
Recommended
Recommended
More Related Content
Similar to Discussion #1 for Week 5RubricsWeekly Participation.docx
Similar to Discussion #1 for Week 5RubricsWeekly Participation.docx (12)
More from cuddietheresa
More from cuddietheresa (20)
Recently uploaded
Recently uploaded (20)
Discussion #1 for Week 5RubricsWeekly Participation.docx
- 1. Discussion #1 for Week 5 Rubrics Weekly Participation IFSM 305 7980 Information Systems in Health Care … Topic: Identify the ethical, legal and regulatory policy issues related to health care information systems. Last week's readings covered ethical, legal and regulatory policy issues related to health care information systems. As you work on your Stage 3 assignment, you will provide definitions for a list of these issues and policies, and explain their impact on the implementation and use of health care IT systems. GROUP 1: Review the list of 20 ethical, legal and regulatory topics in the Stage 3 assignment. Select one (preferably different from others previously chosen, but this is not required) and: 1. Put the topic in the Subject line of your posting
- 2. 2. Discuss an event in your life that relates to that topic a. What it meant to you b. What suggestions you have for improving the outcome or ensuring that others benefit if it was a positive outcome. GROUPS 2, 3 and 4: For at least two postings, respond by discussing your own experience with that topic and your suggestion(s) for improving the outcome or ensuring that others benefit if it was a positive outcome. EVERYONE: Review the criteria in the Discussion Grading Rubric, and reply to those who critique your work or post other points of view. Be sure to demonstrate your understanding of the topic and analytical thinking. https://learn.umuc.edu/d2l/le/content/418648/navigateContent/5 19/Previous?pId=16194506 https://learn.umuc.edu/d2l/le/content/418648/navigateContent/5 19/Next?pId=16194506 javascript:void(0); https://learn.umuc.edu/d2l/home/418648 Start a New Thread
- 3. Filter by: Sort by: Most Recent Activity All Threads Falilat : "Security" Falilat Omolabi posted Nov 18, 2019 2:47 PM 0 Unread 0 Replies 1 Views Subscribe 1. Put the topic in the Subject line of your posting “A di t Th N ti l I tit t f St d d d T h l (NIST) it i “th more Authentication Laura Darley posted Nov 18, 2019 12:56 PM 0 Unread 0 Replies 0
- 4. Views Subscribe As the use of EHR systems for medical practice are on the rise, security of patient sensitive data is a major force for the authentication policies. The most common type of data stolen i l d ti t’ l i f ti lik SSN’ ll id tifi bl d t i more Authorization Alexander Krasnokutsky posted Nov 18, 2019 9:47 AM 0 Unread 0 Replies 2 Views Subscribe Authorization is the process of authorizing or assigning permissions to users so that they gain access to a resource. These resources could be in the form of data files, program permissions, d t d l ti A th i ti t l i t b t l more
- 5. javascript:void(0) javascript:void(0) javascript:void(0) 1 / 1 Task: Reply to this topic Assessment Weekly Discussions Activity Details https://learn.umuc.edu/d2l/le/content/418648/navigateContent/5 19/Previous?pId=16194506 https://learn.umuc.edu/d2l/le/content/418648/navigateContent/5 19/Next?pId=16194506 javascript:void(0); javascript:void(0); Content Week 4, Monday, November 11, 2019 - Sunday, November 17, 2019 IFSM 305 7980 Information Systems in Health Care … The following should be completed in Week 4: Read: Read/View all Week 4 Content
- 6. Do: Participate in Discussion(s), as assigned Submit the Case Study Stage 2 Assignment 0 % 0 of 3 topics complete The second of two weeks on data, this week you will learn more about how data is used to support decision making in health care organizations and how data is protected. Health care data is by definition personal and private, so we will also address issues of ethics and professionalism surrounding data and how health information can be protected. The following table lists the Week 4 outcomes, mapped to the corresponding course outcome. The course outcome gives you "the big picture," and the weekly outcomes provide more detailed information that will help you achieve the course outcome. Course Outcome Met in Week 4 Week 4 Outcomes Analyze the flow of data and explain how clinical decision
- 7. support javascript:void(0); https://learn.umuc.edu/d2l/home/418648 Activities Week 4 Learning Resources Link Discussion for Week 4 Discussion Topic Case Study Stage 2 Assignment Assignment Due November 17 at 11:59 PM information among disparate health information systems to support internal and external business processes systems support health care quality improvement describe the privacy, confidentiality, an security issues with health care data describe methods for protecting health
