1. Skin and Soft Tissue
Infections
Dr P Mahabeer
Dr. N. S. Naidoo
2. • What is the difference bet uncomplicated
and complicated ssti. Give 2 examples of
each and the bacterial causes.
• Write short notes on impetigo, bullous
impetigo, erysipelas, cellulitis.
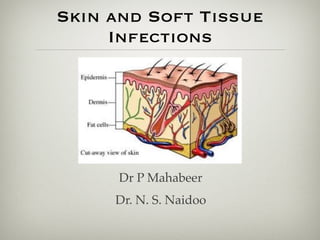
3. The Skin
• Skin :
– organ system with
multiple functions,
incl. protection of
tissues from external
microbial invasion
• Surface =
keratinised
stratified epithelium
4. Healthy Skin
• Intact skin – physical
barrier to penetration of
organisms
• Tight junctions bet
epithelial cells
• Acidic oily matrix prod by
sebaceous glands coats
epithelial cells
• Normal skin flora prevent
colonisation
5. How does infection occur?
• Minor trauma that destroys the integrity
and allows organisms access
• Surface penetrated by ducts of
pilosebaceous glands, sweat gland and hair
follicles provide route of entry for microbes
, esp. if ducts are obstructed
6.
Modes of infection
– Circulating microbe
– Circulating toxin
– Direct introduction of microbe into
epithelium
7. Pathogenesis
• To cause infxn – organisms must penetrate barrier
• Due to trauma
• Symptoms incude
– Pain
– Warmth
– Skin discolouration
– Swelling
– vesicles
8. Categories
– localised or spreading
– Uncomplicated – infxn of superficial layer
– Complicated – infxn extending to deeper
layers
9.
10. • Respond to drainage and antibiotics
• These include:
• Minor abscess
• Impetigo
• Cellulitis
• Erysipelas
• Folliculitis
• Furuncles or boils
• carbuncles
Uncomplicated
SSTI
11. complicated SSTI
– Involve deeper structures
– Significant surgical intervention
– Infxns in pts at risk eg Diabetes; poor blood supply
– These include
• Gas gangrene
• Necrotising cellulitis ( dermal and subcut tx)
• Necrotising fascitis ( include fascia)
• Pyomyositis and myonecrosis ( muscle)
16. • Spread to the dermis
and subcutaneous
tissue multiloculated
abscess
=CARBUNCLE
17. Impetigo
• Superficial infection of the
skin - becomes crusted
• Common in childhood,
poor hygiene,
overcrowding
• spread by sharing of
clothes or towels
• Aetiology
• Group A Streptococci
• S. aureus
18. Bullous impetigo
• Bullous form of impetigo
is caused by
S. aureus
• Newborns and young
children
• Vesicles ! rupture, leave
a moist red surface !
thin, brown crusts
19. Erysipelas
• Aetiology : S. pyogenes
• Rapidly spreading
infection of the deeper
layers of the dermis
• Assoc with pain and
redness
20. Cellulitis
• Acute spreading infection that
extends deeper to involve the
subcutaenous tissue
• Aetiology:
• S. pyogenes
• S. aureus
• Enteric gram negative bacilli
• Clostridia
• Anaerobes
24. Staphylococcus aureus
• Many children and adults become transiently
colonized by S. aureus.
• carried in the :
– Nasopharynx
– skin
– Clothing
– perineal area.
• intrapersonal transfer by aerosol and by direct
contact.
26. o Grow on blood agar
• golden colonies
• some strains show
ring of β-
haemolysis around
colonies
27. Pathogenesis
• Colonisation by Staph aureus mediated by:
– surface proteins – bind to host tissue
– Fibrin
– Collagen
– fibronectin
• Trauma , foreign matter – provide access
for org to enter
28. Virulence factors:
• Capsule
– Exopolysaccharide
– Prevents ingestion by PMN
– Promotes adherence to host cell and prosthetic devices
– Classified into 8 types based on immunotyping.
