
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Fibroma
Similar to Fibroma (20)
More from ishita1994
More from ishita1994 (20)
Recently uploaded
Recently uploaded (20)
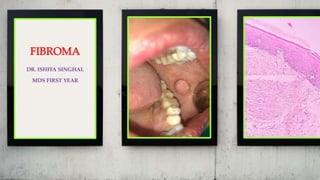
Fibroma
- 1. DR. ISHITA SINGHAL MDS FIRST YEAR
- 2. PERSONAL DATA CASE NO. 1 OPD NO. 567287 NAME SUNITA AGE 48 YEARS SEX FEMALE ADDRESS HARYANA RELIGION HINDU
- 3. CHIEF COMPLAINT Patient complained of growth on the left side of the cheek since 1.5 years.
- 4. ONSET Since 1.5 years. ASSOCIATED SYMPTOMS Small growth in the associated area.
- 5. Past Medical History – No relevant history Family History – No relevant family history Past Dental History – Restorations - 46 General Physical Gait – Normal Built, Co-operative with Normal Gait
- 6. PERSONAL HISTORY Married/ Unmarried –Married Educational Status – 12th pass HABITS Patient cleaned her teeth with toothpaste once daily for 2 minutes She had no deleterious habits
- 7. EXTRA ORAL EXAMINATION Patient was Fair Lips were Normal Pink in Colour
- 8. TMJ Movements Clicking – Mild clicking sound audible on the left side Deviation – Mandible is deviated towards the left side Lymph Nodes – Non-palpable
- 9. INTRA ORAL EXAMINATION Number Of Teeth Present - 32 Missing Teeth – NIL Supernumerary Teeth – NIL Mobility – NIL Caries – 16, 17, 28, 34, 36, 46 and 47 Abrasion – 26, 35, 37, 38, 44, 45 and 47 Plaque & Calculus – Generalised Moderate Calculus Present Gingiva – Reddish Pink, Scalloped, Soft and Oedematous
- 10. GROWTH Number – 1 Location And Extent – i.r.t. 27, 28, 37 and 38 regions Size – 1.5 cm x 1.5 cm Colour – Normal Pink and Shiny Shape – Round Borders – Well Elevated Borders Consistency – Firm and Sessile Non-Fluctuant Non-Tender
- 11. Contoso S u i t e s SINGLE PINK AND SHINY GROWTH ROUND SHAPE WITH WELL ELEVATED BORDERS i.r.t. 27, 28, 37 AND 38 REGIONS
- 12. PROVISIONAL DIAGNOSIS On the basis of Clinical presentation of the growth, the provisional diagnosis of Irritational Fibroma i.r.t. Left Buccal Mucosa was made
- 13. DIFFERENTIAL DIAGNOSIS 1. Irritational Fibroma 2. Pyogenic Granuloma 3. Lipoma 4. Neurofibroma
- 14. INVESTIGATIO N HEMOGRAM – 1. HB - 12.8 gm% 2. BT - 1 minute 10 seconds 3. CT - 6 minutes 20 seconds DLC – 1. Monocytes - 03 % 2. Eosinophils - 02 % 3. Basophils - 00 % 4. Leukocytes - 30 % 5. Neutrophils - 65 % TLC - 7300 /C mm
- 15. BIOPSY Excisional biopsy was done in the Department of Oral and Maxillofacial Surgery and the tissue was sent to the Department of Oral Pathology for histopathological examination
- 16. MACROSCOPIC DETAILS Received 1 small soft tissue specimens measuring 1 cm x 1 cm Firm in consistency Creamy-white in colour
- 17. MICROSCOPIC EXAMINATION The H & E stained tissue section revealed epithelial and connective tissue stroma. Epithelium was stratified squamous with underlying connective tissue exhibiting dense collagen bundles arranged in haphazard manner, mild inflammatory cell infiltrate and blood vessels. Deeper section showed adipose tissue.
- 18. Contoso S u i t e s OVERLYING EPITHELIUM UNDERLYING CONNECTIVE TISSUE WITH ADIPOSE TISSUE
- 19. Contoso S u i t e s PARAKERATINIZED STRATIFIED SQUAMOUS EPITHELIUM MILD INFLAMMATORY CELLS AND BLOOD VESSELS DENSE COLLAGEN BUNDLES BROAD RETE RIDGES
- 20. FINAL DIAGNOSIS The Histopathological features were suggestive of Fibroma i.r.t. 27,28,37 and 38 regions
- 22. DEFINITION It is also called Oral Fibroma or Irritational Fibroma or Focal Fibrous Hyperplasia. Fibroma is a benign neoplasm of fibrous connective tissue origin. It is characterized by excessive proliferation of fibroblast cells with synthesis of large amount of collagen.
