
Recommended
More Related Content
Similar to LEUKEMIA.pptx
Similar to LEUKEMIA.pptx (20)
Recently uploaded
Recently uploaded (20)
LEUKEMIA.pptx
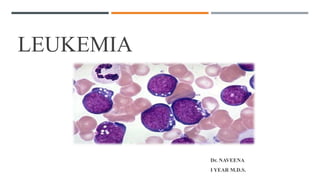
- 1. LEUKEMIA Dr. NAVEENA Ⅰ YEAR M.D.S.
- 2. 2 Leukaemia is a malignant disease of the hemopoietic tissue, characterized by the replacement of normal bone marrow elements with abnormal blood cells. INTRODUCTION DEFINITION
- 3. 3 • Leukemia was first described by anatomist and surgeon Alfred-Armand-Louis-Marie Velpeau in 1827 • John Hughes Bennett a pathologist gave leukemia its first published recognition as a clinical entity and as a blood-related disease • Pathologist Rudolf Virchow in 1845 reported a case and for the first time used the name “leukämie” (leukemia) • Pathologist Franz Ernst Christian Neumann found that the bone marrow of a deceased person with leukemia was colored " green-yellow" as opposed to the normal red. • By 1900, leukemia was viewed as a family of diseases as opposed to a single disease Thomas X. First contributors in the history of leukemia. World J Hematol 2013; 2(3): 62-70 [DOI: HISTORY
- 4. 4
- 5. 5 Blasts, which are immature and dysfunctional cells, normally make up 1% to 5% of marrow cells.
- 6. ETIOLOGY • Heredity – Downs syndrome • Ionizing radiation • Infections – HTLV 1 • Chemical carcinogens • Drugs • Immunodeficiency diseases 6
- 7. PATHOGENESIS • Genetic damage to a single clone of target cells • Chromosomal translocation • AML = t(15;17) • CML = t(9;22) • Maturation defect • Myelosuppression 7
- 8. MYELOID NEOPLASMS MYELOPROLIFERATIVE DISEASES MYELODISPLASTIC DISEASES MYELODISPLASTIC SYNDROMES ACUTE MYELOID LEUKAEMIA ACUTE BIPHENOTYPIC LEUKAEMIA 8
- 9. CHRONIC MYELOID LEUKEMIA (CML) DEFINITION CML is a myeloproliferative neoplasm characterized by the chromosomal translocation t(9;22) (q34.1;q11.2), resulting in the BCR-ABL1 fusion gene and formation of the Philadelphia chromosome (Ph*), which causes an increase in blood granulocytes and bone marrow myeloid precursors as the major proliferative component. ABL protein functions as a tyrosine kinase enzyme that in turn activates other kinases which inhibit apoptosis 9 Interphase fluorescence in situ hybridization (FISH), chromosome banding analysis, and PCR should be integrated for the diagnosis and follow-up of CML
- 10. CLINICAL FEATURES 20% of all leukemias Incidence: 3rd and 4th decade Juvenile CML –rare MANIFESTATIONS: Anemia Hypermetabolism Splenomegaly Bleeding tendencies Juvenile CML- skin rashes 10
- 11. 11 leucocytosis (20000/μl) ↑ myeloblast Basophilia BONE MARROW: Hypercellularity, ↑ myeloid-erythroid ratio HISTOPATHOLOGY
- 12. 12 TREATMENT: Imatinib oral therapy: It competitively inhibits ATP binding site of the ABL kinase, which in turn inhibits signal transduction BCR/ ABL fusion protein. It also induces apoptosis in BCR/ ABL positive cells Allogenic bone marrow transplantation Alpha interferon Chemotherapy
- 13. ACUTE MYELOID LEUKEMIA (AML) Acute myeloid leukemia (AML) is the most common leukemia among the adult population and accounts for about 80% of all cases. It is characterized by clonal expansion of immature “blast cells” in the peripheral blood and bone marrow resulting in ineffective erythropoiesis and bone marrow failure The most common risk factor for AML is myelodysplastic syndrome. 13
- 15. LABORATORY FINDINGS BLOOD PICTURE Anemia Thrombocytopenia ↑ Myeloblast - Auer rods (clumps of azurophilic granules resembling elongated needles) BONE MARROW EXAMINATION Hypercellular – dry tap on aspiration Leukemic cells > 20% blast cells in bone marrow Immunophenotyping – CD13 and CD33 antigen CYTOCHEMISTRY Romanowsky staining- type of leukemia Myeloperoxidase - + in immature myeloid cells Periodic acid Schiff - + in immature lymphoid cells BIOCHEMICAL INVESTIGATION ↑ Serum uric acid 15
- 16. 16 TREATMENT: Neutropenia – highly susceptible to infection prophylaxis against infections patients should be isolated and placed in laminar air flow rooms systemic antibiotics and leucocyte concentrate CYTOTOXIC DRUG THERAPY AIM: Induce remission and reduce hidden leukemic cell population COMBINATION DRUG THERAPY: Cytosine arabinoside, anthracyclines and 6-thioguanine BONE MARROW TRANSPLANTATION The basic principle is to reconstitute the patient’s hematopoietic system after total body irradiation and intensive chemotherapy The remission rate with AML is lower than in ALL. Medial survival with treatment- 12-18
- 17. LYMPHOID NEOPLASMS Hodgkin’s disease Precursor (Immature) B-cell malignancies – B cell acute lymphoblastic leukemia Peripheral (Mature) B-cell malignancies – chronic lymphocytic leukemia, hairy cell leukemia Precursor (Immature) T-cell malignancies - T cell acute lymphoblastic leukemia Peripheral (Mature) T-cell malignancies and NK cell malignancies 17