• Capsular types 5 and 8 resp for up to 75% of clin infections
• Vaccine ags 5 & 8 : pts with hemodialysis
29. Surface adhesins
• Adherence to host proteins
• Microbial surface components –
• acronym : MSCRAMM
• Imp ones are
• Clumping factor A and B
• Fibronectin-binding prts
• Prt A
30. • Protein A:
– Bound to cell wall peptidoglycan
– Binds Fc region of IgG
– Interferes with opsonisation, ingestion by PMN
• Cell wall constituents:
– Teichoic acid – imp for adherence to mucosal surfaces
– Peptidoglycan – rigidity & resilience
– Inhibit chemotaxis
31. • Teichoic acids rep 50% of wt of cell wall
• They are site of attach of prts and
enzymes
• LTA : plasma memb-bound counterparts
of teichoic acid – implicated in
inflammation – triggers cytokine release
32. • Enzymes:
– Catalase – inactivates H peroxide & free radicals prod after ingestion by PMN
– Coagulase – coat bact with fibrin →resistant to opson & phagocytosis
– Fibrinolysis – break down fibrin clots → spread in tissues
– Hyaluronidase – hydrolyses intracellular matrix of mucopolysacc in tissue →
spread
– Lipases – spread in subcut tissue
33. • Haemolysins:
– Alpha – lyses PMN , neurotoxin
– Beta – sphinogomyelinase – lyse varity of cells
• Panton Valentine Leucocidin (PVL):
– Found in 2% of strains
– Cause severe skin infections and severe haemorrhagic
pneumonia in young adults and children
– Encoded on a mobile phage
34. Staphylococcal scalded
skin syndrome
• SSSS (Ritter’s dx)
• Skin and mucosal colonisation with a toxigenic S aureus that prod an
exfoliative toxin (A or B)
• Toxin genes on plasmid or phage
• Toxin acts on desmoglein 1 ( transmemb desosomal glycoprotein invlv
in interkeratinocyte adhesion ) in the stratum granulosum
35. Staphylococcal Scalded
Skin Syndrome (SSSS)
• Infection with S. aureus
strains producing an
exfoliative exotoxin
• Characterized by
widespread bullae and
exfoliation
• Common in children,
especially newborns
36. • Superantigens
• Tsst-1
• Staph enterotoxin
• Are prts that do not activate the imm sys via
normal Ag presenting
• Attach to Vβ domain of large quan of T lymphs
• Activates 20%of total poolof T cells
• Normal Ag pres – 1/10000
• Massive cytokine release - shock
37. • Toxins:
– Exfoliatin/Epidermolytic toxins:
-resp for condition ‘Staph scalded skin syndrome ‘
-intercellular splitting of epidermis bet stratum spinosum and stratum
granulosum
Pyrogenic Toxin Superantigens:
-<10 % of strains prod PTSAgs
-Bind MHC II without processing
-Cause massive cytokine release
-Toxic shock syndrome toxin-1(TSST-1) and Enterotoxins
38. Staphylococcal toxic
shock syndrome(TSS)
• Toxin-mediated disease
• Pyrogenic exotoxin
• (1980’s – reported in hundreds of cases of
young women using intravaginal tampons)
39. Streptococcus Pyogenes
• Gram + cocci in chains
• Cxs
– sore-throat which can
lead to rheumatic
heart disease
– severe deep tissue
infections – ‘Flesh-
eating bacteria’
40. • Streps classified according
to hemolysis
– α , β ,non
• β streps - serogroups
based on CHO antigens
in CW:
– Lancefield Classification
( Group A,B,C )
• Strep pyogenes = Group A
strep =GAS
41.
Virulence factors:
• M protein –
– > 80 serotypes
– Maj virulence factor – anchored in cell memb
– Anti-phagocytic
– Lack of M-prt = non-pathogenic
• Protein F – bind to fibronectin
• LTA( lipoteichoic acid) – similar to Prt F
42. • Adherence to nasopharynx
– M protein
– Protein F
– LTA
• Adherence to skin
– M protein – keratinocytes
– Protein F – Langerhans cells
43.
Hemolysins:
–Streptolysin O:
• cytotoxin lysing WBC, Plts and tissue cells
• toxin inserts directly into the cell memb
forming pores
• antigenic and antibodies ags it used for
serological test ( ASOT)
–Streptolysin S:
– non-antigenic.