- 8. care data explain the ethical issues in health informatics javascript:void(0); https://learn.umuc.edu/d2l/le/content/418648/viewContent/1619 4554/View https://learn.umuc.edu/d2l/le/content/418648/viewContent/1619 4543/View https://learn.umuc.edu/d2l/le/content/418648/viewContent/1619 4549/View Working with Health IT Systems is available under a Creative Commons Attribution-NonCommercial- ShareAlike 3.0 Unported license. © Johns Hopkins University. UMUC has modified this work and it is available under the original license. http://knowledge.amia.org/onc-ntdc/working-with-health-it- systems-1.379705 https://creativecommons.org/licenses/by-nc-sa/3.0/us/ https://creativecommons.org/licenses/by-nc-sa/3.0/us/ Welcome to Health Management Information Systems, Clinical Decision Support Systems. This is Lecture a. The component, Health Management Information Systems, is a “theory” component that provides an introduction to health care applications and the systems that use them, health information
- 9. technology standards, health-related data structures, and enterprise architecture in health care organizations. Lecture a will offer a definition of clinical decision support, provide some historical context surrounding clinical decision support, describe the requirements of a clinical decision support system, and discuss the relationship of clinical practice guidelines and evidence-based practice to clinical decision support systems. 1 The objectives for this unit, Clinical Decision Support Systems are to: • Describe the history and evolution of clinical decision support; • Describe the fundamental requirements of effective clinical decision support systems; • Discuss how clinical practice guidelines and evidence-based practice affect clinical decision support systems; 2
- 10. Additional objectives for this unit, Clinical Decision Support Systems are to: • Identify the challenges and barriers to building and using clinical decision support systems; • Discuss legal and regulatory considerations related to the distribution of clinical decision support systems; • and Describe current initiatives that will impact the future and effectiveness of clinical decision support systems. 3 Osheroff, Pifer, & Teich (as cited in Das & Eichner, 2010) stated “CDS provides clinicians, patients, or caregivers with clinical knowledge and patient-specific information to help them make decisions that enhance patient care” (Das & Eichner, 2010, p. 4). Das & Eichner (2010) go on to explain “The patient’s information is matched to a clinical knowledge base, and patient-specific assessments or recommendations are then communicated effectively at appropriate times during patient care” (p. 4).
- 11. Musen, Shahar, and Shortliffe (2006) define a clinical decision support system as “any computer program designed to help healthcare professionals to make clinical decisions” (p. 700). Bottom line, when one hears CDS or CDSS, think of computer- assisted clinical decision-making. 4 Computer-assisted clinical decision-making has been considered viable since the late 1950s when initial publications appeared. Then in the late 1960s, the Leeds Abdominal Pain System was created at the University of Leeds. The Leeds Abdominal Pain System was built based on “computer-based decision aids using Bayesian probability theory” (Musen, Shahar, & Shortliffe, 2006, p. 702). While it is not possible to explain the theory in depth in this short course, it is important to know the theorem is based on rules of predictive probability. A clinical decision support system may use Bayesian logic in its inference engine. 5
- 12. Other systems considered to be key in the evolution of clinical decision support systems are MYCIN and HELP, both of which used rule-based approaches. According to HIMSS, a rule is “A formal way of specifying a recommendation, directive, or strategy, expressed as ‘IF premise THEN conclusion’ or ‘IF condition THEN action’” (HIMSS Dictionary, 2010, p. 105). MYCIN, which uses a rules-based methodology, is described by Musen, Shahar, & Shortliffe as “…an early exploration of methods for capturing and applying ill-structured expert knowledge to solve important medical problems” (p. 705). HELP, an integrated clinical information system, has decision rules called “HELP sectors” encoded into it (Musen, Shahar, & Shortliffe, 2006, p. 705). Kuperman, Gardner, & Pryor, (as cited in Musen, Shahar, & Shortliffe, 2006) stated, “HELP has the ability to generate alerts when abnormalities in the patient record are noted, and its impact on the development of the field has been immense, with applications and methodologies that span nearly
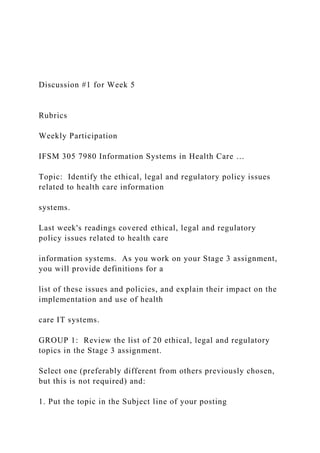
- 13. the full range of activities in biomedical informatics” (p. 705). In addition to Bayesian logic and rule-based approaches, the current clinical decision support systems may use other reasoning methodologies such as neural networks or combinations of several methods. 6 Two Healthcare Information Technology Standards Panel (HITSP) groups convened a meeting with experts in the area of clinical decision support systems and one outcome was the image shown on this slide. As explained by Boone (2006) in his blog, clinical decision support was “…viewed as a black box, through which we have three different kinds of inputs, and several different types of outputs… The three different inputs include: 1. Algorithms, or knowledge about how to make inferences or assertions based on existing instance or world knowledge. 2. Instance data describing the specific case that is being addressed by the clinical decision support application.