- 18. 18 PRECURSOR (IMMATURE) B- AND T-CELL LEUKEMIA ACUTE LYMPHOBLASTIC LEUKEMIA Most ALL cases occur in children, with an incidence of 3 to 4/100,000 in patients 0 to 14 years of age In children, ALLs represent 75% of all acute leukemias, with a peak incidence at 2 to 5 years of age A variety of genetic and environmental factors have been related to ALL. It occurs with increased frequency in patients with Down syndrome, Bloom syndrome, Neurofibromatosis type I Ataxia-telangiectasia
- 19. CLINICAL FEATURES Precursor B-cell lymphoblastic leukemia Extranodal site involvement is early Hepatomegaly, splenomegaly, CNS infiltration,infections due to cytopenia Precursor T-cell lymphoblastic leukemia Differentiate in the thymus Presents as a mediastinal mass and pleural effusion progresses rapidly to develop leukemia in the blood and bone marrow It is more aggressive than its B-cell counterpart. 19
- 20. 20 French-American-British classification for acute lymphoblastic leukemia FAB class Percent cases Morphology L1 Childhood ALL (B- ALL & T-ALL) More common in children Homogenous small lymphoblast; scanty cytoplasm, regular round nuclei, inconspicuous nucleoli L2 Adult ALL Mostly T-ALL More frequent in adults Heterogenous lymphoblasts; variable amount of cytoplasm, irregular cleft nuclei, large nucleoli L3 Burkitt type ALL (B-ALL) Uncommon Large Homogenous lymphoblast; cytoplasmic vacuolation , prominent round nuclei,
- 21. LABORATORY FINDINGS BLOOD PICTURE Anemia Thrombocytopenia ↑ lymphoblasts BONE MARROW EXAMINATION Malignant undifferentiated cells of precursor B or T cell origin CYTOCHEMISTRY Romanowsky staining- type of leukemia Acid phosphatase - + leukemic blasts Periodic acid Schiff - + in immature lymphoid cells 21 Romanowsky staining Giemsa staining
- 22. 22 TREATMENT: CHEMOTHERAPY COMBINATION DRUG THERAPY: vincristine, prednisolone, anthracyclines, cytosine arabinoside, and methotrexate patient with T cell ALL and those with meningeal involvement carry a less favorable prognosis BONE MARROW TRANSPLANTATION from a suitable allogenic or autologous donor is used in adults with relapses Prognosis and disease-free survival of children with ALL is better than in adults Medial survival children – 60 months, Adults- 12-18 months
- 23. 23 B-CELL LEUKAEMIA CHRONIC LYMPHOCYTIC LEUKAEMIA/SMALL LYMPHOCYTIC LEUKAEMIA Chronic lymphocytic leukemia (CLL) is a disease characterized by the relentless accumulation of CD5+ B lymphocytes in the peripheral blood, bone marrow, and secondary lymphoid organs (lymph nodes and spleen) CLL is the most common leukemia in adults, in the western countries, representing about 25–30% of all leukemias RISK FACTOR: Genetic and familial predisposition
- 24. CLINICAL FEATURES Asymptomatic Anemia Enlargement of superficial lymph nodes Splenomegaly, hepatomegaly and hemorrhagic manifestations Respiratory tract infection SAMPLE FOOTER TEXT 20XX 24
- 25. LABORATORY FINDINGS BLOOD PICTURE Anemia- 20% of cases develop coombs’ positive autoimmune hemolytic anemia Leucocytosis – mature small lymphoblasts BONE MARROW EXAMINATION Increased lymphocyte count(25-95%) Reduced erythroid and myeloid precursors LYMPHNODE BIOPSY Diffuse proliferation of well differentiated mature, small and uniform lymphocytes without any cytologic atypia or significant mitosis. 25
- 26. 26 TREATMENT: • Unlike other leukemias, none of the available drugs and radiation therapy are capable of eradicating CLL and inducing true complete remission • Treatment is palliative and symptomatic; these approaches include alkylating drugs, corticosteroids, and radiotherapy. Splenectomy is indicated in cases with autoimmune hemolytic anemia The prognosis of CLL is better than CML since blastic transformation seldom occurs
- 27. ORAL MANIFESTATIONS OF LEUKEMIA In acute leukemias, gingival hyperplasia is generally observed, mainly affecting the interdental papillae and the marginal gingiva caused by inflammation, or leukemic infiltration The infiltration of leukemic cells may also involve periapical tissues and simulate, both clinically and radiographically, periapical inflammatory lesions In chronic leukemia, the leukemic infiltrates in oral tissues is less frequent and can be observed: pallor of the mucosa, soft tissue infections, and generalized lymphadenopathy 27
- 28. DENTAL PROCEDURES IN DIFFERENT STAGES OF THE DISEASE AND TREATMENT Dental treatment should be planned according to the antineoplastic therapy Considering the risk of bleeding and serious infections associated with invasive procedures there are already some protocols that emphasize the importance of evaluating certain hematological indices, mainly neutrophils and platelets. 28 HIGH-RISK •Active leukemia •Pts under treatment •present bone marrow suppression MODERATE RISK •Completed the induction phase •The maintenance phase LOW- RISK •present no evidence of malignancy or myelosuppression.
