Monthly Market Risk Update: April 2024 [SlideShare]
Insurance claim form for roof, exterior, interior repairs
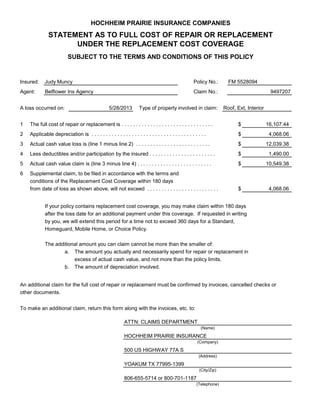
1. HOCHHEIM PRAIRIE INSURANCE COMPANIES
STATEMENT AS TO FULL COST OF REPAIR OR REPLACEMENT
UNDER THE REPLACEMENT COST COVERAGE
SUBJECT TO THE TERMS AND CONDITIONS OF THIS POLICY
Insured: Policy No.:
Agent: Claim No.:
A loss occurred on: Type of property involved in claim:
1 $
2 $
3 $
4 $
5 $
6
$
If your policy contains replacement cost coverage, you may make claim within 180 days
after the loss date for an additional payment under this coverage. If requested in writing
by you, we will extend this period for a time not to exceed 360 days for a Standard,
Homeguard, Mobile Home, or Choice Policy.
The additional amount you can claim cannot be more than the smaller of:
a. The amount you actually and necessarily spend for repair or replacement in
excess of actual cash value, and not more than the policy limits.
b. The amount of depreciation involved.
An additional claim for the full cost of repair or replacement must be confirmed by invoices, cancelled checks or
other documents.
To make an additional claim, return this form along with the invoices, etc. to:
(Name)
(Company)
(Address)
(City/Zip)
(Telephone)
16,107.44
4,068.06
The full cost of repair or replacement is . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Supplemental claim, to be filed in accordance with the terms and
conditions of the Replacement Cost Coverage within 180 days
Applicable depreciation is . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Actual cash value loss is (line 1 minus line 2) . . . . . . . . . . . . . . . . . . . . . . . . . .
Less deductibles and/or participation by the insured . . . . . . . . . . . . . . . . . . . . . . .
Actual cash value claim is (line 3 minus line 4) . . . . . . . . . . . . . . . . . . . . . . . . . .
YOAKUM TX 77995-1399
806-655-5714 or 800-701-1187
500 US HIGHWAY 77A S
Judy Muncy
Belflower Ins Agency
5/28/2013
FM 5528094
9497207
Roof, Ext, Interior
ATTN: CLAIMS DEPARTMENT
HOCHHEIM PRAIRIE INSURANCE
4,068.06from date of loss as shown above, will not exceed . . . . . . . . . . . . . . . . . . . . . . . . .
12,039.38
1,490.00
10,549.38