- 14. 3. Ontological or "world knowledge", representing facts about the world, such as what drugs interact badly, or how body parts are related, or the relationships between genes and diseases” (para. 13). The output of information, actions, and alerts is characterized by symbols shown coming from the black box representing clinical decision support. This image of a model is representative of the components of clinical decision support. 7 As the previous slide showed, a model of a clinical decision support involves certain inputs in order to arrive at an output. Berner (2009) explains the system requirements in the following way: “Common features of CDS systems that are designed to provide patient-specific guidance include the knowledge base (e.g., compiled clinical information on diagnoses, drug interactions, and guidelines), a program for combining that knowledge with
- 15. patient-specific information, and a communication mechanism— in other words, a way of entering patient data (or importing it from the EMR) into the CDS application and providing relevant information (e.g., lists of possible diagnoses, drug interaction alerts, or preventive care reminders) back to the clinician” (p. 5). Each component provides a piece that is important for clinical decision support interventions to occur. For example, clinical decision support could provide suggestions for possible diagnoses (knowledge base) that match a patient’s signs and symptoms (inference engine) and communicate this to the provider through a ranked list of diagnoses that might explain the patient’s signs and symptoms (communication mechanism). 8 The first system requirement is the knowledge base. A knowledge base is just what you would expect it to be, that is an automated representation of clinical knowledge.
- 16. Osheroff et al. (2006) defined clinical knowledge as “A generally applicable fact (or set of facts), best practice, guideline, logical rule, piece of reference information (such as a text article), or other element of information that is important to know for optimal data interpretation and decision-making regarding individual and population health and health care delivery” (p. 59). The knowledge base is a collection of clinical information on such things as diagnoses, drug interactions, and evidence-based guidelines. Content for the knowledge base comes from internal as well as external sources such as specialty societies, commercial knowledge vendors, and health care organizations. Because of amount of time and expertise it takes to create content, healthcare providers usually depend on developers of clinical information systems for the knowledge base who often will obtain and incorporate commercial knowledge bases into their CDS products. For example, a number of drug knowledge bases are available in the marketplace. 9
- 17. The second system requirement is the inference engine. In a clinical decision support system, the inference engine combines the knowledge base with the patient’s data. According to Spooner (2007), “The inference engine is the portion of the CDSS that combines the input and other data according to some logical scheme for output…One such scheme for an inference engine is the Bayesian network… A Bayesian network is a way to put Bayes’ rule to work by laying out graphically which events influence the likelihood of occurrence of other events” (p. 37). As mentioned previously, in addition to Bayesian logic, clinical decision support systems may use other reasoning methodologies such as rule-based approaches. 10 The final system requirement is the communication mechanism. Berner (2009) describes this component as a mechanism for entering patient data into the CDS application and providing relevant information back to the clinician.