- 29. DENTAL TREATMENT IN THE PRECHEMOTHERAPY PHASE Priority should be on eliminating sources of infection and trauma, as well as extractions and periodontal care. Endodontic treatment of symptomatic nonvital teeth should be done at least a week before the start of chemotherapy Extractions should be made, preferably three weeks prior to chemotherapy or radiotherapy and at least 10 to 14 days earlier. A neutrophil count of 1,500/mm3 and platelets of 40,000 cells/mm3 are required for performing periodontal probing or extractions. The procedures must be performed under antibiotic cover. when not possible, dental treatment should be postponed until the haematological indices increase. 29
- 30. DENTAL TREATMENT IN THE TRANSCHEMOTHERAPY PHASE Dental intervention is limited to emergency care The myelosuppression peak is most evident, usually after 14 days of drug administration, and at this time, dental treatment should be avoided; Before or 21 days after the start of chemotherapy the treatment can be performed platelet count of at least 60,000 cells/mm3 - for oral surgeries. When there is spontaneous bleeding resulting from minor trauma, measures Should be taken to control the bleeding MANAGEMENT OF BLEEDING Epinephrine – vasoconstrictor Topical thrombin - to stabilize blood clots Topical aminocaproic acid - to improve coagulation Topical use of tranexamic acid is also cited as an effective hemostatic in reducing postop bleeding 30
- 31. DENTAL TREATMENT AFTER CHEMOTHERAPY Patients who were cured of leukemia are considered to be of low risk and can be met with normal dental treatment regimens Antibiotic prophylaxis during oral procedures should be performed for at least six months after the completion of chemotherapy 31
- 32. CONCLUSION Performing dental procedures can offer a risk to the patient, depending on his state of health and phase of therapy. Noninvasive procedures can be performed at any stage of the disease or treatment. Invasive procedures offer higher risk. In emergency situations of risk considered, particularly those involving pain (acute cases), the patient should be assisted, if necessary, in a hospital setting, with the institution of measures to increase the hematological indices (transfusions) and, if applicable, with antibiotic coverage. 32
- 33. 33 • Textbook Of Pathology by Harsh Mohan 8th edition • Thomas X. First contributors in the history of leukemia. World J Hematol 2013; 2(3): 62-70 [DOI: 10.5315/wjh.v2.i3.62] • Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, Bloomfield CD, Cazzola M, Vardiman JW. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016 May 19;127(20):2391-405. [PubMed] • Zimmermann C, Meurer MI, Grando LJ, Gonzaga Del Moral JÂ, da Silva Rath IB, Schaefer Tavares S. Dental treatment in patients with leukemia. J Oncol. 2015;2015:571739. doi: 10.1155/2015/571739. Epub 2015 Feb 15. PMID: 25784937; PMCID: PMC4345074 • Chennamadhavuni A, Lyengar V, Shimanovsky A. Leukemia. [Updated 2022 May 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560490/ REFERENCES
- 34. 34
Editor's Notes
- All of the blood cells derive from pluripotential stem cells in the bone marrow thanks to a process called hematopoiesis. These cells differentiate into either Myeloid cells (the myeloid cell line). Myeloid cells differentiate into red blood cells, platelets, and the type of cells found in myeloid leukemia: neutrophils, monocytes, and more. Lymphoid cells differentiate into either B lymphocytes (B cells) or T lymphocytes (T cells), and lymphocytic leukemias may begin in either of these cell types.