Call Girls In Andheri East Call 9920874524 Book Hot And Sexy Girls
Antibiotic Therapy.pdf
1. Key Steps in Infection Management
1. ESTABLISH DIAGNOSIS & SEVERITY – follow guidelines and if unsure seek senior clinical advice from within your clinical team.
2. MICRO SAMPLING – Blood cultures (and other micro) before antibiotic. Don’t routinely swab skin/ wounds or culture urine in absence of signs of infection.
3. DOCUMENT INDICATION for antibiotic and proposed DURATION OF THERAPY (clinical notes & kardex) to avoid unnecessarily prolonged prescription.
4. PENICILLIN ALLERGY – Confirm nature with patient/ G.P. Often not true allergy – Vancomycin is inferior to Beta-lactam therapy in sensitive infections.
5. REVIEW & RECORD clinical response, micro results and prescription DAILY. Can you SIMPLIFY (narrow spectrum), SWITCH (IVOST) or STOP ANTIBIOTIC?
6. BEFORE CONTACTING INFECTION SPECIALIST: SENIOR CLINICAL REVIEW within your team, ensure adequate empirical prescription (≥48 hours and no
missed doses), check micro results (clinical portal/ Trakcare), source control – drain/ aspirate/ remove. Consider non-infective reasons for poor response.
Definition of SEPSIS:
INFECTION (includes system-related symptoms or signs and/ or features of the Systemic Inflammatory Response Syndrome (SIRS*)
WITH evidence of ORGAN HYPOPERFUSION (≥ 2 of: Confusion < 15 GCS or Resp Rate ≥ 22/ min or Systolic BP ≤ 100 mm Hg).
Ensure SEPSIS 6 within one hour: 1. Blood cultures (& any other relevant samples), 2. IV Antibiotic administration, 3. Oxygen to maintain target saturation,
4. Measure lactate, 5. IV fluids, 6. Monitor urine output hourly.
*SIRS indicated by Temp < 36°C or > 38°C, HR > 90 bpm, RR> 20/ min & WCC < 4 or > 12 x109/ L. SIRS is not specific to bacterial infection (also viral & non-infective causes).
Consider HIV Testing in all patients with infection and opportunistically in higher risk groups e.g. PWID/ IVDU, MSM, high endemic country of origin or travel.
NB The doses recommended below are based on normal renal/ liver function. See BNF for dose adjustments in renal/ liver impairment.
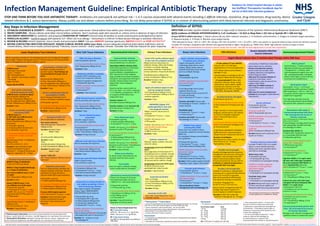
Infection Management Guideline: Empirical Antibiotic Therapy
STOP AND THINK BEFORE YOU GIVE ANTIBIOTIC THERAPY: Antibiotics are overused & not without risk – 1 in 5 courses associated with adverse events including C.difficile infection, resistance, drug interactions, drug toxicity, device
related infections & S. aureus bacteraemia. Always justify use and obtain cultures before prescribing. Do not delay prescription if SEPSIS or in context of deteriorating patient with likely bacterial infection and diagnostic uncertainty.
Guidance for initial hospital therapy in adults.
See StaffNet/ Therapeutics handbook App for
full list of NHS GGC infection guidance.
FURTHER ADVICE: Duty Microbiologist, Clinical/ Antimicrobial Pharmacist, Infectious Disease (ID) Unit at QEUH, local Respiratory Unit (for RTI) or from the Adult Therapeutic Handbook. Infection Control advice may be given by the Duty Microbiologist.
**Gentamicin/ **Vancomycin
• Access the Gentamicin & Vancomycin Adult Dosing Calculators via ‘Clinical
Info’ icon on the staff intranet page or the GGC Medicines App.
• Check creatinine/ renal function daily. Do not use eGFR.
• Record accurate times of dose administration and concentration
measurement on the prescription chart.
• Contact pharmacy if advice required.
Vancomycin
• If creatinine not available give the Vancomycin loading dose according to
actual body weight.
• Calculate the Vancomycin maintenance dose once creatinine is available.