- 18. One method for input would be importing it from the electronic medical record. Some examples of information that might be output are lists of possible diagnoses, drug-allergy alerts, duplicate testing reminder, drug interaction alerts, drug formulary guidelines, or preventive care reminders. One of the five rights in the CDS Five Rights model is communication occurs to the right person, that is consideration of all members of the care team, such as the clinician, patient, parent or caregiver, nurse (Sirajuddin et al., 2009, p. 40). 11 Given the components of a CDSS, what are some expectations of its use? Berner (2009) provided examples shown in Table 5.1 of CDS interventions by target area of care. The first row in Table 5.1 states the target area of care as preventive care with intervention examples of immunization, screening,
- 19. and disease management guidelines for secondary prevention. The second row lists diagnosis as the target area of care, where clinical decision support could provide suggestions for possible diagnoses that match a patient’s signs and symptoms. The third row on the list is the target area planning or implementing treatment. CDS intervention could entail the display treatment guidelines for specific diagnoses, drug dosage recommendations, or alerts for drug-to-drug interactions. The fourth row, follow-up management, is the target area of care for clinical decision support an intervention might involve information about corollary orders or reminders for drug adverse event monitoring. The fifth row states the target area of care as hospital or provider efficiency with care plans to minimize length of stay or the presentation of order sets as examples of CDS intervention. 12 The sixth and final row is the target area cost reductions and
- 20. improved patient convenience. Examples of CDS interventions include duplicate testing alerts and drug formulary guidelines. Thus, CDS interventions can assist health care providers at different stages in the care process, that is, from preventive care through diagnosis and treatment, all the way to monitoring and follow- up. 12 Osheroff et al. (2006) describes CDS interventions as “…alerts, reminders, and order sets, as well as other techniques for knowledge delivery including reference information and education (delivered with or without context sensitivity), health/clinical protocol and workflow orchestration support, display of context-relevant data, topic-oriented documentation forms, and others” (p. 59). Intervention types and examples as summarized by Osheroff (2009) are shown in table 5.2. While typically several elements from these types are combined
- 21. in the clinical decision support intervention, each of these intervention types will be examined independently in the next several slides. Drawing from Osheroff, Pifer, Teich, Sittig, & Jenders, (2005) AHRA provides an example of a combination of elements as “an order set might highlight—through a non- interruptive alert—an essential intervention that should routinely be ordered and provide an infobutton link to more detailed reference information that supports the clinical recommendation” (AHRQ, n.d., para 2). 13 Each major CDS intervention type results in certain benefits and can be further broken down into subtypes. The benefits of the documentation forms/templates intervention include the ability to “provide complete documentation for care quality/continuity, reimbursement, legal requirements; reduce omission errors by displaying items for selection; reduce commission errors by ensuring critical data—such as allergies—are captured; provide coded data for other data-driven CDS; provide prompts to acquire specific information in the format desired” (Osheroff et al., 2005).
- 22. Subtypes along with examples as summarized by Osheroff et al. (2005) are shown in table 5.3. Row one lists the subtype of patient self-assessment forms with the example of a pre-visit questionnaire that outlines health problems and current medications. The second row identifies the subtype of clinician patient assessment forms and an inpatient assessment as its example. Clinician encounter documentation forms is the third subtype and a structured history and physician examination template is an example. The fourth row refers to departmental/multidisciplinary clinical documentation forms as a subtype and emergency department 14 document as an example. The fifth and final row lists data flowsheets as a subtype and the example of a health maintenance/disease management form. 14
- 23. The relevant data presentation intervention has several benefits. They include the ability to “optimize decision making by ensuring all pertinent data are considered and to organize complex data collections to promote understanding of overall clinical picture and to highlight needed actions” (Osheroff et al., 2005). Subtypes and examples for this intervention as summarized by Osheroff et al. (2005) are shown in table 5.4. Row one lists the subtype of relevant data for ordering, administration, or documentation with the example of a longitudinal display of key patient information to highlight trends and issues requiring attention. The second row identifies the subtype of retrospective/aggregate reporting or filtering and adverse drug event tracking as its example. Environmental parameter reporting is the third subtype and recent hospital antibiotic sensitivities is an example.
