Liver kidney microsomal antibody detection and clinical significance
•Download as PPTX, PDF•
5 likes•1,528 views


Recommended
More Related Content
What's hot
What's hot (20)
Similar to Liver kidney microsomal antibody detection and clinical significance
Similar to Liver kidney microsomal antibody detection and clinical significance (20)
More from eman youssif
Recently uploaded
Recently uploaded (20)
Liver kidney microsomal antibody detection and clinical significance
- 2. Liver kidney microsomal antibody Eman abd elraouf ahmed
- 3. introduction The liver is an important organ with responsibility for many critical functions (for example, metabolism of protein and fats, storage, bile acid production and detoxification (toxic drugs & chemicals). Inability to perform these functions leads to liver disease. In this section, autoimmune liver disease (such as autoimmune hepatitis (AIH), primary biliary cirrhosis (PBC), primary sclerosing cholangitis (PSC), and autoimmune cholangiopathy and overlap syndromes)
- 4. Autoimmune liver diseases A variety of clinical signs and symptoms may be associated with the liver disease and the evidence of autoimmune involvement is characterized by chronic progressive inflammation and hyper gamma globulinaemia and the presence of specific high tire auto- antibodies is often evident.
- 5. Primary Biliary Cirrhosis (PBC): Anti-mitochondrial antibodies (AMA) are associated with this disease and affects older females with an incident of 90%. The cause is unknown but it is thought that infection might be a trigger. The most common target for these antibodies is M2 antigen, the pyruvate dehydrogenase complex. A number of the subunits of the pyruvate dehydrogenase may be targeted.
- 6. Autoimmune hepatitis (AIH) This affects about 90% of younger female patients and is categorised by seropositivity for antinuclear antibody (ANA) and/or smooth muscle or antibodies to liver kidney microsomes (LKM). Type 1 AIH is associated with high titre of ANA and /or AMA, whereas type 2 AIH is associated with LKM. There are several antigens identified associated with AIH, for example, liver kidney microsome, liver cytosolic (LC-1), liver cytokeratine, glutathione-S-transferase, soluble liver antigen, actin in smooth muscle and ANA.
- 7. Table: Summary of antibodies in liver disease
- 10. Note: Anti-mitochondria antibodies (AMAs) are observed on rat or mouse kidney sections .Cytoplasmic speckling can also be seen in liver. The antibodies are important in the investigation of liver disease such as chronic active hepatitis, autoimmune hepatitis and PBC. Mitochondria antibodies can be detected in patient serum years before symptoms manifest. The assay is 95% specific for the disease. In PBC the mitochondria antigen is pyruvate dehydrogenase. A simple ELISA assay can be performed to confirm the presence of M2 antibodies that are relevant to PBC.
- 11. AMA
- 13. Other mitochondrial antibodies can also be viewed by immunofluorescence. The clinical significance of these antibodies is described in Table 1.
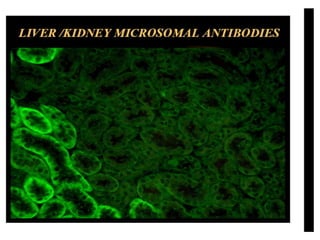
- 14. Liver-kidney microsomal antibodies (LKM) bind to both cytochrome P450 in hepatocytes and proximal renal tubes in rodent tissue .
- 15. Immunofluorescence pattern of LKM1 antibodies on liver (left) and kidney (right). Staining of proximal tubules can be observerved on the kidney, whereas distal tubules remain unstained.
- 16. Revision notes: Several subtypes of anti-liver-kidney microsomal antibodies (LKM) are known. LKM-1 antibodies associated with autoimmune chronic active hepatitis recognize P450 2D6, a cytochrome P450 mono-oxygenase. The frequent association of anti-LKM-1 antibodies and hepatitis C virus (HCV) infections and the probable existence of an infectious and autoimmune form of anti-LKM-1-associated hepatitis, requiring different therapeutically strategies, necessitates the exact determination of anti- LKM-1 specificities.
- 17. Remember: Liver/kidney microsomal antibody type 1 (LKM1) is the marker of type 2 autoimmune hepatitis (AIH) and is detected in up to 6% of patients with hepatitis C virus (HCV) infection.
- 18. The presence of LKM1 in the plasma membrane was investigated by indirect immunofluorescence.
- 19. TEST Screening test for detection of IgG autoantibodies against Smooth muscle, Mitochondria and Liver Kidney Microsomal antigens. Clinical Indications: Primary Biliary Cirrhosis Autoimmune hepatitis Please note: Low titre antibodies may be found in normal people and in a variety of diseases without an autoimmune basis, such as inflammation and cancer. The prevalence of these antibodies increases with age, but in general titres of greater that 1/80 are often significant disease indicators. Low or absent titres do not exclude disease in the presence of relevant clinical features
- 20. Specimen Serum Volume 7 ml Container Red top tubeVacutainer red top Collection Samples should be transported to the laboratory immediately Lab Handling Aliquot and store at 4°C prior to testing and at -20°C or below for 3 months after receipt
- 21. Causes for Rejection Unlabelled/inadequately labelled sample Inadequately completed request form Delay in sample reaching laboratory Reference Range Sera are screened at a dilution of 1/20 (paediatric samples 1/10). In general titres greater or equal to 1/80 are often significant. Samples found to be anti mitochondrial positive will be referred for M2 antibodies. Samples found to be positive at 1/20 may be referred for other Liver Specific Antibodies if clinical details and pattern observed indicate testing. Below are listed the most common reported antibodies and their main clinical association: Mitochondrial antibody - Primary Biliary Cirrhosis, autoimmune thyroiditis and Sjogren's syndrome. Smooth muscle antibody - autoimmune hepatitis, viral infections, SLE and RA. Liver Kidney Microsomal Antibody- Autoimmune and drug induced hepatitis infections
- 23. Thank u