Gentamicin
• If creatinine not available give gentamicin as follows:
Actual body weight Dose
< 40 kg 5 mg/kg
40 – 49 kg 240 mg
50 – 59 kg 280 mg
60 – 69 kg 320 mg
70 – 79 kg 360 mg
≥ 80 kg 400 mg
NB If CKD5 give 2.5 mg/kg (max 180 mg)
Doses in Renal Impairment for:
IV Temocillin dosing
eGFR 10 – 30 ml/min/1.73 m2 2g 24 hrly
eGFR 10 ml/min/1.73 m2 2g 48 hrly
IV Aztreonam dosing
See BNF for dosing advice according to
indication.
Non-severe community
acquired pneumonia (CAP)
CURB 65 score: ≤ 2 (and no sepsis)
Oral Amoxicillin 500mg 8 hrly
Or Oral ▲Doxycycline 200mg as a
one-off single dose then 100mg daily
Or Oral ■Clarithromycin 500mg 12 hrly
Duration 5 days
Severe community acquired
pneumonia (CAP)
CURB 65 score ≥ 3
or CAP (with any CURB 65 score)
PLUS sepsis syndrome:
IV/oral ■Clarithromycin 500mg 12 hrly
PLUS either:
IV Amoxicillin 1g 8 hrly
or if requiring HDU/ ICU level care
IV Co-amoxiclav 1.2g 8 hrly
or if true penicillin/beta-lactam allergy
or if legionella strongly suspected/
confirmed
Monotherapy IV/oral ▲■Levofloxacin
500mg 12 hrly
(NB oral bioavailability 99 – 100 %)
Duration 5 days (IV/oral) if rapid
clinical improvement by day 3
otherwise 7 – 10 days (IV/oral) as per
response. Legionella; 10 – 14 days.
Pneumonia
CURB 65 score:
•Confusion (new onset)
•Urea 7 mmol/L
•RR ≥ 30 breaths/ min
•BP – diastolic ≤ 60 mmHg or systolic
90 mmHg
•Age ≥ 65 years
Assess also for SEPSIS
Hospital acquired pneumonia
Within 4 days of admission
Treat as for CAP (see above)
Within 7 days hospital discharge
or ≥ 5 days of admission:
Non-severe CURB 65 score ≤ 2 and
no sepsis
Oral ▲Doxycycline 100mg 12 hrly
Duration 5 days
Severe CURB 65 score: ≥ 3 or
any CURB 65 score PLUS sepsis:
IV Amoxicillin 1g 8 hrly
+ IV Gentamicin**∆ (max 3 – 4 days)
If eGFR 20 ml/min/1.73 m2 REPLACE
Gentamicin with IV
Temocillin or
IV
Aztreonam.
or if true penicillin/beta-lactam allergy
Monotherapy IV/oral ▲■Levofloxacin
500mg 12 hrly
(NB oral bioavailability 99 – 100 %)
Duration 7 days (IV/oral)
Exacerbation of COPD/ LRTI
Antibiotics (usually oral) only if
purulent sputum. Dual therapy not
recommended increases risk of
harm.
Oral Amoxicillin 500mg 8 hrly
or Oral ▲Doxycycline 200mg as a
one-off single dose then 100mg daily
or Oral ■Clarithromycin 500mg 12 hrly
Duration 5 days
Severe/ complicated infective
exacerbation of COPD
Use IV therapy if indication for IV
route or ventilation required or sepsis.
IV Amoxicillin 1g 8 hrly
or if true penicillin/beta-lactam allergy
IV ■Clarithromycin 500mg 12 hrly
Duration 7 days (IV/oral)
Uncertain if LRTI/ UTI
Do not prescribe Co-amoxiclav.
Non-severe infection
Monotherapy Oral ▲Doxycycline
100mg 12 hrly
Duration Females 5 days
Males 7 days
Or
Oral Amoxicillin 500mg 8 hrly
Duration 5 days
PLUS
Oral Nitrofurantoin 50mg 6 hrly
or Oral Trimethoprim 200mg 12 hrly
Duration Females 5 days
Males 7 days
Severe ? LRTI/ UTI
See “Severe Systemic Infection Source
Unknown”
Aspiration pneumonia
This is a chemical injury and does not
indicate antibiotic treatment. Reserve
antibiotics for those who fail to
improve within 48 hrs post aspiration.
