the Society for Research on Psychopathology. Her major research interests include the relationship
- 2. of personality, ADHD, and antisocial behavior to substance abuse, as well as gene-environment interrelationships. Lisa Legrand is a Research Associate with the Minnesota Center for Twin and Family Research at the University of Minnesota. She received her Ph.D. in 2003 from the University of Minnesota. Her major research interests include gene-environment interplay in the development of externalizing psychopathology. Dawn Peuschold is a Senior Clinical Forensic Psychologist at the Hennepin Country District Court and an instructor at the University of Minnesota. She completed a post-doctoral fellowship in forensic psychology at the University of Massachusetts Medical School after receiving her Ph.D. in clinical psychology from the University of Minnesota. She is interested in risk factors for reoffense in juveniles. William G. Iacono is a Distinguished McKnight University Professor at the University of Minnesota, the institution from which he received his Ph.D. in psychology. He conducts longitudinal studies of adolescent twins and adoptees aimed at understanding the development of adult adjustment and mental health. J. Taylor (�) Department of Psychology, Florida State University, Tallahassee, Florida 32306-1270, USA
- 3. e-mail: [email protected] I. J. Elkins · L. Legrand · D. Peuschold · W. G. Iacono Department of Psychology, University of Minnesota – Twin Cities, Minnesota, USA cence. Boys and girls were grouped by history of DSM-III-R conduct disorder (CD) and ASPD: Controls (n = 340) had neither diagnosis; CD Only (n = 77) had CD by age 17 but no ASPD through age 20; Adolescent ASPD (n = 64) had ASPD by age 17. The Adolescent ASPD group was then compared to 20 young adult men who met criteria for ASPD (ASPD group). As expected, the Adolescent ASPD group had significantly more depression and substance use disor- ders, a greater performance >verbal IQ discrepancy, more deviant peers, and poorer academic functioning than the CD Only group and Controls. The Adolescent ASPD and ASPD groups did not differ on most variables. Results support the construct validity of Adolescent ASPD and suggest that such a diagnosis could help identify adolescents at risk for persis- tent antisocial behavior. Keywords Antisocial personality . Adolescent antisocial behavior . Co-morbidity Antisocial behavior is so common among adolescents that some have called it normative (Moffitt, 1993). Non- normative manifestations of antisocial behavior can be iden- tified in children and adolescents by applying diagnostic cri- teria for conduct disorder (CD) as outlined in the Diagnostic and Statistical Manual of Mental Disorders, 4th Ed. (DSM- IV: American Psychiatric Association, 1994). Another DSM diagnosis that describes manifestations of antisocial behavior is antisocial personality disorder (ASPD), which is reserved for adults aged 18 and older because research shows that while most adult antisocial behavior has its roots in child-
- 4. hood, most antisocial children do not grow up to be antisocial adults (Robins, 1966). As such, the age requirement for the ASPD diagnosis helps avoid placing a lasting label on chil- dren who might very well desist in their antisocial behavior. Unfortunately, this age restriction on the application of the Springer J Youth Adolescence (2007) 36:1048–1057 1049 ASPD diagnosis may result in overlooking a clinically im- portant group of antisocial adolescents. Research suggests that earlier onset of CD and other types of conduct problems are associated with a poor prognosis in terms of academic functioning and trajectory of antisocial behavior (e.g., Moffitt & Caspi, 2001). A similar set of poor outcomes might hold for early presentations of ASPD, in which case the identification of those individuals would be useful in order to hasten intervention. Moreover, the type of intervention that is applied with adolescents exhibiting CD only might differ from that applied to those with ASPD in terms of duration needed to see improvement, client moti- vation for treatment, adherence to treatment, and need for treatment of more numerous and/or severe co-morbid disor- ders (e.g., substance dependence). At present there are no studies in the literature that speak directly to the construct validity of an ASPD diagnosis assigned before age 18 (here- after referred to as “Adolescent ASPD”). However, there is some precedent for examining “adult” constructs in child- hood or adolescence. Psychopathy is a manifestation of antisocial behavior comprised of an antisocial lifestyle combined with a cal-
- 5. lous and emotionally detached interpersonal style, and early descriptions of this clinical phenomenon informed the cre- ation of the ASPD diagnosis. However, psychopathy is not a DSM-based diagnosis and has no age restriction for its application, and a large body of research exists on the downward extension of the psychopathy construct to chil- dren. Findings indicate that children with CD who also show callous and unemotional traits have similar charac- teristics of adults with psychopathy in terms of response styles (Barry et al., 2000; O’Brien & Frick, 1996), an- tisocial behavior pattern (Christian et al., 1997; Frick & Ellis, 1999), and processing of emotional stimuli (Blair, 1999; Frick et al., 1999), suggesting that the psychopa- thy construct is likely valid for children. To the extent that psychopathy and ASPD have overlapping features and tap a similar construct (i.e., a persistent antisocial personal- ity/behavioral style), it stands to reason that the ASPD diag- nosis might similarly be valid when applied to adolescents who are not yet 18, but this notion has not yet been tested. Although the bulk of research appears to support the downward extension of psychopathy to children, it is im- portant to note that this extension has occurred with some controversy and debate over the possible dangers of applying such a label to children (Frick, 2002; Lynam, 2002; Seagrave & Grisso, 2002). One of the primary concerns is that adult psychopathy is thought to be treatment resistant and, there- fore, identifying juveniles as psychopathic might lead the criminal justice system to view those individuals as simi- larly untreatable perhaps leading to a premature dismissal of the possibility of rehabilitation that could result in more harsh sentences (Seagrave & Grisso, 2002). Another concern is that characteristics of adults such as psychopathic traits might appear transiently in juveniles (Seagrave & Grisso, 2002) thereby leading to the potential for false labels that
- 6. could carry serious consequences. However, Frick (2002) persuasively argues that psychopathy is not that different from other disorders found in adults that have been applied to children and adolescents (e.g., depression), and a similar argument could be made for ASPD. The goal of the present study was to examine the validity of Adolescent ASPD. To this end, we compared adolescents who met the criteria for ASPD to those with CD only on robust correlates of antisocial behavior to show that CD and Adolescent ASPD are distinct in important ways and may therefore convey different information about an adolescent’s antisocial behavior problem. Alcohol and drug dependence (Cottler et al., 1995; Helzer & Pryzbeck, 1988; Hesselbrock, 1991; Taylor & Carey, 1998), depression (Moffitt et al., 2001; Pager, 1998; Schuckit, 1986), and attention-deficit/hyperactivity disorder (ADHD) (Disney et al., 1999; Lahey et al., 1995) are positively associated with antisocial behavior across gender. A differential rate of association of these disorders with ASPD versus CD in ado- lescents would indicate potential differences with regard to psychological impairment that could impact the severity of antisocial behavior (e.g., alcohol or drug dependence serving to increase antisocial behavior) and/or the complexity of the treatment plan (e.g., more issues to address in treatment). Cognitive functioning has also been linked to antisocial behavior. Specifically, verbal intelligence is inversely related to antisocial behavior in children and adolescents (White et al., 1994), and low verbal IQ predicts persistence of antiso- cial behavior (Farrington & Hawkins, 1991; Simonoff et al., 2004). Furthermore, antisocial behavior is often associated with a marked performance IQ > verbal IQ (PIQ > VIQ) discrepancy (Cornell & Wilson, 1992; Snow & Thurber, 1997). Given these findings, it may be the case that ASPD (characterized by persistence of antisocial behavior from
- 7. adolescence into adulthood) is underlied, in part, by greater VIQ deficits than CD that does not develop into ASPD. Antisocial behavior has also been robustly linked to de- viance in peer groups (e.g., Jessor et al., 1995; Simons et al., 1994) and to poor academic functioning (Patterson, 1986). Antisocial peers might serve both as models for and facil- itators of antisocial behavior, which suggests that they can impact the likelihood that antisocial behavior will persist (as in the case of ASPD) or desist (as in the case of CD only). The persistence associated with ASPD might also translate into a particularly poor level of academic functioning given that the effects of early school problems likely compound over time. The potential differential association of deviant peers and academic functioning with ASPD versus CD only might have important impacts on family functioning (e.g., greater family conflict surrounding highly deviant friends and bad Springer 1050 J Youth Adolescence (2007) 36:1048–1057 grades among adolescents with ASPD) as well as treatment plans (e.g., need to focus attention on academic improve- ments and perhaps remedial education for adolescents with ASPD). Finally, the influence of genes on CD and ASPD is well documented and a recent study shows that a similar set of ge- netic factors contributes to both disorders in men and women but adult symptoms of ASPD have an overall greater genetic influence than CD (Kendler et al., 2003). Thus, ASPD and CD that does not progress into ASPD might have different etiological structures that could help explain the difference