- 24. The fourth row refers to choice lists as a subtype and suggested dose choice lists, possibly modified as needed for patient’s kidney or liver function and age as an example. 15 The fifth and final row lists practice status display as a subtype and the example of ED tracking display. 15 The benefit to order/prescription creation facilitators include “promote adherence to standards of care by making the right thing the easiest to do” (Osheroff et al., 2005). The subtypes and examples for the order/prescription creation intervention as summarized by Osheroff et al. (2005) are shown in table 5.5. Row one lists the subtype of single-order completers including consequent orders with the example of suggested drug and/or dose
- 25. choice lists integrated into ordering function—possibly modified by patient’s kidney or liver function and age. Order sets is the third subtype and general order sets such as an order set for hospital admission or problem-oriented ambulatory visit is an example. The third and final row identifies tools for complex ordering as a subtype and the example of guided dose algorithms based on weight, body surface area (BSA), kidney function, etc. 16 The next intervention is protocol/pathway support. The benefit of this intervention is that it “Provides support for multistep care plans, pathways, and protocols that extend over time” (Osheroff et al., 2005). As summarized by Osheroff et al. (2005), table 5.6 identifies two subtypes and examples for the protocol/pathway support intervention. Row one lists the subtype of stepwise processing of multi-step
- 26. protocol or guideline with the example of tools for monitoring and supporting inpatient clinical pathways (for example, for pneumonia admissions) and multiday/multi-cycle chemotherapy protocols in the inpatient or outpatient setting. Support for managing clinical problems over long periods and many encounters is the second subtype and computer-assisted management algorithm for treating hyperlipidemia over many outpatient visits is an example. 17 "Address recognized information needs of patients and clinicians" (Osheroff et al., 2005) is a benefit of the CDS intervention type, reference information and guidance. The subtypes and examples as summarized by Osheroff et al. (2005) are shown in table 5.7. Row one lists the subtype of context-insensitive with the example of a general link from EMR or clinical portal to a reference program (at table of contents or general-search level).
- 27. The second row identifies the subtype of context-sensitive and link within patient-messaging application to relevant patient drug information leaflets as its example. 18 The final intervention is alerts and reminders. The benefits to this intervention include “provide immediate notification of errors and hazards related to new data or orders entered by clinical information system (CIS) user or the CIS itself (such as when abnormal lab result is posted) or passage of a time interval during which a critical event should occur; help enforce standards of care. Effectiveness requires careful attention to workflow, high value of information to end user, and other factors” (Osheroff et al., 2005). The subtypes and examples for the alerts and reminders intervention as summarized by Osheroff et al. (2005) are shown in table 5.8. The first row refers to alerts to prevent potential
- 28. omission/commission errors or hazards as a subtype and drug interaction alert, for example, with drugs, pregnancy, laboratory, food as an example. Row two lists the subtype alerts to foster best care and the example disease management such as an alert for needed therapeutic intervention based on guidelines/evidence and patient-specific factors. 19 This image is an example of the subtype alerts to prevent potential omission/commission errors or hazards. The screen shot depicts an example of a CDS drug warning alert. The warning indicates the patient is currently on another drug and to avoid use due to a patient’s possible allergy to cephalosporins. The user has different options to consider, including canceling or continuing with the order thereby overriding the alert. 20
- 29. As mentioned previously, requirements for clinical decision support include the knowledge base, inference engine, and the communication mechanism. Each component provides a piece that is essential for clinical decision support interventions to occur. Since clinical decisions are made based on the intervention, then the accuracy and reliability of the knowledge base is vitally important. Clinical best practices and evidence-based medicine are important to the trustworthiness of the knowledge base or its rules and associations of compiled data. Osheroff et al. (2006) explain CDS has the capability of having the scientific evidence and clinical best practices be more available and helpful and “in so doing adds substantially to the value of health information technology such as EHRs and CPOE …It is only through CDS that EHRs and CPOE can achieve their full potential for improving the safety, quality and cost-effectiveness of care” (p.22).