IVAmoxicillin 1g 8 hrly
+ IV Metronidazole 500mg 8 hrly
or if true penicillin/beta-lactam allergy
IV ■Clarithromycin 500mg 12 hrly
+ IV Metronidazole 500mg 8 hrly
If severe AND hospital acquired
ADD IV Gentamicin**∆ (max 3 – 4 days)
Duration 5 days (IV/oral) if rapid
clinical improvement by day 3
otherwise 7 days (IV/oral) as per
response.
Mild soft tissue infection
Oral Flucloxacillin 1g 6 hrly
or if true penicillin/beta-lactam allergy
Oral ▲Doxycycline 100mg 12 hrly
Duration 5 days
Mild infected human/ animal bite
Oral Co-amoxiclav 625 mg 8 hrly
or if true penicillin/beta-lactam allergy
Oral ▲Doxycycline 100mg 12 hrly
+ Oral Metronidazole 400mg 8 hrly
Duration 7 days
Severe infected human/
animal bite
Consider surgical review.
IV Co-amoxiclav 1.2g 8 hrly
or if true penicillin/beta-lactam allergy
IV Vancomycin**
+ Oral Metronidazole 400mg 8 hrly
+ Oral ▲■Ciprofloxacin 500mg 12 hrly
Duration 10 days (IV/oral)
Moderate cellulitis/ erysipelas
Consider OPAT/ ambulatory care
(consult local management pathway).
If requires inpatient management:
IV Flucloxacillin 2g 6 hrly
If MRSA suspected or if true penicillin/
beta-lactam allergy
IV Vancomycin**
Duration 7 days (IV/oral)
Mild peri-anal soft tissue infection
Oral Co-amoxiclav 625 mg 8 hrly
or if true penicillin/beta-lactam allergy
Oral ▲Doxycycline 100mg 12 hrly
+ Oral Metronidazole 400mg 8 hrly
Duration 7 days
Severe peri-anal soft tissue infection
Urgent surgical review.
IV Co-amoxiclav 1.2g 8 hrly
or if true penicillin/beta-lactam allergy
IV Clindamycin 600mg 6 hrly
+ IV Gentamicin**∆ (max 3 – 4 days)
+ Oral Metronidazole 400mg 8 hrly
Duration 10 days (IV/oral)
Suspected necrotising fasciitis or
any rapidly spreading or life or
limb threatening infection
Seek urgent surgical/ orthopaedic
review. Urgent DEBRIDEMENT/
EXPLORATION may be required.
IV Flucloxacillin 2g 4 hrly
+ IV Benzylpenicillin 2.4g 6 hrly
+ IV Metronidazole 500mg 8 hrly
+ IV Clindamycin 600mg 6 hrly
+ IV Gentamicin**∆ (max 3 – 4 days)
If MRSA suspected or if true penicillin/
beta-lactam allergy
Treat as above but REPLACE Flucloxacillin
+ Benzylpenicillin with IV Vancomycin**
Duration 10 – 14 days or as per
microbiology/ ID
Gastroenteritis infection
Antibiotics not usually required and
may be deleterious in E.coli 0157.
Clostridium difficile infection (CDI)
Treat before laboratory confirmation
if suspected (loose stools plus
recent antibiotics, hospitalisation or
PPI). Discontinue if toxin negative.
Stop/ simplify concomitant antibiotics
and gastric acid suppressive therapy if
possible. Review opiates and avoid
loperamide. Ensure adequate
hydration.
Severity markers; severe colitis on
CT/ X-ray, WCC 15 x 109/L, creatinine
1.5 x baseline, temperature 38.5°C
or suspicion of PM colitis/ toxic
megacolon/ ileus.
Severity markers = 0
Oral Metronidazole 400mg 8 hrly
Severity markers ≥ 1 or recurrent CDI
Oral Vancomycin 125mg 6 hrly
Duration 10 days
Lower UTI/ cystitis without sepsis
in men and non-pregnant women
Obtain urine for culture prior to
antibiotic therapy. Often self-limiting
in women so consider delaying
prescribing. Antibiotics if significant
urinary symptoms, frequency dysuria.