- 8. in their course (i.e., greater genetic influence on ASPD might contribute to persistence of antisocial behavior). Hypotheses Our hypothesis was that Adolescent ASPD is a valid con- struct, and this was examined in two ways. First, we com- pared an Adolescent ASPD group, a CD Only group (who had a CD diagnosis, but not ASPD), and a Control group (with no CD or ASPD diagnosis) on robust correlates of an- tisocial behavior. We had the following specific predictions for these comparisons: 1. Boys and girls in the Adolescent ASPD group will show significantly higher rates of alcohol and drug dependence, ADHD, and depression than adolescents in the CD Only and Control groups. 2. Boys and girls in the Adolescent ASPD group will show significantly lower verbal IQ and a greater PIQ > VIQ dis- crepancy than those in the CD Only and Control groups. 3. Boys and girls in the Adolescent ASPD group will show significantly greater peer group deviance and poorer aca- demic functioning (lower grades, more suspensions and absences) than those in the CD Only and Control groups. 4. Boys and girls in the Adolescent ASPD group will show a higher rate of paternal ASPD than the other groups. Second, we compared the Adolescent ASPD group to a young adult group who had ASPD using all DSM criteria (including the age of onset criterion) in order to show that the ASPD diagnosis conveys similar clinical characteristics whether it is assigned before or after age 18. This is important in showing that the ASPD diagnosis could be used before
- 9. age 18 to help identify adolescents at risk for following a more persistent antisocial behavior trajectory. Method Participants Participants were drawn from a sample of 578 16- to 18- year-old male (M = 17; SD = .45) and 674 female (M = 17; SD = .65) same-sex monozygotic (MZ) and dizygotic (DZ) twin pairs participating in the Minnesota Twin Family Study (MTFS). Twin pairs were identified through Minnesota state birth records for the years 1972 through 1977 (male ado- lescent cohort) and 1975 through 1979 (female adolescent cohort). Exclusion criteria were minimal (twins could not be adopted nor could they have a physical or intellectual disability as determined through a detailed phone interview with the twins’ mother). After complete description of the study to participants, parents provided informed written con- sent for their own and their minor child’s participation in the MTFS. Children under 18 provided written assent to partic- ipate. Families were paid for their participation. The racial composition of the entire MTFS sample (98% white) is con- sistent with the demographics of Minnesota in the birth years sampled. Twins were recruited for the first follow-up assess- ment at an average age of 20 (i.e., approximately 3 years after the intake assessment). Most (88%) of the 1,252 twins com- pleted diagnostic measures for that follow-up assessment. Participants were grouped based on diagnoses of CD and ASPD from clinical interviews conducted at ages 17 (intake) and 20 (first follow-up). At both ages, symptoms of ASPD (including symptoms of CD present prior to age 15) were assessed independently in each twin using the Structured Clinical Interview for DSM-III-R Personality Disorders
- 10. (SCID-II; Spitzer et al., 1987). (The DSM-III-R criteria were the diagnostic standard at the time of the assessments.) Highly trained interviewers who had at least a B.A. degree in psychology conducted all interviews. At age 17 only, symp- toms of CD were also assessed via the Diagnostic Interview for Children and Adolescents – Revised (DICA-R-P) (Her- janic & Reich, 1982; Reich & Welner, 1988) administered to the twins’ mother in an independent interview. A case con- ference team of two advanced clinical psychology graduate students assigned symptoms of disorders after reviewing the interview data from a particular informant (i.e., symptoms reported by the mother were assigned independently from those reported by the twin for any diagnosis with both informant reports). Separate case conferences were used to assign symptoms for members of each twin pair and teams were blind to the co-twin’s diagnostic status and to the pair’s zygosity during the case conferences. Symptoms assigned during case conferences were entered into a computer and algorithms (to implement DSM-III-R criteria) were employed to produce study diagnoses. When reports from both the mother and the twin were available, a symptom was counted toward the diagnosis if either informant endorsed it, as is typical in a best-estimate diagnostic strategy (Bird, Gould, & Staghezza, 1992). At age 20, the twin was the sole informant for all interviews and therefore diagnoses at that assessment were based solely on the twin’s report. Seventy-seven participants (25 girls; 32.5%) comprised the CD Only group, which had a probable or definite (2 or Springer J Youth Adolescence (2007) 36:1048–1057 1051
- 11. more symptoms plus duration) CD diagnosis at age 17 and no more than one adult antisocial behavior (AAB) symptom from the ASPD criteria through age 20. Sixty-four partic- ipants (17 girls; 26.6%) comprised the Adolescent ASPD group, which had a probable or definite ASPD diagnosis (3 or more AAB symptoms and a probable or definite CD diag- nosis) at age 17. Twenty men (but no women) were identified as having probable or definite ASPD when all DSM-III-R criteria were applied (including age at onset). These men, who comprised the ASPD group, had CD at age 15 but did not meet (probable or definite) ASPD criteria until age 20. The inclusion of probable cases helped maximize the num- ber of participants classified, but did not greatly inflate the rates of CD (6.2%) or ASPD (6.7%) in the overall sam- ple. Table 1 presents the rates of endorsement of CD and AAB symptoms for each group. Three hundred forty Con- trols (274 girls; 81%) were identified who had no CD or AAB symptoms through age 20. Note that eight of the Adolescent ASPD group members were 18 at the time of the “age 17” assessment because there was not enough time in a year for all pairs to visit at age 17. Analyses were rerun with the eight 18-year-olds removed with similar findings, therefore, results for the full Adoles- cent ASPD group are reported. Also, there was a potential concern about comparing a disproportionately female con- trol group to two largely male antisocial behavior disorder groups. Thus, a control group with a similar proportion of girls to that found in the disordered groups was created by randomly selecting 50 girls from the 274 control girls and combining them with the 66 control boys (N = 116; 43% girls). All analyses were rerun with this control group and results were quite similar, therefore, the results using the full Control group (N = 341) are reported. Approximately 30–60% of each group was comprised of
- 12. MZ or DZ twin pairs representing related individuals within the group: Control (102 pairs or 204 related individuals), CD Table 1 Symptom characteristics of the conduct disorder only (CD only), adolescent antisocial personality disorder (adolescent ASPD), and antisocial personality disorder (ASPD) groups CD Only (n = 77) Adolescent ASPD (n = 64) ASPD (n = 20) Symptom (DSM-III-R) N % N % N % Conduct disorder (CD) Stolen without confrontation 14 18.2 37 57.8 12 60.0 Ran away overnight 3 3.9 9 14.1 1 5.0 Often lies 21 27.3 35 54.7 11 55.0 Set fires deliberately 1 1.3 5 7.8 1 5.0 Often truant 6 7.8 29 45.3 6 30.0 Broken into home/car 4 5.2 23 35.9 5 25.0 Destroyed property 26 33.8 32 50.0 14 70.0 Cruel to animals 31 40.3 17 26.6 7 35.0 Used weapon in a fight 16 20.8 13 20.3 6 30.0 Often initiates physical fights 35 45.5 31 48.4 9 45.0 Stolen with confrontation 1 1.3 5 7.8 1 5.0 Cruel to people 4 5.2 17 26.6 5 25.0 Adult Antisocial Behavior (AAB) Inconsistent work behavior 2 2.6 41 64.1 10 50.0 Fails to conform to social norms 1 1.3 46 71.9 17 35.0 Irritable and aggressive 4 5.2 40 62.5 13 65.0 Fails to honor financial debts 0 0 5 7.8 4 20.0 Fails to plan ahead/impulsive 0 0 3 4.7 1 5.0 No regard for the truth 2 2.6 38 59.4 9 45.0 Reckless disregard for safety 28 36.4 53 82.8 19 95.0 Irresponsible parent 0 0 0 0 0 0 Non-monogamous 0 0 1 1.6 0 0 Lacks remorse 1 1.3 28 43.8 4 20.0
- 13. Mean SD Mean SD Mean SD No. of CD Symptoms 2.56 1.21 4.39 2.09 4.25 1.45 No. of AAB Symptoms 0.49 0.50 3.98 1.02 3.85 0.93 Note. CD Only group members were allowed to have one AAB symptom at 17 or 20, and the table reflects AAB symptoms endorsed at either age. For the Adolescent ASPD group, the table reflects symptoms reported at age 17, when that group met criteria for ASPD. For the ASPD group, the rates for CD are from age 17 and rates for AAB are from age 20 given that they had a CD diagnosis at 17 but did not meet the AAB component of ASPD until age 20. Springer 1052 J Youth Adolescence (2007) 36:1048–1057 Only (10 pairs), Adolescent ASPD (11 pairs), and ASPD (3 pairs). As indicated below, steps were taken to account for this non-independence of observations in the analyses. Measures Co-morbid disorders At ages 17 and 20, twins were independently interviewed with the expanded Substance Abuse Module (SAM) of the Composite International Diagnostic Interview (Robins et al., 1988) to assess lifetime criteria of substance use disorders including nicotine dependence and abuse and dependence
- 14. on alcohol, cannabis, amphetamines, opioids, sedatives, co- caine, PCP, hallucinogens, and inhalants. Lifetime criteria of major depression were assessed using the Structured Clinical Interview for DSM-III-R (SCID; Spitzer et ., 1987) at ages 17 and 20. At age 17, twins reported their symptoms of ADHD via the DICA-R and mothers reported on the twins’ ADHD, depression, and substance use disorders via the DICA-R-P. The case conference procedure described above was used to assign symptoms of ADHD, depression, and substance use disorders, and computer algorithms implementing DSM-III- R criteria were used to determine diagnoses. At age 17, diag- noses were derived using the aforementioned best estimate strategy. At age 20, diagnoses were based solely on the twin’s report. Independent case conference teams (blind to the orig- inal team’s symptom ratings and to the study diagnoses) rated a random sample of cases and produced diagnostic reliability coefficients (kappa) of .75 or greater. Co-morbid diagnoses were considered present if criteria were met at a definite diagnostic level. Alcohol, nicotine, and cannabis use disorders were examined separately from all other drug classes because they were the most common; the remaining drugs were combined into an illicit abuse (i.e., criteria met for abuse of any illicit drug other than cannabis) and an illicit dependence (criteria met for dependence on any illicit drug other than cannabis) variable. Cognitive functioning Verbal IQ (VIQ) was estimated from the Information and Vo- cabulary subtests and performance IQ (PIQ) was estimated from the Picture Arrangement and Block Design subtests of the Wechsler Adult Intelligence Scale – Revised (WAIS- R; Wechsler, 1981) administered at age 17. The PIQ > VIQ discrepancy reflected the simple difference between PIQ and VIQ.
