
Recommended
More Related Content
What's hot
What's hot (19)
Viewers also liked
Viewers also liked (12)
Similar to Ai morning report 1 21-2014
Similar to Ai morning report 1 21-2014 (20)
More from pkhohl
More from pkhohl (17)
Recently uploaded
Recently uploaded (20)
Ai morning report 1 21-2014
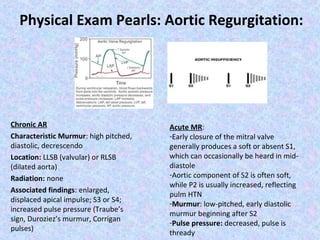
- 1. Physical Exam Pearls: Aortic Regurgitation: Chronic AR Characteristic Murmur: high pitched, diastolic, decrescendo Location: LLSB (valvular) or RLSB (dilated aorta) Radiation: none Associated findings: enlarged, displaced apical impulse; S3 or S4; increased pulse pressure (Traube’s sign, Duroziez’s murmur, Corrigan pulses) Acute MR: -Early closure of the mitral valve generally produces a soft or absent S1, which can occasionally be heard in middiastole -Aortic component of S2 is often soft, while P2 is usually increased, reflecting pulm HTN -Murmur: low-pitched, early diastolic murmur beginning after S2 -Pulse pressure: decreased, pulse is thready
- 2. Guidelines for Surgery in Native Valve Infective Endocarditis Deva Sharma, MD PGY3 1-21-2014
- 3. History: • Surgery was not an option for the management of IE until 1961, when Kay & colleagues excised fungal vegetations from the tricuspid valve of a patient • (Kay et al. N Engl J Med 1961; 264:907) • In 1965, an aortic valve was successfully replaced in a patient with IE 2/2 to Serratia marcescens • (Wallace et al. Circulation 1965; 31:450). • Over the last 3 decades, valve replacement & even repair have become more common in the management of select complications
- 4. ACC/AHA Guideline Summary: Surgery for Native Valve Endocarditis Class I: •Valve stenosis or regurgitation leading to heart failure. •AR or MR with hemodynamic evidence of elevated LVED or atrial pressures such as premature closure of the mitral valve with aortic regurgitation or moderate to severe pulmonary hypertension. •IE due to fungal or other highly resistant organisms. •Complications such as heart block, annular or aortic abscess, or destructive penetrating lesions such as fistula formation, mitral leaflet perforation with IE of the aortic valve, or infection in annulus fibrosis. Class IIa: •Recurrent emboli and persistent vegetations despite appropriate antibiotic therapy. Class IIb: •Mobile vegetations larger than 10 mm with or without emboli. J Am Coll Cardiol 2006; 48:e1.
- 5. European Society of Cardiology Guideline Summary: Surgery for Native Valve Endocarditis: Heart Failure (AR or MR): •Severe acute regurgitation or valve obstruction causing refractory pulmonary edema or cardiogenic shock (EMERGENT) •Fistula into a cardiac chamber or pericardium causing refractory pulmonary edema or shock (EMERGENT) •Severe acute regurgitation or valve obstruction and persisting heart failure or echocardiographic signs of poor hemodynamic tolerance (early mitral closure or pulmonary HTN) (URGENT) •Severe regurgitation and no heart failure (ELECTIVE) Habib et al. Eur Heart J 2009; 30:2369 Uncontrolled Infection: ALL URGENT •Locally uncontrolled infection (abscess, false aneurysm, fistula, enlarging veg) •Persisting fever and positive blood cultures >7 to 10 days •Infection caused by fungi or multiresistant organisms Prevention of Embolism: ALL URGENT •Large veg (>10 mm) following ≥ 1 embolic episodes despite appropriate abx tx •Large veg (>10 mm) & other predictors of complicated course (HF, persistent infection, abscess) •Very large vegetations (>15 mm)
- 6. Timing of Surgery: • In some cases, surgical intervention is delayed due to concerns about placing a prosthetic valve into actively infected tissue • On the other hand, early surgical intervention may be curative and life saving if it is done as early as the 1st or 2nd day of diagnosis in patients with acute valvular regurgitation and severe CHF. • Early surgery is recommended in patients with clear indications (ex, aortic regurgitation with heart failure, perivalvular extension or persistent infection, or high embolic risk), b/c prognosis is poor w/ medical therapy • • (Foghsgaard et al, Scand J Infect Dis 2008; 40:216) Although some studies show lower mortality rates with a longer duration of antibiotic therapy prior to surgery, these studies are affected by selection bias as patients who survive longer with medical therapy alone are at lower risk (Barsic et al, Clin Infect Dis 2013; 56:209)
- 7. Choice of Procedure: • When surgery is performed in the setting of active infection, the 2006 ACC/AHA guidelines recommended that valve repair is preferred to valve replacement • Valve repair may be particularly desirable in young IV drug users in whom compliance with AC required for mechanical prosthetic heart valves is often poor, & use of a bioprosthetic heart valve is associated with a high rate of structural deterioration over the long term.