- 30. 21 Clinical practice guidelines are a foundational part of the knowledge base. The Quality Assurance Project (QAP), funded by the U.S. Agency for International Development, includes a glossary of useful terms. According to Marquez (2001) “Practice guidelines consist of systematically developed statements, usually based on scientific evidence and expert consensus, to assist practitioner decision making about appropriate care for a specific clinical situation” (p. 5). A similar definition from the National Library of Medicine (NLM) defines a clinical practice guideline as “Work consisting of a set of directions or principles to assist the health care practitioner with patient care decisions about appropriate diagnostic, therapeutic, or other clinical procedures for specific clinical circumstances. Practice guidelines may be developed by government agencies at any level, institutions, organizations such as professional societies or governing boards, or by the convening of expert panels. They can
- 31. provide a foundation for assessing and evaluating the quality and effectiveness of health care in terms of measuring improved health, reduction of variation in services or procedures performed, and reduction of variation in outcomes of health care delivered” (NLM, 2012). Clinical practice guidelines are central to determining the care plan for a patient and are considered to be the preferred process for care. 22 As the previous slide noted, there a number of places where clinical practice guidelines can be located. For example, government agencies, institutions, professional societies, or expert panels may generate them. Clinical practice guidelines “…can provide a foundation for assessing and evaluating the quality and effectiveness of health care in terms of measuring improved health, reduction of variation in services or procedures performed, and reduction of variation in outcomes of health care delivered. Clinical or practice
- 32. guidelines usually cite references from a research study whose findings were used to support the recommendations as noted in the guideline” (Becker Medical Library, 2010, para. 2, 3) 23 The National Guideline Clearinghouse (NGC), a program of the Agency for Healthcare Research and Quality (AHRQ), was formed as a partnership with the American Medical Association and the American Association of Health Plans (now America's Health Insurance Plans [AHIP]). The NGH is a public resource for evidence-based clinical practice guidelines. The image shown is a screen shot taken from AHRQ’s National Guideline Clearinghouse. It shows a portion of the clinical practice guideline for using nontraditional risk factors in coronary heart disease risk assessment. The source of this guideline is the U.S. Preventive Services Task Force, a federally-appointed panel of independent experts. It is an example of a source for clinical practice guidelines from a government agency. 24
- 33. Clinical practice guidelines which are based on evidence present the strongest case for accuracy and reliability. The National Library of Medicine (NLM) defines evidence-based practice as “A way of providing health care that is guided by a thoughtful integration of the best available scientific knowledge with clinical expertise. This approach allows the practitioner to critically assess research data, clinical guidelines, and other information resources in order to correctly identify the clinical problem, apply the most high-quality intervention, and re-evaluate the outcome for future improvement” (NLM, 2012). The practice of evidence-based medicine is supported through the provision of clinical decision support systems. As Berner (2009) emphasized, “…the quality of the information and the evidence underlying it are the major determinants of the impact of clinical decision support on patient safety and quality improvement” (p. 7). The accuracy and reliability of the knowledge base is vitally important since clinical decisions are being made based on the intervention. Clinical best practices and evidence-based
- 34. medicine are essential to the trustworthiness of the knowledge base. Through the provision of clinical decision support systems the practice of evidence-based medicine is supported. While guidelines exist, the reality is the availability and utility of useful guideline representations and user interface issues continue as challenges in CDS deployment. 25 This concludes Lecture a of Clinical Decision Support Systems. This lecture defined clinical decision support, described system requirements, and explained the effects of clinical practice guidelines and evidence-based practice on CDSS. 26 No audio. 27 No audio.
- 35. 28 No audio. 29 No audio. 30 Working with Health IT Systems is available under a Creative Commons Attribution-NonCommercial- ShareAlike 3.0 Unported license. © Johns Hopkins University. UMUC has modified this work and it is available under the original license. http://knowledge.amia.org/onc-ntdc/working-with-health-it- systems-1.379705 https://creativecommons.org/licenses/by-nc-sa/3.0/us/ https://creativecommons.org/licenses/by-nc-sa/3.0/us/ Welcome to Health Management Information Systems, Clinical Decision Support Systems. This is Lecture b.
- 36. The component, Health Management Information Systems, is a “theory” component that provides an introduction to health care applications and the systems that use them, health information technology standards, health-related data structures, and enterprise architecture in health care organizations. Lecture b will identify the challenges and barriers in building and using clinical decision support systems, explain how legal and regulatory technologies may affect their use, and introduce the future directions for clinical decision support systems. 1 The objectives for this unit, Clinical Decision Support Systems are to: • Describe the history and evolution of clinical decision support; • Describe the fundamental requirements of effective clinical decision support systems;
- 37. • Discuss how clinical practice guidelines and evidence-based practice affect clinical decision support systems; 2 Additional Objectives for this unit, Clinical Decision Support Systems are to: • Identify the challenges and barriers to building and using clinical decision support systems; • Discuss legal and regulatory considerations related to the distribution of clinical decision support systems; • and Describe current initiatives that will impact the future and effectiveness of clinical decision support systems. 3 As a framework for supporting clinical decisions to improve outcomes, the CDS Five Rights model states CDS-supported improvements in desired healthcare outcomes can be achieved if
- 38. communication occurs in the following manner: “The right information: Evidence-based, suitable to guide action, pertinent to the circumstance To the right person: Considering all members of the care team, including clinicians, patients, and their caretakers In the right CDS intervention format: Such as an alert, order set, or reference information to answer a clinical question Through the right channel: For example, a clinical information system (CIS) such as an electronic medical record (EMR), personal health record (PHR), or a more general channel, such as the Internet or a mobile device At the right time in workflow: For example, at time of decision/action/need” (Sirajuddin et al., 2009, p. 40). However, achieving the five rights for CDS is challenging.