- 15. Peer group At age 17, each twin nominated up to four teachers to comp- lete a teacher rating form modeled after the Connors Teacher Rating Scale (Connors, 1969; Pelham et al., 1989) and the Rutter Child Scale B (Rutter, 1967). The Bad Peers scale included four descriptors (tough, dangerous, rebellious, and involved with alcohol and drugs) rated on a 5-point scale. Ratings were averaged across teachers and high scores indi- cated greater levels of the four descriptors in the twin’s peer group (Alpha = .77). Academic functioning Official school records are not obtained by the MTFS given the variability in grading procedures (e.g., assignment of grades versus some other evaluative mark) and standards (e.g., using something other than a 4-point academic scale) used across school districts from which twins were drawn. As such, at age 17, teachers completing the teacher rating form (described above) also rated twins’ academic achieve- ment in four areas: English, Math, Science, and Social Stud- ies. Achievement in each area was rated on an academic grade scale of A (coded 4) to F (coded 0). Ratings were averaged across teachers with high scores reflecting better grades. Teachers also reported the number of school suspen- sions and unexcused absences, and ratings were averaged across teachers within each of these variables. Paternal history of ASPD At age 17, twins participated in the MTFS with their parents. Biological fathers were independently interviewed regard- ing symptoms of ASPD using the SCID-II. The consensus
- 16. case conference procedure described above was applied to diagnostic data from fathers to arrive at study diagnoses of ASPD. For each twin, paternal history of ASPD was denoted as either positive (lifetime probable or definite diagnosis of ASPD present in biological father) or negative (no lifetime diagnosis of ASPD in biological father). (Our decision to focus on paternal ASPD was a practical one based on initial examination of the data that showed that only four biologi- cal mothers of adolescents assigned to any of the groups met criteria for ASPD thus precluding an analysis of maternal ASPD effects.) Analyses In the first test of the study hypothesis, the Adolescent ASPD, CD Only, and Control groups were compared on rates of co-morbid diagnoses at age 17 using chi-square tests with one twin from each twin pair within a group randomly se- lected and removed prior to analysis to meet the requirement of independence of observations. To correct for the number of tests conducted, alpha was set to .01 for the omnibus chi-square tests. Alpha was set to .05 (1-tailed) for follow-up chi-square contrasts following significant omnibus tests. Springer J Youth Adolescence (2007) 36:1048–1057 1053 The three groups were also compared on VIQ score and PIQ > VIQ discrepancy, Bad Peers scale scores, and aca- demic achievement in analyses using the Mixed procedure in SPSS 12.0 which provided a multilevel framework that allowed twins to be nested within families and thus allowed all cases to be included in the analyses. A mixed linear model
- 17. was fit for each cognitive variable using restricted maximum likelihood estimation. Models included fixed effects in a full factorial model with tests for group, gender, and the group × gender interaction. The effect of twins nested within families was modeled as a random effect in each model. Alpha was set to .01 for the omnibus F-tests, and follow-up contrasts to significant effects were conducted using the Bonferroni test with alpha set to .05 (1-tailed). Initial examination of the sus- pensions and unexcused absences variables revealed highly positively skewed distributions that were not amenable to transformations to improve normality. Thus, these two variables were examined using non-parametric Kruskal Wallis omnibus and follow-up tests. Such tests do not lend themselves to nesting and, therefore, one twin was removed from each pair within a group for the analyses. Alpha was set to .025 (.05/2) for the omnibus tests and .05 for follow-up tests. Finally, groups were compared on paternal ASPD history using a chi-square test with one twin from each twin pair within a group removed and alpha was set to .05. The second test of the study hypothesis entailed a compar- ison of the Adolescent ASPD and the ASPD groups. Groups were first compared on their rates of endorsement of each CD and AAB symptom using chi-square tests with co-twins removed as described above. Groups were then compared on rates of co-morbid disorders at age 17 (when the Adolescent ASPD group first met criteria for ASPD) and at age 20 (when the ASPD group first met criteria for ASPD) using chi-square tests with co-twins removed as indicated previously. This strategy afforded an examination of the clinical problems that precede, occur with, and follow an ASPD diagnosis. The two groups were then compared on VIQ and PIQ > VIQ discrepancy, Bad Peers scores, and academic achievement using the Mixed procedure in SPSS 12.0. Models included a fixed effect for group and the effect of twins nested within families as a random effect (there were no gender effects in
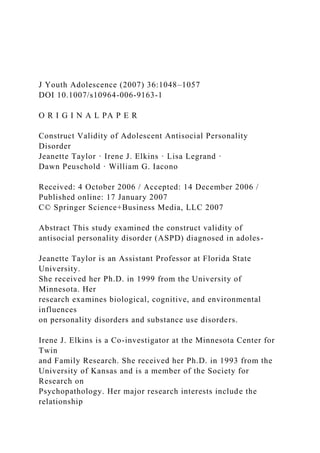
- 18. the models because the ASPD group was all male). Next, dif- ferences in school suspensions and unexcused absences were examined with Mann-Whitney non-parametric tests with co- twins removed. Finally, groups were compared on paternal ASPD history using a chi-square test with co-twins removed. The alpha for all tests was set to .05 (2-tailed). Results The Adolescent ASPD group was distinct from the CD Only group in most analyses, largely supporting our hy- potheses. As expected, the omnibus chi-square test was significant (p < .001) for each disorder: ADHD (χ 2 [2] = 24.13), depression (χ 2 [2] = 38.81), alcohol abuse (χ 2 [2] = 220.06), alcohol dependence (χ 2 [2] = 153.41), nicotine dependence (χ 2 [2] = 164.73), cannabis abuse (χ 2 [2] = 125.48), cannabis dependence (χ 2 [2] = 105.75), illicit drug abuse (χ 2 [2] = 46.15), and illicit drug depen- dence (χ 2 [2] = 28.51). Fig. 1 presents the percent of each group with a co-morbid diagnosis at age 17. As expected, the Adolescent ASPD group had a significantly (p < .001) greater rate of depression and all substance use disorders than the CD Only and Control groups (which did not dif- fer significantly). Both the CD Only and Adolescent ASPD group differed significantly (p < .007) from Controls (but not from each other) on rate of ADHD. (To investigate pos- sible gender differences, analyses were rerun separately by gender and results were unchanged although a few effects were significant at p < .05 instead of p < .01 likely due to the reduced power of the within-gender analyses.) Table 2 presents a summary of the group comparisons on the cognitive, peer, academic, and paternal ASPD vari- ables. Some participants were missing data on some of the variables resulting in the variable df for tests reported in the
- 19. table. The group × gender interaction was non-significant for VIQ, PIQ > VIQ, Bad Peers, and all academic achieve- ment variables. The main effect for group was significant (p < .001) for all variables except VIQ, English, and Math (the latter two approached significance at p < .02, which was just short of the adopted alpha of .01). As expected, the Adolescent ASPD group was significantly (p < .05) dif- ferent from the Control and CD Only groups (which were not significantly different) on PIQ > VIQ, Bad Peers, and Science grades. The Adolescent ASPD group differed sig- nificantly only from Controls on Social Studies grades and paternal history of ASPD. The Kruskal Wallis test was sig- nificant at p < .02 for school suspensions (χ 2 [2] = 8.05) and for unexcused absences (χ 2 [2] = 35.01). As expected, the Adolescent ASPD group was significantly higher in mean rank than the CD Only and Control groups, who differed sig- nificantly (p = .048) only on unexcused absences (with the CD Only group having a higher mean rank than the Control group). The second test also supported our hypothesis in that the Adolescent ASPD group was not significantly different from the ASPD group in most analyses. As expected, groups did not differ significantly on their rates of endorsement of the individual CD or AAB symptoms (see Table 1), suggesting that adolescents and young adults diagnosed with ASPD endorse similar kinds of symptoms. Also as expected, the groups did not differ significantly on any diagnosis at age 20 and differed at age 17 on alcohol abuse (χ 2 [1] = 8.90, p = .003), nicotine dependence (χ 2 [1] = 9.37, p = .002), and cannabis (χ 2 [1] = 5.49, p = .02) where the Adolescent Springer
- 20. 1054 J Youth Adolescence (2007) 36:1048–1057 0 10 20 30 40 50 60 70 80 90 100 AD HD De pr es sio n Al
- 23. D ep en de nc e % o f G ro u p w ith D ia g n o si s Control (n = 237-8) CD Only (n = 76-7) Adolescent ASPD (n = 51-3) Fig. 1 Rate of co-morbid
- 24. diagnoses in the control, conduct disorder (CD) only, and adolescent antisocial personality disorder (Adolescent ASPD) groups at age 17. Data were missing for a few cases on one or more disorders resulting in slightly variable group Ns. ADHD = attention-deficit/ hyperactivity disorder. Illicit drug abuse and dependence refer to abuse and dependence on illicit drugs other than cannabis. The vertical line with crossbars represents the 95% CI for the percent estimate ASPD group had the higher rates of co-morbidity. Figure 2 presents the rate of co-morbid diagnoses for each group at ages 17 and 20. As expected, the two ASPD groups did not differ signifi- cantly on any of the cognitive, peer, academic achievement, or paternal history variables. Table 2 presents a summary of those analyses. Note that there were two members of the Adolescent ASPD group with co-twins in the ASPD group, which might bias the result toward our null expectation given that members of a twin pair have identical data for paternal history. The analysis for the paternal ASPD history vari- able was re-run after removing the two Adolescent ASPD twins who had ASPD co-twins and the results were nearly identical (the rate of paternal ASPD went from 21.7% in the Adolescent ASPD group to 20.5% and the χ 2 remained non-significant). Finally, the Adolescent ASPD and ASPD groups did not differ significantly on school suspensions or
- 25. unexcused absences. Discussion Adolescent antisocial behavior is an important topic of re- search given its negative consequences to both families and Table 2 Summary of group comparisons on cognitive functioning, peer group, academic achievement, and paternal ASPD history Control vs. CD Only vs. Adolescent ASPD Adolescent ASPD vs. ASPD Control CD Only Adolescent ASPD ASPD F (df) Mean (SE) Mean (SE) Mean (SE) F (df) Mean (SE) VIQ 2.67 (2, 472.8) 98.18 (0.99) 95.80 (1.59) 93.47 (1.96) 0.16 (1, 66.6) 92.62 (2.74) PIQ > VIQ 73.36 (2, 439.9)∗ ∗ ∗ 7.64 (1.25)a 8.79 (2.13)a 18.44 (2.55)b 0.30 (1, 67.1) 21.10 (3.64) Bad Peers 51.51 (2, 313.2)∗ ∗ ∗ 0.14 (0.10)a 0.15 (0.02)a 0.43 (0.03)b 0.56 (1, 52.0) 0.39 (0.05) Achievement English 4.19 (2, 270.3) 3.15 (0.06) 3.09 (0.10) 2.54 (0.19) 1.56 (1, 38.8) 1.92 (0.25) Math 3.94 (2, 226.3) 2.98 (0.08) 2.96 (0.15) 2.32 (0.23) 0.41 (1, 38.0) 2.15 (0.23) Science 10.33 (2, 241.0)∗ ∗ ∗ 3.07 (0.08)a 2.85 (0.13)a 2.07 (0.21)b 0.52 (1, 2.5) 2.09 (0.20) Social Studies 6.69 (2, 261.3)∗ ∗ ∗ 3.19 (0.07)a 2.91 (0.12)a,b 2.55 (0.18)b 2.61 (1, 40.8) 1.94 (0.23)
- 26. χ 2 (df) % (95% CI) % (95% CI) % (95% CI) χ 2 (df) % (95% CI) Paternal ASPD 12.79 (2)∗ ∗ 5.5a(2.89–9.46) 9.5a,b(3.58–19.59) 21.7b(10.95– 36.36) 0.15 (1) 16.7(2.09–48.41) Note. Groups within a row that do not share a superscript differed at p < .05. For the Adolescent ASPD vs. ASPD comparisons, none of the effects were statistically significant (all ps > .11). The Bad Peers scores were log-transformed (log10 [x + 1]) for analyses and means are presented in log-transformed units. The academic achievement variables were rated on a grading scale of A (4) to F (0). CD = conduct disorder; ASPD = antisocial personality disorder; VIQ = verbal IQ; PIQ = performance IQ; Paternal ASPD refers to presence vs. absence of a lifetime diagnosis of ASPD in the twin’s biological father. The entries in the table reflect the percent of each group with ASPD present in the biological father. ∗ ∗ p < .002; ∗ ∗ ∗ p < .001. Springer J Youth Adolescence (2007) 36:1048–1057 1055 0 10 20 30
- 30. ro u p w ith D ia g n o si s Adolescent ASPD (n = 51-3) ASPD (n = 17) B) Co-morbid Diagnoses at Age 20 A) Co-morbid Diagnoses at Age 17 0 10 20 30 40 50