Oral Nitrofurantoin 50mg 6 hrly
or Oral Trimethoprim 200mg 12 hrly
Duration Females 3 days
Males 7 days
Upper UTI without sepsis in men
and non-pregnant women
Oral▲■Ciprofloxacin 500mg 12 hrly
or Oral Trimethoprim 200mg 12 hrly if
sensitive organism.
Duration 7 days
UROSEPSIS (Upper UTI/
pyelonephritis) in men and
non-pregnant women
Obtain urine for culture prior to
antibiotic.
IV Gentamicin**∆ (max 3 – 4 days)
If eGFR 20 ml/min/1.73 m2
IV
Temocillin
If eGFR 20 ml/min/1.73 m2 AND true
penicillin/beta-lactam allergy
Oral ▲■Ciprofloxacin
See BNF for dosing in renal impairment
Duration 7 days
Catheter related UTI
Remove/ replace catheter and send
urine for culture.
Symptomatic bacteriuria WITHOUT
sepsis
Give single dose of IV Gentamicin**∆
immediately prior to catheter removal
or if IV route not available give single
dose of oral ▲■Ciprofloxacin 500mg
30 minutes before catheter change.
Symptomatic bacteriuria WITH sepsis
As above and treat as per
pyelonephritis/ culture results.
Duration 7 days (IV/oral)
Septic arthritis/ Osteomyelitis/
Prosthetic joint infection
Urgent orthopaedic referral if
underlying metal work or recent
surgery. Obtain blood cultures,
synovial fluid/ deep tissue sample
prior to antibiotic therapy.
Native joint
IV Flucloxacillin 2g 6 hrly
If MRSA suspected or if true penicillin/
beta-lactam allergy
IV Vancomycin**
If considered high risk for Gram
negative infection e.g.
immunocompromised, recurrent UTI
or sickle cell disease
ADD IV Gentamicin**∆ (max 3 – 4 days)
Duration and IVOST: discuss with
microbiology at 72 hours. Usually 4 – 6
weeks (IV/oral).
Prosthetic joint
IV Gentamicin**∆ (max 3 – 4 days)
+ IV Vancomycin**
Duration and IVOST: discuss with
microbiology at 72 hours.
Diabetic foot sepsis/
osteomyelitis (OM)
Assess ulcer size, probes to bone,
neuropathy, peripheral vascular disease,
MRSA risk.
For outpatient therapy consult diabetic
clinic guidelines.
IV Flucloxacillin 2g 6 hrly
+ IV Gentamicin**∆ (max 3 – 4 days)
+ Oral Metronidazole 400mg 8 hrly
If MRSA suspected or if true penicillin/
beta-lactam allergy
IV Vancomycin**
IV Gentamicin**∆ (max 3 – 4 days)
+ Oral Metronidazole 400mg 8 hrly
Duration If OM usually 6 weeks (IV/oral)
Dependent upon surgical intervention
Vascular graft infection
IV Flucloxacillin 2g 6hrly
+ IV Gentamicin **∆ (max 3 – 4 days)
If MRSA suspected or if true penicillin/
beta-lactam allergy
IV Vancomycin**
+ IV Gentamicin**∆ (max 3 – 4 days)
Discuss duration/ further
management with microbiology/ ID
Intra-abdominal sepsis
IV Amoxicillin 1g 8 hrly
+ IV Metronidazole 500mg 8hrly
+ IV Gentamicin**∆ (max 3 – 4 days)
If eGFR 20 ml/min/1.73 m2 REPLACE
Gentamicin with IV
Temocillin
or if true penicillin/beta-lactam allergy
IV Vancomycin**
+ IV Metronidazole 500mg 8 hrly
+ IV Gentamicin**∆ (max 3 – 4 days)
If eGFR 20 ml/min/1.73 m2 REPLACE
Gentamicin with IV/oral ▲■Ciprofloxacin.
See BNF for dosing in renal impairment
Duration 7 days (IV/Oral)
Biliary tract infection
As above except metronidazole not
routinely required unless severe
infection.
Pancreatitis
Does not require antibiotic therapy
unless complicated by cholangitis.
Spontaneous bacterial peritonitis
Chronic liver disease PLUS ascites
PLUS peritoneal white cell count
500/mm3 or 250 neutrophils/mm3
IV Amoxicillin 1g 8 hrly
+ IV
Temocillin 2g 12 hrly
or if true penicillin/beta-lactam allergy
▲■Ciprofloxacin IV 400mg 12 hrly
or Oral 500mg 12 hrly
+ IV Vancomycin**
Duration 7 days (IV/oral) but
dependent on clinical review
LP safe without CT scan UNLESS:
seizures, GCS ≤ 12, CNS signs,
papilloedema or immunosuppression.