- 8. Predictors of Poor Surgical Outcomes: • Five year survival rate for native valve endocarditis (aortic & mitral) is ~ 7579% • (Delay et al, Ann Thorac Surg 2000; 70:1219). • Predictors of operative morality: preoperative shock, perivalvular abscess, left ventricular ejection fraction <40%, & infection with Staphylococcus aureus (David et al, J Thorac Cardiovasc Surg 2007; 133:144) • Patients undergoing dialysis also have higher operative mortality, up to 25% • (Rankin et al, J Heart Valve Dis 2007; 16:617)
- 10. A 38 year-old man is admitted to the hospital for fever and SOB. He reports a 4 week history of malaise, recurrent fevers with chills, myalgia, and decreased appetite. On physical exam, temperature is 39.0°C (102.2°F), BP is 138/60 and pulse is 112. O2 saturation is 92% on ambient air. JVD is increased. The carotid upstrokes are brisk. There is an early systolic ejection click after S1 followed by a grade III/VI midpeaking systolic ejection murmur at the RUSB. S2 is normal but followed by a grade III/VI decrescendo diastolic murmur at the LLSB. An S3 and bibasilar crackles are heard. Lab findings include a Hgb of 9.0 and WBC count of 17.5 K with a left shift. He is empirically treated with vancomycin and gentamycin intravenously. Blood cultures are positive for viridans streptococci, susceptible to penicillin. TEE shows normal LV size and systolic function. The aortic valve is biscuspid with fusion of the right and left cusps. There is mild aortic stenosis. There is severe aortic valve regurgitation, with a leaflet perforation. An oscillating vegetation is found on the aortic valve, and echolucency (fluid) is seen around the aortic annulus posterior to this region. Which of the following is the most appropriate next step in management? (A)Add rifampin (B)Aortic valve replacement (C)Cardiac catheterization
- 11. Answer: B (aortic valve replacement) • In patients with endocarditis complicated by heart failure, abscess, severe regurgitation or hemodynamic derangements, valve replacement should be performed urgently, without delay for response to antibiotic therapy. • Addition of rifampin is not indicated in this patient with viridans streptoccocal endocarditis • Cardiac catheterization is not indicated in this patient and may increase the risk of embolization of vegetation or worsening hemodynamic status • Cardiac catheterization before planned cardiac surgery is indicated in patients with risk factors for coronary artery disease, which are not present in this patient.
- 12. A 55 year-old man is admitted to the hospital with a 3 week history of intermittent fevers and SOB. He has a mechanical aortic valve. He takes warfarin and no other medications. On physical exam, he has a temperature of 40.0°C (104.0°C), BP is 148/50, pulse is 93 and RR is 22. A grade II/VI early systolic murmur and early diastolic murmur are noted at the cardiac base. EKG shows sinus tachycardia with a new 1st degree AV block (prolonged PR interval). Blood cultures obtained on admission demonstrate grampositive cocci in clusters. Serum Cr level is 2.3. Which of the following is the most appropriate initial study to obtain? (A)Cardiac CT angiography (B)Cardiovascular magnetic response imaging (C)Transesophageal echocardiography (D)Transthoracic echocardiography
- 13. Answer: C (transeosphageal echocardiography) • TEE is the initial test of choice when there is a moderate or high pretest probability of endocarditis (ex- in patients with staphylococcal bacteremia or fungemia, a prosthetic heart valve or an intracardiac device) • TTE is ~ 32% sensitive overall in the diagnosis of infective enocarditis • Cardiac CT angiography & cardiovascular MR imaging may be helpful in identifying an aortic root abscess, but TEE is more likely to identify cardiac vegetations (also, the patient here has an elevated serum Cr)
- 14. References: KAY JH, BERNSTEIN S, FEINSTEIN D, BIDDLE M. Surgical cure of Candida albicans endocarditis with open-heart surgery. N Engl J Med 1961; 264:907. WALLACE AG, YOUNG WG Jr, OSTERHOUT S. TREATMENT OF ACUTE BACTERIAL ENDOCARDITIS BY VALVE EXCISION AND REPLACEMENT. Circulation 1965; 31:450. Vikram HR, Buenconsejo J, Hasbun R, Quagliarello VJ. Impact of valve surgery on 6-month mortality in adults with complicated, left-sided native valve endocarditis: a propensity analysis. JAMA 2003; 290:3207. Durack DT. Evaluating and optimizing outcomes of surgery for endocarditis. JAMA 2003; 290:3250. Aksoy O, Sexton DJ, Wang A, et al. Early surgery in patients with infective endocarditis: a propensity score analysis. Clin Infect Dis 2007; 44:364. Cabell CH, Abrutyn E, Fowler VG Jr, et al. Use of surgery in patients with native valve infective endocarditis: results from the International Collaboration on Endocarditis Merged Database. Am Heart J 2005; 150:1092. Tleyjeh IM, Ghomrawi HM, Steckelberg JM, et al. The impact of valve surgery on 6-month mortality in left-sided infective endocarditis. Circulation 2007; 115:1721.