- 23. ETIOLOGY Although a large number of fibrous over-growths are found inside the oral cavity, most of these are reactive lesions occurring as a result of trauma or local irritation and therefore true fibromas are extremely rare. Jain G et al (2017) stated that traumatic irritants include calculi, foreign bodies, overhanging margins, restorations, margins of caries, chronic biting, sharp spicules of bones, and overextended borders of appliances. Fibroma, a benign neoplasm of fibroblastic origin, is reactive in nature and represents a reactive hyperplasia of fibrous connective tissue in response to local irritation or trauma rather than being a true neoplasm. Jain G, Arora R, Sharma A, Singh R, Agarwal M. Irritation fibroma: Report of a case. J Curr Res Sci Med 2017;3:118-21.
- 24. CLINICAL FEATURES Age: Fibromas commonly develop in the third, fourth and fifth decade of life. Sex: They are more common among females. Ratio: Male: Female - 1:2 Site: Intraoral fibromas often develop from the gingiva, however, these lesions may also develop from buccal mucosa, tongue, lips and palate as well. SHAFER’S TEXTBOOK OF ORAL PATHOLOGY 7TH EDITION
- 25. CLINICAL PRESENTATION Clinically, fibromas appear as small, asymptomatic, round or oval, well-circumscribed, slow enlarging, nodular growths in the oral cavity. The size varies between 1 to 2 cm in diameter. These lesions can be either pedunculated or sessile and their surface is usually smooth. On palpation, these lesions are either soft or firm in consistency and the overlying covering epithelium often appears normal in colour. Persistent trauma or injury to these lesions often causes pain, inflammation or surface ulceration. Sometimes , the surface may be hyperkeratotic. SHAFER’S TEXTBOOK OF ORAL PATHOLOGY 7TH EDITION
- 26. NEVILLE’S TEXTBOOK OF ORAL AND MAXILLOFACIAL PATHOLOGY 3RD EDITION
- 27. DIFFERENTIAL DIAGNOSIS Mortazavi H, Safi Y, Baharvand M, Rahmani S, Jafari S. Peripheral Exophytic Oral Lesions: A Clinical Decision Tree. Int J Dent. 2017;2017:9193831.
- 28. HISTOLOGICFEATURES The fibroma consists of bundles of interlacing collagenous fibers interspersed with varying number of fibroblasts or fibrocytes and small blood vessels. The overlying epithelium is thin stratified squamous epithelium which frequently appears stretched and it often shows shortening and flattening of the rete pegs. In few cases, vasodilation, edema and chronic inflammatory cell infiltration may be found within the connective tissue stroma, especially, those lesions which are often traumatized or ulcerated. SHAFER’S TEXTBOOK OF ORAL PATHOLOGY 7TH EDITION
- 29. NEVILLE’S TEXTBOOK OF ORAL AND MAXILLOFACIAL PATHOLOGY 3RD EDITION
- 30. Fibroma, a true neoplasm of connective tissue origin, is microscopically similar to the condition known as inflammatory hyperplasia, an increased bulk of connective tissue which forms as part of an inflammatory reaction. Hyperplasia is usually considered to be a self limiting process which is not etiologically related to neoplasia. Both processes, however, are typified by an increase in the number of cells brought about by increased mitotic activity. Hyperplastic tissue sometimes, but not invariably, regresses after the removal of the stimulus or irritant. Neoplastic tissue shows no such regression. SHAFER’S TEXTBOOK OF ORAL PATHOLOGY 7TH EDITION
- 31. TREATMENT By surgical excision. Jiang M et al (2019) stated that complete excision is the recommended treatment for irritation fibroma. Other therapies including cryosurgery or intralesional injection of corticosteroids can be considered on condition that there is a definitive diagnosis based on histopathologic findings. Jiang M, Bu W, Chen X, Gu H. A case of irritation fibroma. Postepy Dermatol Alergol. 2019;36(1):125–126.
- 32. REFERENCES SHAFER’S TEXTBOOK OF ORAL PATHOLOGY 7TH EDITION NEVILLE’S TEXTBOOK OF ORAL AND MAXILLOFACIAL PATHOLOGY 3RD EDITION Jain G, Arora R, Sharma A, Singh R, Agarwal M. Irritation fibroma: Report of a case. J Curr Res Sci Med 2017;3:118-21. Mortazavi H, Safi Y, Baharvand M, Rahmani S, Jafari S. Peripheral Exophytic Oral Lesions: A Clinical Decision Tree. Int J Dent. 2017;2017:9193831.