If CT: Blood cultures and antibiotics
BEFORE CT scan.
Use Meningitis/ Encephalitis order set
on Trakcare, Blood and CSF Glucose.
LP contraindicated if: Brain shift,
rapid GCS reduction, Resp/ cardiac
compromise, severe sepsis, rapidly
evolving rash, infection at LP site,
coagulopathy (incl INR ≥ 4, Platelets
40, DOAC, therapeutic LMWH).
Possible bacterial meningitis
IV Ceftriaxone 2g 12 hrly
or if true penicillin/beta-lactam allergy
IV Chloramphenicol 25mg/kg (max 2g)
6 hrly
If age ≥ 60 years, immunosuppressed,
pregnant, alcohol excess, liver disease
or if listeria meningitis suspected:
ADD IV Amoxicillin 2g 4 hrly to
Ceftriaxone
or if true penicillin/beta-lactam allergy
ADD IV Co-trimoxazole 30mg/kg 6 hrly
to Chloramphenicol
IF BACTERIAL MENINGITIS STRONGLY
SUSPECTED ADD IV Dexamethasone
10mg 6 hrly (for 4 days) and refer to ID
Duration of antibiotics:
Meningococcal; 5 days, Listeria; 21 days,
Pneumococcal; 10 – 14 days,
Haemophilus; 10 days
Possible viral meningitis
Usually only diagnosed after empirical
management and exclusion of bacterial
meningitis. Viral meningitis does NOT
require antiviral prescription unless
immunocompromised. Discuss with ID.
Confusion or reduced consciousness =
Encephalitis NOT meningitis
Possible viral encephalitis
Consider if confusion or reduced level
consciousness in suspected CNS infection.
Ensure CSF viral PCR is requested.
May not be possible to differentiate
from bacterial meningo-encephalitis.
IV Aciclovir 10mg/kg 8 hrly
See BNF for dosing in renal impairment.
Discuss further management with ID/
virology. May require repeat LP or
neuro-imaging to establish diagnosis.
Duration If HSV/ VZV confirmed
continue IV therapy for 14 – 21 days
Community or Healthcare associated
sepsis where source unknown.
Review all anatomical systems,
perform CXR and consider other
imaging/ laboratory investigations.
Review diagnosis DAILY.
Add cover for S.aureus infection if;
healthcare associated, recent
hospitalisation, post-op wound/ line
related, IVDU/ PWID.
Add cover for MRSA infection if;
recent MRSA carrier or previous
infection.
Add cover for severe Streptococcal
infection if; pharyngitis/ erythroderma/
hypotension.
Source unknown
IV Amoxicillin 2g 6 hrly
+ IV Gentamicin**∆ (max 3 – 4 days)
If S.aureus suspected
ADD IV Flucloxacillin 2g 6 hrly
If MRSA suspected or if true penicillin/
beta-lactam allergy
IV Vancomycin**
+ IV Gentamicin**∆ (max 3 – 4 days)
If severe Streptococcal infection
suspected
ADD IV Clindamycin 600mg 6 hrly
Duration Review with response/ micro
results at 72 hours.
Possible Infective Endocarditis
Consider if PWID/ IVDU, line related
sepsis or recent dental extraction.
Always seek senior specialist advice
and refer to cardiology.
Native heart valve
IV Amoxicillin 2g 4 hrly
+ IV Flucloxacillin 2g 4 hrly
+ IV Gentamicin ∆ (#synergistic dosing)
If MRSA or resistant organisms
suspected or if true penicillin/
beta-lactam allergy
IV Vancomycin**
+ IV Gentamicin ∆ (#synergistic dosing)
Prosthetic heart valve
IV Vancomycin**
+ IV Gentamicin ∆ (#synergistic dosing)
Duration Review with micro results at
72 hours and discuss addition of
Rifampicin (NB many drug interactions)
Which patient?