- 34. p w ith D ia g n o si s Adolescent ASPD (n = 35-9) ASPD (n = 16-7) Fig. 2 Rate of co-morbid diagnoses in the adolescent antisocial per- sonality disorder (Adolescent ASPD) and antisocial personality disor- der (ASPD) groups at age 17 and age 20. Data were missing for a few cases on one or more disorders resulting in slightly variable group Ns. ADHD = attention-deficit/hyperactivity disorder. Illicit drug abuse and dependence refer to abuse and dependence on illicit drugs other than cannabis. The vertical line with crossbars represents the 95% CI for the percent estimate society. The results of the present study suggest that Adoles-
- 35. cent ASPD is a valid construct that could identify adolescents with non-normative antisocial behavior. This might better enable parents, clinicians, and teachers to reach out early to adolescents who might be on a more persistent pathway for antisocial behavior. Adolescent ASPD was found to be distinct from CD in terms of co-morbid psychiatric diagnoses, cognitive func- tioning, peer deviance, and academic performance. More- over, because no evidence of an interaction between gender and group was found, Adolescent ASPD appears to be a valid construct for both genders. Thus, loosening the DSM criteria for ASPD to allow diagnosis among adolescents could provide a means to identify adolescents at risk for persistent antisocial behavior. Consistent with the large body of literature linking CD to other childhood behavioral disorders, both CD and Ado- lescent ASPD were significantly associated with ADHD in Springer 1056 J Youth Adolescence (2007) 36:1048–1057 this study. But, as predicted, boys and girls with Adolescent ASPD had significantly higher rates of depression and sub- stance use disorders as compared to those with CD Only. However, the present findings are not inconsistent with pre- vious studies relating CD to substance use disorders (e.g., Disney et al., 1999) as members of the Adolescent ASPD group also had CD. If groups had been selected simply on CD status, then the “CD group” would have had high rates of substance use disorders, but our results suggest that the
- 36. elevated rates would have been attributable to the members with Adolescent ASPD. This suggests that the assessment of ASPD in adolescents could identify those at greatest risk for substance use disorders or, stated another way, restricting the ASPD diagnosis to those over age 18 may result in a missed opportunity at identifying antisocial adolescents that are at high risk for early-onset substance use disorders. An important finding was that, as expected, Adolescent ASPD and CD were distinct in many ways. Equally impor- tant was the finding that an ASPD diagnosis—regardless of when it was assigned—was associated with substantial rates of co-morbid psychiatric disorder in adolescence and early adulthood. In addition, the Adolescent ASPD and ASPD groups showed a similar PIQ > VIQ discrepancy, the mag- nitude of which ( >18 points) is considered not only statis- tically significant but also abnormal (Hsu et al., 2000) and corroborates the idea that cognitive deficits are associated with persistent forms of antisocial behavior (Moffitt, 1993). In addition, the Adolescent ASPD and ASPD groups showed similarly deviant peer groups and similarly poorer academic functioning (in both achievement and discipline) at age 17. These results suggest that cognitive deficits in verbal rela- tive to performance IQ, affiliation with deviant peers, and poorer academic functioning may contribute to the devel- opment and/or maintenance of persistent antisocial behavior that could be identified in adolescents by applying ASPD criteria. Our expectation for a statistically significant difference between the CD Only and Adolescent ASPD groups on pater- nal ASPD history was not supported. However, the data were ordered in the expected direction, with the rate of paternal ASPD for the adolescent ASPD group more than double that seen in the CD Only group. Only the Adolescent ASPD group showed a high rate of substance use disorders—another form
- 37. of externalizing disorder. Thus, the biological risk transmit- ted in families may primarily manifest as an antisocial be- havior disorder in children (CD or ASPD), but other factors (e.g., deviant peer group, cognitive functioning) then con- tribute to the continuity of the antisocial behavior (CD vs. ASPD) and perhaps also to the likelihood that other external- izing disorders manifest (e.g., substance use disorders; see Krueger et al., 2002). The major strengths of this study included the use of a mixed gender sample with groups carefully selected on CD and ASPD diagnostic status. Analyses of gender were con- ducted wherever possible and showed similar results for boys and girls. Structured clinical interviews provided excellent measurement of CD, ASPD, and co-morbid disorders. The use of teachers as raters of peer group and academic func- tioning served to avoid the complete reliance on self-reports that plagues many studies. It also likely resulted in less biased information than might have been obtained through self or even parent reports on those measures. Finally, the use of lon- gitudinal data allowed us to compare individuals diagnosed with ASPD in adolescence to those who met the criteria in early adulthood. The longitudinal data also allowed us to examine prospectively the co-morbidity between Adolescent ASPD, depression, and substance use disorders. Limitations of the study also existed and included the use of a predominantly white sample, indicating that caution be used in generalizing our results to non-white populations. Certainly, additional work is needed to confirm and extend the present findings. In addition, though the rates of CD and ASPD were consistent with those found in the general popu- lation, our ASPD group size was modest. Thus, confidence in our results would be enhanced with replications using larger samples (e.g., obtained from clinics where the disorders are
- 38. found at higher rates). Such replications would also bolster confidence in the predicted null findings given that null re- sults could arise from actual similarity across groups but also from methodological or statistical anomalies. Finally, we acknowledge that teachers might not be able to provide the most comprehensive rating of peer group given their lim- ited context of interaction with the adolescents. Moreover, it is possible that the teacher’s perceptions of the peer group could affect their rating of academic performance (e.g., per- ception of a negative peer group might lead to more negative academic evaluations). In summary, this study suggests that Adolescent ASPD is a valid construct that appears to provide incremental clinical utility beyond what is gleaned from a CD diagnosis alone. Given the high prevalence of antisocial behavior during ado- lescence, it may be difficult for parents and professionals alike to determine whether an adolescent is exhibiting nor- mative, transitory antisocial behavior or whether he/she is at risk for a more persistent course. The application of the ASPD criteria to adolescents under the age of 18 appears to identify a clinically important subgroup of antisocial ado- lescents who might benefit most from interventions to help deter them from a continued course of antisocial behav- ior. Such applications, however, should be made cautiously until further research confirms the present findings given the potential dangers that diagnostic labels can bring. Acknowledgements The present study was supported in part by National Institute of Drug Abuse grant DA 05147 and National In- stitute on Alcohol Abuse and Alcoholism grant AA09367. Springer
- 39. J Youth Adolescence (2007) 36:1048–1057 1057 References Barry CT, Frick PJ, DeShazo TM, McCoy MG, Ellis M, Loney BR (2000) The importance of callous-unemotional traits for extrnd- ing the concept of psychopathy to children. J Abnorm Psychol 109:335–340 Bird HR, Gould MS, Staghezza B (1992) Aggregating data from multi- ple informants in child psychiatry epidemiological research. J Am Acad Child Adolesc Psychiatry 31:78–85 Blair RJR (1999) Responsiveness to distress cues in the child with psychopathic tendencies. Pers Individ Differences 27:135– 145 Christian RE, Frick PJ, Hill NL, Tyler L, Frazer DR (1997) Psychopathy and conduct problems: II. Implications for subtyping children with conduct problems. J Am Acad Child Adolesc Psychiatry 36:233– 241 Conners CK (1969) A teacher rating scale for use in drug studies with children. Am J Psychiatry 126:152–156 Cornell D, Wilson LA (1992) The PIQ > VIQ discrepancy in violent and nonviolent delinquents. J Clin Psychol 48:256–261
- 40. Cottler LB, Price RK, Compton WM, Mager DE (1995) Subtypes of adult antisocial Behavior among drug abusers. J Nerv Ment Dis 183:154–161 Disney ER, Elkins IJ, McGue M, Iacono WG (1999) Effects of ADHD, conduct disorder, and gender on substance use and abuse in ado- lescence. Am J Psychiatry 156:1515–1521 Farrington DP, Hawkins JD (1991) Predicting participation, early onset and later persistence in officially recorded offending. Criminal Behav Ment Health 1:1–33 Frick PJ (2002) Juvenile psychopathy from a developmental perspec- tive: Implications for construct development and use in forensic assessments. LawHum Behav 26:247–253 Frick PJ, Ellis M (1999) Callous-unemotional traits and subtypes of conduct disorder. Clin Child Fam Psychol Rev 2:149–168 Frick PJ, Lilienfeld SO, Ellis M, Loney B, Silverthorn P (1999) The association between anxiety and psychopathy dimensions in chil- dren. J Abnorm Child Psychol 27:383–392 Helzer JE, Pryzbeck TR (1988) The co-occurrence of alcoholism with other psychiatric disorders in the general population and its impact on treatment. J Stud Alcohol 49:219–224
- 41. Herjanic B, Reich W (1982) Development of a structured psychiatric interview for children: Agreement between child and parent on individual symptoms. J Abnorm Child Psychol 10:307–324 Hesselbrock M (1991) Gender comparison of antisocial personality disorder and depression in alcoholism. J Subst Abuse 3:205– 220 Hsu LM, Hayman J, Koch J, Mandell D (2000) Relation of statistically significant, abnormal, and typical WAIS-R VIQ-PIQ discrepancies to full scale IQs. Eur J Psychol Assess 16:107–114 Jessor R, Van Den Bos J, Vanderryn J, Costa FM, Turbin MS (1995) Protective factors in adolescent problem behavior: Moderator ef- fects and developmental change. Dev Psychol 31:923–933 Kendler KS, Prescott CA, Myers J, Neale MC (2003) The structure of genetic and environmental risk factors for common psychiatric and substance use disorders in men and women. Arch Gen Psychiatry 60:929–937 Krueger RF, Hicks BM, Patrick CJ, Carlson SR, Iacono WG, McGue M (2002) Etiologic connections among substance dependence, antisocial behavior, and personality: Modeling the externalizing spectrum. J Abnorm Psychol 111:411–424
- 42. Lahey BB, Loeber R, Hart EL, Frick PJ, Applegate B, Zhang Q, Green SM, Russo MF (1995) Four-year longitudinal study of conduct disorder in boys: Patterns and predictors of persistence. J Abnorm Psychol 104:83–93 Lynam DR (2002) Fledgling psychopathy: A view from personality theory. Law Hum Behav 26:255–259 Moffitt TE (1993) Adolescence-limited and life-course- persistent an- tisocial behavior: A developmental taxonomy. Psychol Bull 100:674–701 Moffitt TE, Caspi A (2001) Childhood predictors differentiate life- course persistent and adolescence-limited antisocial pathways in males and females. Dev Psychopathol 13:355–376 Moffitt TE, Caspi A, Rutter M, Silva PA (2001) Sex differences in antisocial behavior (pp. 135–150). Cambridge University Press, Cambridge, UK O’Brien BS, & Frick PJ (1996) Reward dominance: Associations with anxiety, conduct problems, and psychopathy in children. J Abnorm Child Psychol 24:223–240 Pajer KA (1998) What happens to “bad” girls? A review of the adult outcomes of antisocial adolescent girls. Am J Psychiatry
- 43. 155:862– 870 Patterson GR (1986) Performance models for antisocial boys. Am Psy- cholozist 41:432–444 Pelham WE, Milich R, Murphy DA, Murphy HA (1989) Normative data on the IOWA Conners Teacher Rating Scale. J Clin Child Psychol 18:259–262 Reich W, Welner Z (1988) Diagnostic Interview for Children and Adolescents—Revised: DSM-III-R Version (DICA-R). Washing- ton University, St. Louis. Robins LN (1966) Deviant Children Grown Up. Williams & Wilkins: Baltimore, MD Robins LN, Wing J, Wittchen HU, Helzer JE, Babor TF, Burke J, Farmer A, Jablenski A, Pickens R, Regier DA, Sartorius N, Towle LH (1988) The Composite International Diagnostic Interview: An epidemiologic instrument suitable for use in conjunction with different diagnostic systems and different cultures. Arch Gen Psy- chiatry 45:1068–1077 Rutter M (1967) A children’s behaviour questionnaire for completion by teachers: Preliminary findings. J Child Psychol Psychiatry
