Deep vein thrombosis
•Download as PPTX, PDF•
8 likes•660 views

Deep vein thrombosis is a blood clot that forms within the deep veins, usually in the legs. Ultrasound is the primary imaging tool used to diagnose DVT and distinguish between acute, subacute, and chronic clots based on characteristics like echogenicity, size, and adherence to vein walls. Doppler ultrasound can further evaluate venous blood flow and identify areas of obstruction. While ultrasound is very accurate, other modalities like CT, MRV, and conventional venography may be used in specific cases to identify clots in other veins or rule out other causes.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Deep vein thrombosis
Similar to Deep vein thrombosis (20)
Recently uploaded
Recently uploaded (20)
Deep vein thrombosis
- 2. Definition Deep vein thrombosis is a condition by which blood changes from liquid to solid state and produces a blood clot (thrombus) within the deep venous system typically in the lower limbs
- 3. Grayscale Ultrasound Acute thrombosis (- 14 days) • Low echogenicity • Venous distension: Recently larger than accompanying artery • Loss of compressibility: • Free floating thrombus: • Collateralization: Tortuous and braided collateral veins, usually smaller than the normal vein Subacute thrombosis (- 2 weeks to 6 months) • more echogenic, variable • Decrease thrombus and vein sizel • Adherence of thrombus: Free floating thrombus becomes attached to vein wall • Resumption of flow: Luminal flow may be restored; but vein may remain occluded • Collateralization: Collateral continues to develop Chronicphase (~ 6 months) • Post-thrombotic scarring: Thrombus becoming organized as fibrous tissue • Wall thickening: with reduced luminal diameter • Echogenic intraluminal material: may occasionally calcify • Synechiae: Formed from un lysed thrombus that is attached to one side of the vein wall and gradually transformed into a fibrous band • Fibrous cord: In veins which fail to recanalize, • Valve abnormalities: thickening of valve cusps and restricted cusp motion may result leading to reflux and venous stasis
- 4. Pulsed Doppler o Spontaneous flow (any waveform present) • Expected in medium to large veins, but flow is often not spontaneous in smaller calf veins o Phasic flow (variation in flow velocity with respiration) • When phasic pattern is absent, flow is described as continuous, indicating the presence of obstruction closer to the heart o Valsalva maneuver • Causes abrupt cessation of blood flow in large and medium size veins documenting patency of venous system from point of examination to thorax o Augmentation (increase in flow velocity with distal compression) • Absence of this response indicates presence of obstruction further away from the heart to the site of examination
- 5. Color Doppler - Useful to detect low echo or anechoic thrombus which may be missed on grayscale US - Demonstration of recanalized lumen in the thrombus and collateralization - Demonstration of reflux in valvular incompetence • Power Doppler: Particularly useful in the demonstration of slow flow through recanalized lumen and collaterals
- 6. Imaging Recommendations • Best imaging tool o Duplex Doppler ultrasound is first line imaging investigation with sensitivity and specificity for acute symptomatic DVT between 90-100% o CECT and MR/MR venography are good non-invasive imaging tools for assessment of pelvic veins and IVC and for exclusion of pelvic and abdominal causes of DVT o Conventional venography has a false negative rate of 11% and should be reserved for use as problem solving aid
- 7. DIFFERENTIAL DIAGNOSIS Interpretation Errors • Baker cyst, artifactual "echocontrast" from slow flow, thickened valve mistaken for thrombus in chronic venous obstruction, failure to identify duplicated vein Technical Errors • Inadequate compression, improper use of color flow image, poor venous distension, misidentification of deep vs. superficial veins
- 8. CLINICAL ISSUES • Most common signs/symptoms o Acute DVT: Swollen and tender lower limb (extent of swelling depends on site of DVT), increased temperature o Post thrombotic syndrome: Sequelae of DVT resulting from chronic venous obstruction and/or acquired incompetence of valves o Chronic leg swelling, ankle pigmentation, and ulceration in the lower calf and ankle (gaiter zone) • Other signs/symptoms: Signs and symptoms from pulmonary embolism: Shortness of breath, pleuritic chest pain, tachycardia, hypoxia, hypotension
- 9. Image Interpretation Pearls • Thrombus is excluded if the vein is completely compressed
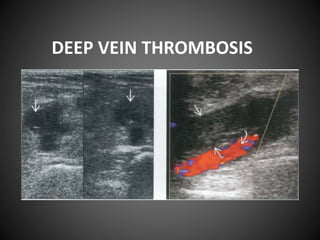
- 10. Transverse ultrasound shows acute DVT of the popliteal vein, filled with hypoechoic thrombus (right) and incompressible with transducer pressure (left).
- 11. Corresponding longitudinal color doppler ultrasound shows vein with absent intraluminal color signal while the artery posterior to it demonstrates complete color filling.
- 12. Transverse ultrasound shows thrombosis of the common femoral vein (CFV) The vessel is non-compressible (right side of image).
- 13. Corresponding longitudinal color Doppler ultrasound shows DVT of CFV with partial color filling.
- 14. Longitudinal color Doppler ultrasound shows acute thrombosis of the superficial femoral vein (SFV)
- 15. Longitudinal color Doppler ultrasound shows acute thrombosis of the popliteal vein
- 16. Longitudinal color Doppler ultrasound shows thrombosis of one of the posterior tibial veins (PTV)
- 17. Longitudinal color Doppler ultrasound shows a normal posterior tibial artery accompanied by a pair of normal,patent, posterior tibial veins . Note that calf veins are usually paired.
- 18. Longitudinal color Doppler ultrasound shows acute thrombosis of the peroneal veins. Note paired thrombosed peroneal veins are accompanied by small peroneal artery .
- 19. Transverse ultrasound shows chronic DVT of the SFV. The thrombosed vein is contracted and filled with echogenic thrombus.
- 20. Longitudinal ultrasound shows a soleal vein thrombosis with intraluminal incompressible, hypoechoic thrombus. Note sluggish flow in the soleal vein may mimic venous thrombosis.
- 21. Longitudinal color Doppler ultrasound shows chronic DVT with partial recanalization of thrombus
- 22. Transverse ultrasound shows chronic DVT with a contracted thrombus.
- 23. Longitudinal ultrasound shows chronic DVT within the CFV. Note the thrombosed vein contains multiple calcifications with acoustic shadowing.
- 24. Longitudinal pulsed Doppler ultrasound shows the normal variation in Phasic flow in the SFV Note phasic variation is absent and becomes continuous if an obstructing lesion is present between the site of examination and heart.
- 25. Longitudinal pulsed Doppler ultrasound shows normal augmentation in the SFV when the calf is compressed. This indicates there are no obstructing lesions between the site of examination and calf
- 26. MR venogram of the common femoral veins external iliac veins common iliac veins and inferior vena cava. Contrast was injected simultaneously via pedal veins in both feet.
- 27. MRV shows obstruction to flow of contrast at the origin of the left external iliac vein (f/V) =indicating thrombosis of the left f/V
- 28. Oblique CECT shows Non enhancing thrombus within the infra renallVC. Distance between the left renal vein BI and the top of the IVC thrombus was measured (26.3 mm) for assessment of suitability for IVC filter deployment.
- 29. IVC cavogram with pigtail catheter positioned above the common iliac vein confluence. An IVC filter is seen within the Infrarenal lVC with thrombus (filling defects) trapped within it.