Chemotherapy 3 weeks previously,
high dose steroids (e.g. prednisolone
15mg/day for 2 weeks), other
immunosuppressive agents (e.g. anti-
TNF, cyclophosphamide), transplant
patient (solid organ or bone marrow)
or primary immunodeficiency.
Neutropenic Sepsis
Neutrophils 0.5 or 1.0 if recent
chemotherapy within previous 3 weeks
AND temperature 38°C or 36°C on
2 occasions 30 mins apart or if clinically
unwell even if apyrexial.
If on high dose steroids/ severely
immunocompromised may be afebrile
but present with symptoms of sepsis.
Neutropenic with sepsis or
Immunocompromised with fever,
NO neutropenia and source of
infection unknown
(See Initial Management of Neutropenic Sepsis in
Adults poster for details)
If haematology/ oncology patient discuss
with appropriate specialist and seek
microbiology/ ID advice.
Standard Risk: NEWS ≤ 6
IV Piperacillin/ Tazobactam 4.5g 6 hrly
or if unavailable REPLACE with
IV Ceftazdime 2g 8 hrly
or if history of penicillin/beta-lactam
allergy (NOT anaphylaxis)
IV
Aztreonam 2g 6 hrly
+ IV Vancomycin**
or if beta-lactam anaphylaxis
IV Gentamicin**∆ (max 3 – 4 days)
+ IV Vancomycin**
High Risk: NEWS ≥ 7 or septic shock
OR stem cell/ solid organ transplant
OR acute leukaemia AND NEWS ≤ 6:
As for Standard Risk above but
ADD IV Gentamicin**∆ (max 3 – 4 days)
or if beta-lactam anaphylaxis
IV Gentamicin**∆ (max 3 – 4 days)
+ IV Vancomycin**
+ IV ▲■Ciprofloxacin 400mg 12 hrly
Critical risk: stem cell/ solid organ
transplant OR acute leukaemia AND
NEWS ≥ 7 or septic shock:
IV Meropenem 2g 8 hrly
+ IV Amikacin (See Adult Therapeutics
Handbook for dosing)
or if true penicillin/beta-lactam allergy
IV Amikacin (See Adult Therapeutics
Handbook for dosing)
+ IV ▲■Ciprofloxacin 400mg 12 hrly
+ IV Vancomycin**
Immunocompromised patient with
fever, NO neutropenia but source
of infection identified
Manage as per infection management
guidelines based on anatomical source.
Lower Respiratory Tract Infections Skin/ Soft Tissue Infections Gastrointestinal Infections Urinary Tract Infections Bone/ Joint Infections CNS Infections
Severe Systemic Infection
Source Unknown
Immunocompromised Patient
Urgent Blood Cultures then IV Antimicrobial Therapy within ONE hour
• Take a Gentamicin level 6 – 14 hours after
the start of the first infusion review dose.
• Ototoxicity is associated with prolonged use
of Gentamicin. If the patient reports signs or
symptoms of ototoxicity STOP Gentamicin and
contact Microbiology/ ID.
• Do not use Gentamicin beyond 3 – 4 days
unless on advice of Microbiology/ ID.
∆ Avoid Gentamicin in patients with
decompensated liver disease or myasthenia gravis.
Suspected prostatitis
Refer to urology
Oral ▲■Ciprofloxacin 500mg 12 hrly
or Oral Trimethoprim 200mg 12 hrly
if sensitive organism.
Duration 28 days
■Clarithromycin/ Quinolone: risk of serious drug interactions may prolong the QTc
interval. Avoid if other QTc risk factors. See BNF (appendix 1) or seek advice from pharmacy.
▲Doxycycline/ Quinolone: absorption reduced with oral iron, calcium, magnesium and
some nutritional supplements. See BNF (appendix 1) or seek advice from pharmacy.
NHS GGC Antimicrobial Utilisation Committee; Aug 2017. Expires Aug 2020. Updates: www.ggcformulary.scot.nhs.uk/Guidelines
#See Synergistic Gentamicin for Endocarditis
in Adults guideline on StaffNet for dosing.
Obtain respiratory samples for microbiology (sputum) and virology (throat gargle)
and consider influenza during peak season. If clinical suspicion of influenza please
refer to HPS guidelines for latest treatment options.
Uncertain if UTI/ LRTI
See under ‘Lower Respiratory Tract
Infection’ section.