- 44. 8:1– 11 Schuckit MA (1986) Genetic and clinical implications of alcoholism and affective disorder. Am J Psychiatry 143(2):140–147 Seagrave D, Grisso T (2002) Adolescent development and the mea- surement of juvenile psychopathy. Law Hum Behav 26:219–239 Simonoff E, Elander J, Holmshaw J, Pickles A, Murray R, Rutter M (2004) Predictors of antisocial personality: Continuities from childhood to adult life. Br J Psychiatry 184:118–127 Simons RL, Wu C-I, Conger RD, Lorenz FO (1994) Two routes to delinquency: Differences between early and late starters in the impact of parenting and deviant peers. Criminology 32:247–275 Snow M, Thurber S (1997) Cognitive imbalance and antisocial person- ality characteristics. J Clin Psychol 53:351–354 Spitzer RL, Williams JB, Gibbon M (1987) Structured clinical interview for DSM-III-R. Biometrics Research Department, New York State Psychiatric Institute, New York Spitzer RL, Williams JB, Gibbon M, First MB (1987) Structured clinical interview for DSM-III-R personality disorders (SCID-II). Biomet- rics Research Department, New York State Psychiatric Institute,
- 45. New York Taylor J, Carey G (1998) Antisocial behavior, substance abuse, and somatization in families of adolescent drug abusers and adolescent controls. Am J Drug Alcohol Abuse 24:635–646 Wechsler D (1981) Manual for the Wechsler Adult Intelligence Scale – Revised (WAIS-R). The Psychological Corporation, San Antonio, TX White JL, Moffitt TE, Caspi A, Jeglum-Bartusch D, Needles DJ, Stouthamer-Loeber M (1994) Measuring impulsivity and exam- ining its relationship to delinquency. J Abnorm Psychol 103:192– 205 Springer Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. << /ASCII85EncodePages false /AllowTransparency false /AutoPositionEPSFiles true /AutoRotatePages /None /Binding /Left /CalGrayProfile (None) /CalRGBProfile (sRGB IEC61966-2.1) /CalCMYKProfile (ISO Coated)
- 46. /sRGBProfile (sRGB IEC61966-2.1) /CannotEmbedFontPolicy /Error /CompatibilityLevel 1.3 /CompressObjects /Off /CompressPages true /ConvertImagesToIndexed true /PassThroughJPEGImages true /CreateJDFFile false /CreateJobTicket false /DefaultRenderingIntent /Perceptual /DetectBlends true /ColorConversionStrategy /sRGB /DoThumbnails true /EmbedAllFonts true /EmbedJobOptions true /DSCReportingLevel 0 /SyntheticBoldness 1.00 /EmitDSCWarnings false /EndPage -1 /ImageMemory 524288 /LockDistillerParams true /MaxSubsetPct 100 /Optimize true /OPM 1 /ParseDSCComments true /ParseDSCCommentsForDocInfo true /PreserveCopyPage true /PreserveEPSInfo true /PreserveHalftoneInfo false /PreserveOPIComments false /PreserveOverprintSettings true /StartPage 1 /SubsetFonts false /TransferFunctionInfo /Apply /UCRandBGInfo /Preserve /UsePrologue false
- 47. /ColorSettingsFile () /AlwaysEmbed [ true ] /NeverEmbed [ true ] /AntiAliasColorImages false /DownsampleColorImages true /ColorImageDownsampleType /Bicubic /ColorImageResolution 150 /ColorImageDepth -1 /ColorImageDownsampleThreshold 1.50000 /EncodeColorImages true /ColorImageFilter /DCTEncode /AutoFilterColorImages false /ColorImageAutoFilterStrategy /JPEG /ColorACSImageDict << /QFactor 0.76 /HSamples [2 1 1 2] /VSamples [2 1 1 2] >> /ColorImageDict << /QFactor 0.76 /HSamples [2 1 1 2] /VSamples [2 1 1 2] >> /JPEG2000ColorACSImageDict << /TileWidth 256 /TileHeight 256 /Quality 30 >> /JPEG2000ColorImageDict << /TileWidth 256 /TileHeight 256 /Quality 30 >> /AntiAliasGrayImages false /DownsampleGrayImages true /GrayImageDownsampleType /Bicubic
- 48. /GrayImageResolution 150 /GrayImageDepth -1 /GrayImageDownsampleThreshold 1.50000 /EncodeGrayImages true /GrayImageFilter /DCTEncode /AutoFilterGrayImages true /GrayImageAutoFilterStrategy /JPEG /GrayACSImageDict << /QFactor 0.76 /HSamples [2 1 1 2] /VSamples [2 1 1 2] >> /GrayImageDict << /QFactor 0.15 /HSamples [1 1 1 1] /VSamples [1 1 1 1] >> /JPEG2000GrayACSImageDict << /TileWidth 256 /TileHeight 256 /Quality 30 >> /JPEG2000GrayImageDict << /TileWidth 256 /TileHeight 256 /Quality 30 >> /AntiAliasMonoImages false /DownsampleMonoImages true /MonoImageDownsampleType /Bicubic /MonoImageResolution 600 /MonoImageDepth -1 /MonoImageDownsampleThreshold 1.50000 /EncodeMonoImages true /MonoImageFilter /CCITTFaxEncode /MonoImageDict << /K -1 >>
- 49. /AllowPSXObjects false /PDFX1aCheck false /PDFX3Check false /PDFXCompliantPDFOnly false /PDFXNoTrimBoxError true /PDFXTrimBoxToMediaBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXSetBleedBoxToMediaBox true /PDFXBleedBoxToTrimBoxOffset [ 0.00000 0.00000 0.00000 0.00000 ] /PDFXOutputIntentProfile (None) /PDFXOutputCondition () /PDFXRegistryName (http://www.color.org?) /PDFXTrapped /False /Description << /DEU <FEFF004a006f0062006f007000740069006f006e007300200066 006f00720020004100630072006f0062006100740020004400690 07300740069006c006c0065007200200036002e000d0050007200 6f006400750063006500730020005000440046002000660069006 c0065007300200077006800690063006800200061007200650020 007500730065006400200066006f0072002000640069006700690 0740061006c0020007000720069006e00740069006e0067002000 61006e00640020006f006e006c0069006e0065002000750073006 100670065002e000d002800630029002000320030003000340020 0053007000720069006e006700650072002d005600650072006c0 061006700200047006d0062004800200061006e00640020004900
- 51. /PageSize [2834.646 2834.646] >> setpagedevice Document 1 of 1 The construct validity of the extraversion subscales of the Myers-Briggs type indicator Author: Zumbo, Bruno D; Taylor, Shannon V ProQuest document link Abstract (Abstract): It seems that the MBTI scales formed a factor of their own and that the EPQ combined with Sociability and Impulsiveness to create the third factor. This comes as no surprise since the EPQ seems intuitively to define extraversion in terms of these two variables. The fact that the MBTI and the EPQ occurred as separate factors suggests that these two measures do not hold identical views on extraversion. However, as evidenced by the factor correlation matrix, Factor 1 (MBTI) and Factor 3 (SOC/EPQ/IMP) had a fairly high correlation. From this one could conclude that although each measure is unique, each contains a high degree of sociability and impulsiveness in its definition. The interfactor correlation among factors one and three was in support of Campbell &Heller (1987). The substantial correlation among factors one and three, and the factor loadings of the SOC, EPQ, and IMP suggested that the MBTI was primarily a sociability measure with a minimal association with impulsivity. This was also in support of Campbell &Heller. The second factor (INF/ANX) yielded only low negative correlations with the other factors and it seems therefore that although it took up 14.5% of the variance, it bears little relation to the other factors. Finally,
- 52. Factor 4, Dominance, which was responsible for only 4.2% of the variance, obtained only a low loading on the MBTI factor in the three - factor solution and was relegated to its own factor in the final four - factor solution. From this first phase of the results it is clear that extraversion cannot be described as entirely unitary. It would appear to be defined in these measures by sociability, impulsiveness, a lack of inferiority and anxiety and the presence of dominance. Part 2 of the results made apparent the possibility of a single higher - order factor capable of bridging the gap between the original four factors. The results did, in fact, indicate that these can be brought together into one interpretable, though less convincing higher - order factor. We may ask at this point whether the results were out of the ordinary and this question is difficult to answer since the study was unique in its approach. To the authors' knowledge, there have been no scale - level analyses of extraversion, though many item - level analyses exist. Such item analyses have revealed that extraversion is composed of many factors. For example, Sipps &Alexander (1987) reported finding three factors of extraversion which were sociability, impulsivity/non - planning and risk - taking / jocularity while [Browne, J.A.] (1971) reported twelve. Certainly, it would be safe to say that sociability has never been far away from any set of results. Apart from being present in most factor analyses of extraversion, it has been shown that the extraversion scale of the MBTI is largely a measure of sociability (Sipps &DiCaudo, 1988). Given that the present study declared MBTI extraversion as the most salient factor, one must wonder about the strength of the relationship between extraversion and sociability. Links: Obtain full text from Shapiro Library Full text: Abstract This paper examined the construct validity of the extraversion
- 53. and introversion subscales of the Myers - Briggs Type Indicator (MBTI) with the Eysenck Personality Questionnaire (EPQ) and the Howarth Personality Questionnaire (HPQ). We further explored the accompanying issue of the unitary nature of extraversion. A conjoint factor analysis undertaken at the scale level produced four first - order factors: Factor 1 - MBTI extraversion/introversion, Factor 2 - Inferiority/ Anxiety, Factor 3 - Sociability/EPQ/Impulsiveness and Factor 4 - Dominance. A subsequent higher - order factor analysis revealed one factor. The results suggested that the MBTI subscales were largely a measure of sociability and that extraversion as represented in these three measures is not, at first glance, unitary although interfactor correlations do exist in varying degrees. Resume http://ezproxy.snhu.edu/login?url=http://search.proquest.com/do cview/220473870?accountid=3783 http://pn8vx3lh2h.search.serialssolution.com/?ctx_ver=Z39.88- 2004&ctx_enc=info:ofi/enc:UTF- 8&rfr_id=info:sid/ProQ:psychologyshell&rft_val_fmt=info:ofi/f mt:kev:mtx:journal&rft.genre=article&rft.jtitle=Canadian%20Jo urnal%20of%20Behavioural%20Science&rft.atitle=The%20cons truct%20validity%20of%20the%20extraversion%20subscales%2 0of%20the%20Myers- Briggs%20type%20indicator&rft.au=Zumbo,%20Bruno%20D;Ta ylor,%20Shannon%20V&rft.aulast=Zumbo&rft.aufirst=Bruno&r ft.date=1993-10- 01&rft.volume=25&rft.issue=4&rft.spage=590&rft.isbn=&rft.bt itle=&rft.title=Canadian%20Journal%20of%20Behavioural%20S cience&rft.issn=0008400X&rft_id=info:doi/ Le present document porte sur la validite conceptuelle des sous - echelles d'extraversion et d'introversion de
- 54. l'indicateur de type de Myers - Briggs (MBTI), ainsi que sur le questionnaire de personnalite d'Eysenck (EPQ) et sur le questionnaire de personnalite de Howarth (HPQ). La question connexe de la nature unitaire de l'extraversion y est egalement examinee. Il est ressorti d'une analyse factorielle mixte de differentes echelles quatre facteurs de rang un: facteur 1 - extraversion/introversion MBTI, facteur 2 - inferiorite/anxiete, facteur 3 - sociabilite/EPQ/impulsivite et facteur 4 - dominance. Un facteur de rang superieur est ressorti d'une analyse subsequente. Les resultats semblent indiquer que les sous - echelles du MBTI constituent, en grande partie, une mesure de la sociabilite et que l'extraversion, representee dans les trois mesures susmentionnees, n'est pas unitaire de prime abord, meme si des correlations existent entre les facteurs a divers degres. There are now several measures of extraversion available to the researcher and practitioner. Of these the Myers - Briggs Type Indicator (MBTI) and its corresponding extraversion - introversion subscales are widely used in Canada and the United States. Workshops and a very lucrative enterprise around the MBTI has evolved in the Canadian and American workplace. However, the construct validity of this measure has not yet been clearly established. There are a few studies which have explored the construct validity of the MBTI. Sipps &Alexander(1987) administered the MBTI and the Eysenck Personality Inventory (EPI) scales and factor analyzed the combined results. (For a comparison of the EPI and the later EPQ, please see Campbell &Reynolds, 1984). In their conjoint item analysis three factors of extraversion emerged: a sociability component, an impulsivity/non - planning component and a liveliness/risk - taking/jocularity component. A synthesis of the reliability and validity studies of the MBTI can be found in Carlyn (1977), Carskadon (1979) or Carlson (1985). Briefly, various studies