– toxic to WBC
44. • Pyrogenic exotoxins
– Erythrogenic toxin!scarlet fever(10%
GAS)
– Similar to pyrogenic toxins in St aureus
46. • 2 immunologic complications of GAS
infection:
– Acute rheumatic fever
• Antibodies to M protein bind to heart tissue- cross-
react
– Acute glomerulonephritis
• Deposition of immune complexes in glomerulus –
complement activation & inflammation
47. Wound infections
• Secondary to surgery, trauma or physiologic
• Contributing factors :
– Contaminating dose
– Virulence of org
– Physical condition of wound
– Physiological state of wound
• poor oxygenation
• poor blood supply
48. • Sources of infection
– Patient’s normal flora
– From infected people/carriers that may
reach the wound eg hands, fomites, air
– From environment eg soil, clothing
51. • produce the blue-
green pigment
pyocyanin.
• has a characteristic
fruity grape-like
odor.
52. • Epidemiology
• Found in soil, water
• Has been isolated from stool
• Hospitalised pts – higher colonisation rate
• Most impt cause of opportunistic infection
• Burns
• Cystic fibrosis
• Immunosuppression
54. • Toxins:
Exoenzyme S
Exotoxin A
• Lipopolysaccharide
Antiphagocytic surface properties
capsules, slime layers
LPS
Biofilm construction
55. Complicated SSTI
• Gas gangrene is a severe condition
resulting from bacteria invading healthy
muscle from adjacent traumatized muscle
or soft tissue.
• The infection originates in a wound
contaminated with bacteria of the genus
CLOSTRIDIUM.
56. • Clostridial myonecrosis is a destructive infectious
process of muscle associated with infections of the
skin and soft tissues.
• Caused by the anaerobic, gas-forming bacilli of
the Clostridium genus.
• Often occurs after
• abdominal operations on the GIT ,
• penetrating trauma, such as gunshot wounds
• frostbite,
can expose muscle, fascia, and subcutaneous tissues to
these organisms.
57. Clostridium spp.
• Large, spore forming GPB
• Spores resistant to heat, dessication and
disinfectant
• Medically impt:
• C. perfringens
• C. tetani
59.
C. perfringens
• Contamination of
wounds with org from
own intestinal flora or
spores from
environment
• Most common cause of
gas gangrene
o Culture
• Grows on BA
60. Clostridium perfringens
• This organism produces collagenases and
proteases that cause widespread tissue
destruction
• Multiple exotoxins
– Most important is α-toxin-phospolipase
that hydrolyses lecithin &
sphingomyelin! disrupt cell
membranes of various host cells
61.
C. tetani
• Contamination of wounds
• Can lead to tetanus in the unimmunised pt
• Effect by neurotoxin – tetanospasmin
• Blocks release of inhibitory
neurotransmitters
• Clinical:
• Severe muscle spasm – trismus (lockjaw)
62. Necrotising fascitis
• Severe infection involving the
subcutaneous soft tissues,
particularly the superficial and deep
fascia with muscle involvement
• Aetiology
• S. aureus
• Streptococci – Group A and Strep milleri
• Anaerobes
• Clostridia spp
• Vibrio vulnificus
• Aeromonas hydrophila
63. Infection of other skin
layers
• Infection of keratinised layers
• Fungal infections:
– Candida spp
– Dermatophytes
• Candida
• Moist areas
• Can be assoc with defects in cellular immunity
64. Dermatophyes:
• Human-human
transmission req close
contact
• minor lesions come in
contact with
dermatophyte hyphae
shed from another
infection.
• non-living, keratinised
tissues of nails, hair
and stratum corneum
of skin
65. • Low infectivity & virulence
• Not painful or life-threatening
• Families, locker rooms
• Aetiology -3 genera
• Microsporum
• Trichyophyton
• Epidermophyton
66. • Each “disease” often given its own name, eg.
Tinea capitis (scalp), tinea pedis (athletes foot)
• Most common – ringworm
• Treatment : topical antifungals (eg azoles)
67. Human bites
• can result in serious soft tissue infection.
• infections include
– Streptococcus spp
– S. aureus
– Eikenella corrodens
– Fusobacterium nucleatum
– Prevotella melaninogenica
68. Dog bites
• Infections related to dog bites are often
polymicrobial, predominantly involving
Pasteurella and Bacteroides spp.
69.
70. • A history of travel is important in the
assessment of SSTIs:
– Vibrio spp. infection in those exposed to
sea water
• Rashes in travellers may be associated with
a range of infections
– Tick bite fever