- 55. investigated the split - half reliability coefficients for the MBTI scales. They found that the reliability varied from .80 to .90. However, the test - retest tend to be slightly lower but acceptable. Furthermore, Thompson and Borrello (1986) and Tzeng, Outcalt, Boyer, Ware, and Landis (1984) have demonstrated item - level construct validity of the MBTI. That is, the results of the assessments of the MBTI tend to substantiate that it is a reliable instrument that has four distinct psychometric dimensions (validated by item - level factor analysis) that are unidimensional and consistent with the theoretical constructs of the MBTI. Interwoven in the issue of the construct validity of the MBTI extraversion - introversion subscales is the questionable unitary nature of extraversion. As Zumbo and Hubley (1993) state, establishing validity is difficult because it is generally intertwined with the construction and verification of scientific theories. That is, trying to verify a measure is often difficult to separate from trying to verify a theory. Specifically, it is important to confront the question of whether the criterion scales concur in their conception of extraversion. That is, to establish the construct validity of the MBTI, the authors see a need to examine empirically the correlational framework in which these subscales exist. Necessarily, such a task must deal with the innate tension which exists between the conceptual and the concrete forms of a term. Campbell &Reynolds (1984, p. 318) warn that the "actual labels attached to concepts and scales is not at issue; the point is that semantic similarity bears no clear relationship to - and cannot substitute for - empirical similarity". The authors support this statement and seek to clarify, empirically, what it is that is measured in certain extraversion subscales. The purpose of the present paper is directed at the above question although in a somewhat novel fashion. The study is limited to three measures of extraversion: the MBTI,
- 56. the Eysenck Personality Questionnaire (EPQ), and the Howarth Personality Questionnaire (HPQ). To the authors' knowledge, scale - level construct validity analysis of extraversion has not been reported in the literature. Appropriate subscales were combined into one test which enabled us to carry out a factor analysis to investigate the overall factor structure. In doing this, it was possible to examine the construct validity of the MBTI extraversion - introversion subscale and whether extraversion as represented in these tests is fairly unified. Before presenting the current study we will briefly review the literature on the unitary nature of extraversion. Confusion as to what it is that tests of extraversion are measuring stems not only from the area of test construction but from basic problems involved in the definition of extraversion. Taking a brief look at the history of extraversion we see that it has roots as far back as the late seventeenth century when extraversion was used in reference to the mind as a turning outward of one's thoughts toward objects and was at the same time used in chemistry meaning "to render visible or sensible the latent constituents of a substance" (Browne, 1971, p. 7). The word "extraversion" is taken from "extra" meaning "outward" and "vert - ere" meaning "to turn". By contrast, introversion is derived from a different prefix, "intro", meaning "inward" (Browne, 1971, p. 7). Although this definition may provide some insight into the literal meaning of extraversion - introversion, it is not clear what is directed outward or inward. A discussion of the history of extraversion can be found in Eysenck (1970). Early in the present century, research began to emerge which focussed on the biological side of extraversion - introversion (for a recent
- 57. discussion, see Stelmack, 1990). As well, later, ideas were beginning to surface concerning the adaptive qualities of extraversion. Speculation about extraversion occurred on what is now considered a subjective level until the 1930's when factor analysis of test scores enabled a quantitative definition by researchers such as the Guilfords (Guilford &Guilford, 1934). The Guilfords published several articles on their attempts to identify various factors of personality and of extraversion, using factor analysis. Factor analysis of personality dimensions probably attained its height in the 1960's when its use in personality theory was widely popular. FACTORS OF EXTRAVERSION H.J. Eysenck and S.B.G. Eysenck have been important contributors to the study of extraversion. Eysenck and Eysenck (1963) discussed the possibility of sociability and impulsiveness being aspects of extraversion that were not independent. In a subsequent publication (Eysenck &Eysenck, 1967) their factor analysis involved scores on the lemon test (a physiological measure of extraversion) as well as scores on extraversion items and neuroticism items. Their results indicated two uniform factors which were extraversion and neuroticism. Eysenck &Eysenck concluded that for the purposes of the experiment, extraversion was unitary in nature due to its appearance as a unitary factor. Guilford (1977) published a response to a long series of disagreements between himself and the Eysencks concerning the nature of extraversion. Guilford disagreed with Eysenck's notion of extraversion being a second - order factor resting on impulsiveness (factor R in Guilford's scheme) and sociability (factor s). The dispute was based on the fact that in factor analysis, a certain hierarchy of factors exists in which first - order factors are more molecular than second order factors. Having discovered many different first - order factors, the task is to
- 58. assess how they may combine to form second - order factors. In the case of J.P. Guilford and H.J. Eysenck, they both believed that extraversion could exist as a second order factor, but whereas Eysenck believed it to be connected to R and S, Guilford believed it to be more closely tied to R and T (Thoughtfulness). Guilford suggested to Eysenck that his options were either to adopt extraversion as resting on R and T since they were more highly correlated than R and S, or to adopt extraversion as being equivalent to the first order factor R. Guilford believed that R and S were independent and that Eysenck's extraversion factor became "rotated out of existence" (Guilford, 1977, p. 415). EXTRAVERSION AND SOCIAL DESIRABILITY Having looked at extraversion from a theoretical point of view, let us examine some popular conceptions of extraversion. Farley and Goh (1976) instructed students whencompleting a measure of psychoticism, neuroticism and extraversion to answer by relaying either a "good impression" (reflecting social desirability), a "worst impression" (reflecting psychiatric illness) or to answer "normally". Results showed increased scores on psychoticism, neuroticism and introversion for the "worst impression" set. Here we see evidence of a popular belief that introversion reflects mental instability. Furnham and Henderson (1982) conducted a similar study in which subjects who were instructed to give a bad impression on various personality tests demonstrated significantly lower extraversion scores while subjects instructed to give a good impression scored significantly higher on extraversion. These two pieces of research raise the disconcerting possibility of test response bias on measures of extraversion.
- 59. This leads us now to the method used in the present study which is a conjoint factor analysis, a procedure enabling various items or various scales to be combined and analyzed together in the same matrix. For example, Sells, Demaree &Will (1970) used 600 items for their conjoint analysis while Browne and Howarth (1977) combined four hundred items. CONJOINT FACTOR ANALYSIS OF EXTRAVERSION Conjoint factor analytic studies have been used for measures of more specific scales than personality inventories. They have proven themselves useful in the analysis of measures of extraversion although very few actually exist to date. Guilford and Guilford (1934) chose thirty - five items from current introversion - extraversion tests which they combined into one questionnaire. The results produced eighteen factors of which four were considered central: a) a tendency to fear the environment, b) an emotional sensitivity to the environment, c) impulsiveness, and d) interest in self. It was concluded that "the usual scale bearing the name [extraversion] does not refer to any real dimension of personality any more than the usual intelligence test measures a single real variable of mental ability" (Guilford &Guilford, 1934, p. 399). Finally, the study which most resembles the present one was reported in 1971 (Browne, 1971). Browne combined 400 items taken from twenty different item sources. An item factor analysis yielded twelve factors: sociability, adjustment - emotionality, social shyness, trust vs. suspicion, impulsivity, persistence, sex &superego, Freudian introversion, dominance, unidentified, cooperativeness - considerateness and finally, inferiority. This broad spectrum of factors led Browne to conclude that extraversion is too broad to be considered a unitary concept. THE PRESENT STUDY This leads us to the question, now, of whether tests which claim
- 60. to be measuring the same thing, such as extraversion, are actually measuring the same thing. It may be that two tests claiming to measure the exact same trait, for example, may not be measuring the same one, and this may be due to either a disparity between operational definitions or to inadequacies in the construction of the tests. The present study is focussed on these questions and has chosen to examine the concept of extraversion as reflected by various measures. METHOD Subjects The sample consisted of 210 introductory psychology students who completed their questionnaires in full. The sample was constructed of 109 females and 92 males(f.1). The age range of the 171 subjects who indicated their age was 19 to 52. The overall mean age was 22.4 (SD = 5.4). The average age for females was 23.2 (SD = 6.2) and for males 21.4 (SD = 3.9). Our sample is representative, in both age and gender composition, of those previously used in investigating the psychometric properties of the MBTI, EPQ, and HPQ. Psychometric Instruments A 98 - item questionnaire was developed as a measure of extraversion and was constructed from three measures of extraversion. These three scales were as follows: 1. The extraversion and introversion subscales of the Myers Briggs Type Indicator (MBTI) Form G. 2. The extraversion subscale of the Eysenck Personality Questionnaire (EPQ). 3. The five subscales of the Howarth Personality Questionnaire (HPQ) which comprise extraversion. The HPQ (Howarth, 1980) has been constructed from an item pool based on twenty personality factors of which ten traits are represented in the HPQ. For a more detailed history of the HPQ and subsequent research see Howarth &Zumbo (1988). The HPQ and EPQ were chosen because of
- 61. their popularity and because they were soundly constructed on the basis of factor analysis. The questionnaire was constructed by simply amalgamating the subscales beginning with the MBTI followed by the EPQ and the HPQ. There was no particular reason for this ordering. The item order of each subscale was unchanged from the order in which they originally appeared and instructions for each section were retained from the original. The MBTI extraversion subscale contains 21 items, the EPQ also contains 21 items and the HPQ contains 12 items for each subscale by which extraversion is defined: Sociability, Anxiety, Dominance, Impulsiveness and Inferiority (Howarth, 1985) for a total of 60 items from the HPQ. From these 102 items four were eliminated due to replication (EPQ #70 "Can you get a party going?", HPQ #21 "Do you like going out a lot?", #71 "I am a good social mixer" and #101 "I generally keep in the background on social occasions"). Scoring A. Item Scores. Each item of the questionnaire was scored according to the test manuals. A score of one was given to a response endorsing extraversion and zero elsewhere. This resulted in 98 dichotomously scored items. B. Scale Scores. To provide a score with which to validate the extraversion scales, we computed a scale score for each subject for each extraversion scale. This was accomplished by assigning a unit weight to each item which comprised the HPQ and EPQ scales. Therefore, the subjects received one point for each extraversion item they endorsed (i.e., answered in favour of extraversion). This procedure is identical to that given in the test manuals of the EPQ and HPQ.
- 62. It should be noted that for the EPQ and HPQ introversion is, in theory, lack of extraversion. That is, they are envisioned as two ends of a continuum. However, the MBTI differentiates between extraversion and introversion in that subjects receive scores for extraversion as well as for introversion. For the most part, extraversion items are identical to introversion items except that each item is weighted differently depending on whether the subject responds in favour of extraversion or introversion. The weighting for each item is given in the test manual. The scale scores for the MBTI were, therefore, formed in accordance with these weightings. When data analysis of extraversion scales was executed, those items which had been removed from any given scale due to replication elsewhere in the questionnaire were reinserted into their appropriate scale calculations so that all scales contained their complete set of items. Reliabilities Reports of the MBTI have generally yielded satisfactory reliabilities. Carskadon (1977) reported test - retest reliabilities on the extraversion/introversion scale as being .79 for males and .83 for females. The manual for the EPQ reports a test - retest reliability for the extraversion subscale as being high at .89 and being equally high for university students. The reliabilities for the five subscales of the HPQ range from .72 to .84 in value (Howarth, 1985). RESULTS The means, standard deviations and reliabilities were calculated for the items comprising each scale (see Table 1). These statistics were computed from the dichotomous data resulting from the item scoring. It is important to note that the two MBTI scales and the EPQ scale were each scored out of 21 and each of the HPQ scales, (Sociability (SOC), Anxiety (ANX), Dominance (DOM), Impulsiveness (IMP) and Inferiority (INF), were scored
- 63. out of 12. PART 1 Factorability of the Correlation Matrix Table 2 contains the correlation matrix of the eight scales. These eight scales were obtained via the scale scoring description given above. The Kaiser - Meyer Olkin (KMO) measure of sampling adequacy (Kaiser, 1970) was used yielding a value of .79 which is more than adequate. Bartlett's Sphericity test was used in order to determine whether the correlation matrix differed from the identity matrix. The test yielded a value of 1322.27, p <.001. Given the magnitude of the correlations these results were not surprising and allowed us to appropriately use the factor model. A maximum likelihood factor analysis followed by oblique rotation (Direct Quartimin, that is, Direct Oblimin with a delta value set at zero) was used for all factor solutions. A delta value of zero was chosen because when it is set at a large negative value the factor solutions are increasingly orthogonal, a value of zero allows for factors to be fairly highly correlated, while values approaching one produce factors that are highly correlated. We chose the moderate value zero. It should be noted, however, that even though there is a relation between the value of delta and the size of the correlation among the factors, the maximum value of the correlation among the factors for a given value of delta depends on the data. This is particularly why the Direct Quartimin was chosen, it allows the factors to be highly correlated (a solution very likely in a domain like extraversion) while not forcing a positive manifold (i.e., a one factor second - order solution; that is, something akin to a g - factor of extraversion) on the factor space. Furthermore, maximum
- 64. likelihood analysis allows for a statistical test of the goodness - of - fit between the data and the factor model while oblique rotation which is recommended by Hakstian (1971) and Hakstian &Abel (1974), does not constrain the resulting factors to being orthogonal and allows us to investigate any possible second - order factors. Various factor solutions were tested in which one - through to five - factor solutions were examined. Criteria used in determining the suitability of the model were twofold. The Chi - squared goodness - of - fit test and the residuals between the observed and the reproduced correlations each served to test how well the model fit the actual data. All of the residuals should be less than 0.10 in order for the solution to be appropriate for the data (McDonald, 1985). Neither the one - factor solution nor the two - factor solution met any of the criteria. The three - factor solution did not meet the criterion of the goodness - of - fit although the residuals were deemed adequate. A glance at the pattern matrix for the 3 - factor solution relayed reasonably high loadings of variables on factors except for the variable Dominance which had a low loading on all factors. It is the authors' opinion that the 3 - factor model is an under extraction. Without going into much detail, Factor 1 included MBTI - introversion, MBTI - extraversion, and Dominance. Factor 2 included Inferiority and Anxiety while Factor 3 included Sociability, EPQ, and Impulsiveness. The four - factor solution was decided upon as being most suitable. The goodness - of - fit test, x(Fe 2) (2) = 0.7463, p <.65, suggested an acceptable fit and all the residuals were acceptable at less than .10. Furthermore, all the communalities were less than 1.0 (see Table 2) which is an indicator of an adequate solution. The factors obtained were as follows: (see Table 3) Factor 1. This first factor was indeed responsible for a large portion of the total variance (46.0%) and was made
- 65. up of the MBTI scales. It makes theoretical sense for both MBTI scales to be in the same factor since, as we have seen, they are almost perfectly negatively correlated in the original correlation matrix. Factor 2. Howarth's Inferiority and Anxiety scales created this factor. Howarth's own definition describes extraversion as "lacking either anxiety or feelings of inferiority" (Howarth, 1985) and it would appear that a lacking in both of these is somehow related. Factor 2 accounted for 14.5% of the total variance. Factor 3. Sociability, EPQ extraversion and Impulsiveness formed the third factor which accounted for 6.6% of the total variance. Factor 4. The final factor responsible for only 4.2% of the total variance included only one variable, Dominance. In order to obtain a general idea of how the factors related to each other, let us now look at the factor correlation matrix. Table 4 indicates negative correlations between Factor 2 and all factors, which was expected considering Howarth's belief that his scales measure something which other extraversion scales lack. One cannot help noticing the large value (.787) which has resulted between Factor 1 (MBTI) and Factor 3 (SOC/EPQ/IMP). However, weaker correlations seemed to exist between Factors 4 and 1 and between Factors 4 and 3. Before proceeding, it should be noted that the results of this section were obtained from scale scores. These are the scores that an individual would obtain when scoring the measures according to their respective test manuals. This is important to note because there exists an alternative manner of analysing this data. That is, under statistically optimal conditions (i.e., given that we have 98 items we need well over 1500 subjects) the alternative approach would be to simultaneously fit all of the
- 66. scales via confirmatory factor analysis, then the resulting inter - factor correlation matrix would serve as the input for the exploratory factor analysis. However, the alternative analysis was not conducted for the following reasons: 1. In administering these scales in an applied setting factor score coefficients are not used. Rather, unit weights are utilized. We were interested in examining the construct validity of these scales within the context that they are being used. See Zumbo and Hubley (1993) for a discussion of the importance of considering the intended use of tests when investigating their validity. 2. The sample size in the present study is too small to allow for item - level analysis. This study was planned for scale - level analysis and therefore we planned for a factor analysis of eight variables. Furthermore, with the simultaneous fit method, our sample size would result in poor estimation of factor coefficients and factor scores. This would have a cascading disastrous effect on the joint distribution of the variables and the correlation coefficients among the factors (Tucker, 1971). Therefore, we have followed the recommendations of Bartlett (1937) and Overall and Klett (1983) to use unit weights rather than factor scoring coefficients(f.2) 3. It can be seen in the literature review that the item - level factorial validity of the EPQ, HPQ, and MBTI are well supported. In fact, these measures were chosen because of their psychometric properties. Another item - level analysis is not necessarily needed to substantiate the factorial validity of these measures. In summary, the simultaneous method was not utilized because of the issue of establishing validity within the context of test use, the inappropriate sample size, and that the
- 67. item - level factorial validity has been established in previous papers. Therefore, the four - factor solution based on the factor analysis of the scale scores can now be submitted to higher - order factor analysis. PART 2 Having extracted four factors from the data, the next step was to examine the structure of possible second - order factors. The four - factor correlation matrix achieved an adequate KMO - value of .61 and a significant value of 263.82, p <.05 on the Bartlett test of sphericity. These results allowed us to proceed with a higher - order factor analysis. The four - factor solution which was found to be appropriate in Part 1 of the results was subjected to a factor analysis in order to explore the possibility of extracting a single interpretable higher - order factor. Factor analysis proceeded as before, although rotation was not necessary for a one - factor solution. Using the same criteria as in Part 1, it was found that the Chi - squared goodness - of - fit was not statistically significant with X'Symbol not transcribed'2 (2)= 5.74, p >.05 with all residuals less than .10. The one - factor solution was, therefore, found to be appropriate. This second - order factor was labelled a general extraversion - introversion factor. The highest loading on this one general factor was Factor 1 with a value of .979 followed by factors 3, 4, and 2, with loadings of .804, .441, and -.273, respectively. This general extraversion - introversion factor is a coalescence of the MBTI extraversion/lack of introversion as well as Sociability, Impulsiveness and Eysenck's extraversion. Again, the small negative loading on Factor 2 lends credence to Howarth's statement that INF and ANX measure something that Eysenck's extraversion scale lacks. Out of curiosity the previously rejected three - factor solution was subjected to higher - order analysis. The criteria for the Kaiser - Meyer - Olkin and Bartlett tests were
- 68. met. The resulting three - factor matrix was similar to the four - factor matrix with Factor 1 (which now includes Dominance) loading almost perfectly followed by Factor 3 and Factor 2. The ordering of factors was similar to the above - mentioned solution and the factors themselves, described earlier, were almost identical in the content of their variables. Again, Factor 2 made up of Inferiority and Anxiety received a negative loading. This solution lends to the robustness of the unifactorial extraversion model. DISCUSSION In this paper we were interested in the construct validity of the MBTI subscales as a vehicle for exploring the potential unitary nature of extraversion. A conjoint factor analysis of certain extraversion scales seemed to be an interesting gateway to these issues. Though some studies have carried out item analyses of extraversion (Sipps &Alexander, 1987; Browne, 1971), the present study is unique to the authors' knowledge in its factor analytic calculations of extraversion at the scale level. What this means is that each measure of extraversion was represented in its entirety somewhere within the overall factor structure of the combined scales, as opposed to individual items being represented somewhere within the overall structure of the combined items. In other words, conjoint analysis at the scale level was more qualified to address the question of how each scale may differ from the other scales in terms of factor membership and the extent to which the factors are correlated. Conversely, analysis at the item level is limited to the question, "How well are each of the factors reproduced by the items?". So it is clear that conjoint scale analysis is better equipped to deal with our present concern which is that of discrepancies between scales
- 69. in what is being measured, i.e. factorial validity. See Howarth and Zumbo (1989; 1988) for further discussion. It seems that the MBTI scales formed a factor of their own and that the EPQ combined with Sociability and Impulsiveness to create the third factor. This comes as no surprise since the EPQ seems intuitively to define extraversion in terms of these two variables. The fact that the MBTI and the EPQ occurred as separate factors suggests that these two measures do not hold identical views on extraversion. However, as evidenced by the factor correlation matrix, Factor 1 (MBTI) and Factor 3 (SOC/EPQ/IMP) had a fairly high correlation. From this one could conclude that although each measure is unique, each contains a high degree of sociability and impulsiveness in its definition. The interfactor correlation among factors one and three was in support of Campbell &Heller (1987). The substantial correlation among factors one and three, and the factor loadings of the SOC, EPQ, and IMP suggested that the MBTI was primarily a sociability measure with a minimal association with impulsivity. This was also in support of Campbell &Heller. The second factor (INF/ANX) yielded only low negative correlations with the other factors and it seems therefore that although it took up 14.5% of the variance, it bears little relation to the other factors. Finally, Factor 4, Dominance, which was responsible for only 4.2% of the variance, obtained only a low loading on the MBTI factor in the three - factor solution and was relegated to its own factor in the final four - factor solution. From this first phase of the results it is clear that extraversion cannot be described as entirely unitary. It would appear to be defined in these measures by sociability, impulsiveness, a lack of inferiority and anxiety and the presence of dominance. Part 2 of the results made apparent the possibility of a single higher - order factor capable of bridging the gap between the original
- 70. four factors. The results did, in fact, indicate that these can be brought together into one interpretable, though less convincing higher - order factor. We may ask at this point whether the results were out of the ordinary and this question is difficult to answer since the study was unique in its approach. To the authors' knowledge, there have been no scale - level analyses of extraversion, though many item - level analyses exist. Such item analyses have revealed that extraversion is composed of many factors. For example, Sipps &Alexander (1987) reported finding three factors of extraversion which were sociability, impulsivity/non - planning and risk - taking / jocularity while Browne (1971) reported twelve. Certainly, it would be safe to say that sociability has never been far away from any set of results. Apart from being present in most factor analyses of extraversion, it has been shown that the extraversion scale of the MBTI is largely a measure of sociability (Sipps &DiCaudo, 1988). Given that the present study declared MBTI extraversion as the most salient factor, one must wonder about the strength of the relationship between extraversion and sociability. We would like to emphasize that factorial construct validity should be conducted not only at the item level whereby one establishes the reproducibility of the postulated scales but also at the scale level whereby several similarly labelled scales can be explored within a common factor space. We concur with Campbell &Reynolds (1984) in the following: In summary, we suggest that the most useful question to ask is not "Which is the real factor?" but rather "How do the available measures operate?" Researchers should continue to examine the utility of primary and higher - order traits... As a final caveat, researchers should not be misled by semantic similarity, either between models or across successive instruments for a given model; a dimension of
- 71. personality is best understood by its operating characteristics, not by its label (p. 319). One may wonder whether research in the area of extraversion is still necessary. Although the literature is less prevalent than in the past, the concept of extraversion has infiltrated personality measures and common language and remains an integral part of many personality inventories. As long as the term is still in use, research in this domain cannot be futile, nor can it be futile to examine and question the construct validity of representative scales. The authors believe there is a need for further scale level analyses as a process for expanding our knowledge of extraversion and its psychometric homologues. Thanks to Prof. Bob Stelmack of the University of Ottawa and three anonymous reviewers for comments on an earlier draft. Parts of this paper were reported by the second author for her B.A. Honours thesis at Carleton University under the supervision of BDZ. Send correspondence to: Bruno D. Zumbo, Measurement and Evaluation, Faculty of Education, University of Ottawa, Ottawa, Ontario CANADA K1N 6N5. E - mail: ZUMBO AT ACADJM1. UOTTAWA.CA. References Bartlett, M.S. (1937). The statistical conception of mental factors. British Journal of Psychology, 22, 97 - 104. Browne, J.A. (1971). Extraversion: In search of a personality dimension. Doctoral thesis, University of Alberta, 1971. Browne, J.A. &Howarth, E. (1977). A comprehensive factor analysis of personality questionnaire items. Multivariate Behavioural Research, 12, 399 - 427. Campbell, J.B. &Heller, J.F. (1987). Correlations of extraversion, impulsivity and sociability with sensation
- 72. seeking and MBTI - introversion. Personality and Individual Differences, 8, 133 - 136. Campbell, J.B. &Reynolds, J.H. (1984). A comparison of the Guilford and Eysenck Factors of Personality. Journal of Research in Personality, 18, 305 - 320. Carlson, J.G. (1985). Recent assessments of the Myers - Briggs Type Indicator. Journal of Personality Assessment, 49, 356 - 365. Carlyn, M. (1977). An assessment of the Myers - Briggs Type Indicator. Journal of Personality Assessment, 41, 461 - 473. Carskadon, T.G. (1977). Test - retest reliabilities of continuous scores on the Myers - Briggs Type Indicator. Psychological Reports, 41, 1011 - 1012. Eysenck, H.J. (1970). Historical Introduction. In H.J. Eysenck (Ed.), Readings in Extraversion - Introversion, Vol. 1, Theoretical and Methodological Issues. John Wiley &Sons: New York. Eysenck, H.J. &Eysenck, S.B.G. (1967). On the unitary nature of extraversion. Acta Psychologica, 26, 383 - 390. Eysenck, S.B.G. &Eysenck, H.J. (1963). On the dual nature of extraversion. British Journal of Social and Clinical Psychology, 2, 46 - 55. Farley, F. &Goh, D. (1976). PENmanship: Faking the P - E - N. British Journal of Social and Clinical Psychology, 15, 139 - 148. Furnham, A. &Henderson, M. (1982). The good, the bad and the mad: Response bias in self - report measures. Personality and Individual Differences, 3(3), 311 - 320. Guilford, J.P. (1977). Will the real factor of extraversion - introversion please stand up? A reply to Eysenck. Psychological Bulletin, 84, 412 - 416. Guilford, J.P. &Guilford, R.B. (1934). An analysis of the factors in a typical test of introversion - extraversion. Journal of Abnormal and Social Psychology, 28, 377 - 399. Hakstian, A.R. (1971). A comparative evaluation of several
- 73. prominent methods of oblique factor transformation. Psychometrika, 36, 175 - 193. Hakstian, A.R. &Abel, R.A. (1974). A further comparison of oblique factor transformation methods. Psychometrika, 39, 429 - 444. Howarth, E. (1980). Major factors of personality. Journal of Psychology, 104, 171 - 183. Howarth, E. (1985). Scale descriptions, norm tables and bibliography for the HPQ, APF and HMACL. Laboratory for Research in Personality, University of Alberta. Howarth, E. &Zumbo, B.D. (1989). An empirical investigation of Eysenck's typology. Journal of Research in Personality, 23, 343 - 353. Howarth, E. &Zumbo, B.D. (1988). Exploring new personality dimensions. Laboratory for Research in Personality, University of Alberta. Kaiser, H.F. (1970). A second generation Little Jiffy. Psychometrika, 35, 401 - 415. McDonald, R.P. (1985). Factor analysis and related methods. Hillsdale, N.J.: Lawrence Erlbaum. Overall, J.E., &Klett, C.J. (1983). Applied multivariate analysis. Malabar, Florida: Robert E. Kreiger Publishing Co.. Sells, S.B., Demaree, R.G., &Will, D.P. Jr. (1970). Dimensions of personality: A conjoint factor structure of Guilford and Cattell trait markers. Multivariate Behavioural Research, 5, 391 - 422. Sipps, G.J. and Alexander, R.A., (1987). The multifactorial nature of extraversion - introversion in the Myers - Briggs Type Indicator and Eysenck Personality Inventory. Educational and Psychological Measurement, 47, 543 - 552. Sipps, G.J. and DiCaudo, J., (1988). Convergent and discriminant validity of the Myers - Briggs Type Indicator as a measure of sociability and impulsivity. Educational and Psychological Measurement, 48, 445 - 451.
- 74. Stelmack, R.M. (1990). Biological Bases of Extraversion: Psychophysiological Evidence. Journal of Personality, 58, 293 - 311. Thompson, B., &Borrello, G.M. (1986). Construct validity of the Myers - Briggs Type Indicator. Educational and Psychological Measurement, 46, 745 - 752. Tucker, L.R. (1971). Relations of factor score estimates to their use. Psychometrika, 36, 427 - 436. Tzeng, O.C.S., Outcalt, D., Boyer, S.L., Ware, R., &Landis, D. (1984). Item validity of the Myers - Briggs Type Indicator. Journal of Personality Assessment, 48, 255 - 256. Zumbo, B.D., &Hubley, A.M. (1993). The role of validity theory in the resolution of observational indeterminacy. Carleton Papers in Applied Language Studies, 10, 18 - 37. Submitted June 28, 1991 Revision July 6, 1992 Accepted October 14, 1992 Footnote (f.1) To comply with ethical standards at our institution, subjects were given the option of submitting age and gender on the questionnaire. Nine subjects did not indicate their gender. (f.2) Although a simultaneous factor analysis of all items was not conducted, a scale - by - scale unifactorial solution was obtained. Factor scores were computed for each scale separately and these factor scores were used to create an 8 x 8 correlation matrix. The results of this analysis were a replication of the scale - level results in Table 4. We would like to thank a reviewer for this suggestion and prompting our consideration or this issue. TABLE 1 Mean Scores, Standard Deviations and Reliabilities for Each Scale ------------------------------------------------------------ Scale Mean Standard Reliability Deviation ------------------------------- ----------------------------- MBTI-Ext 13.90 6.30 .83 MBTI-Int 14.14 6.34 .83 EPQ 14.51 4.79 .86 SOC 8.36 3.34 .85