- 39. Berner (2009) states “Achieving the five rights for CDS presents challenges, and the challenges differ depending on how closely the CDS is tied to what the clinician already intends to do. Clinicians may initially want certain reminders or, after performance assessments, agree that they need other reminders, but in either situation they are choosing to receive the reminders. The key issue in reminding the user about things they choose to be reminded about is the timing of the reminder. For instance, should reminders for preventive care be given to the physician in advance of the patient visit 4 (e.g., the day before), or should the reminders appear during the patient’s visit” (p. 7-8)? 4 Clinical decision support systems offer so much potential to improve patient care and outcomes. Similar challenges in designing and selecting clinical decision support systems to the five rights
- 40. model can be posed as questions. Berner (2009) asked them in the following manner: “whose decisions are being supported, what information is presented, when is it presented, and how is it presented to the user” (p. 6). Each question should be explored and answered before building or selecting a clinical decision support system. If any are ignored, the chances that end-users will use it and the expected system benefits gained are limited. For example, consider the question – when the intervention will be presented? Depending on the information, the best time to deliver could be at the point of care—for example, delivering an alert about drug-to-drug interactions at the time of prescribing. Other information, such as providing the names of patients being seen on a given day who need immunizations, could occur prior to the patient encounter. Knowing when the information from the CDS should be presented automatically or “on demand”, i.e., when the user chooses to access the information, is no small feat. Tying the answers to the other questions, e.g., whose
- 41. decisions are being supported, can also be complex. 5 Looking further at the challenge of knowing when the information from the CDS should be presented, that is, automatically or “on demand,” another factor that must be considered and presents its own set of challenges is deciding how much control the user has over the decision to use clinical decision support. In other words control over whether users are required to accept the CDS suggestion, whether they can easily ignore it, or whether it takes significant effort to override the advice. Berner (2009) explains, “These decisions involve not only whether the CDS is set up to be displayed on demand, so that users have full control over whether they choose to access it, but also the circumstances under which users can, after viewing the CDS information, choose whether to accept it. The two aspects of control are related and
- 42. they connect with how closely the CDS advice matches a clinician’s intention. CDS may be designed to (1) remind clinicians of things they intend to do, but should not have to remember; (2) provide information when clinicians are unsure what to do; (3) correct errors clinicians have made; or (4) recommend that the clinicians change their plans. Conceived of in this way, it should be obvious that the users’ reactions to CDS may differ with these diverse intents” (p. 7). 6 Building on to the challenges already described, Table 5.1 summarizes three clinical decision support intents and matches each to a user’s intention along with a key issue. The first CDS intent is an automatic intervention – a reminder of actions a user intends to do but should not have to remember. As one would expect, timing is a key issue. Next under CDS intent is an on demand intervention – one that
- 43. provides information when a user is unsure of what to do, or a request for consultation. In this instance, it is speed and ease of access that the user is looking for. According to (Berner, 2009) “Users may recognize the need for information, but may be willing to access it only if they can do so efficiently. If access is too difficult or time-consuming, potential users may choose not to use the CDS” (p. 8). The third row lists the CDS intent as correct user’s errors and/or recommend a user change plans, and could be either an automatic or on-demand intervention. For an automatic intervention, the key issues are timing, autonomy, and user control over the response. For an on demand intervention, they are speed, ease of access, autonomy, and user control over the response. For this CDS intent, users balance the change planned with the desire for autonomy with other demands such as improving patient safety or decreasing practice costs. Another key issue related to autonomy that was previously discussed is the amount of control users have
- 44. over how they respond to the CDS. Berner (2009) goes on to explain, “While some of these issues have been addressed by research, there are no universally accepted guidelines regarding them, in part because clinicians often differ in their preferences. In addition, there are varying clinical approaches that are justified, which makes designing effective CDS a challenge. How these issues are addressed will influence the ultimate impact and effectiveness of CDS” (p. 8). 7 The report, Clinical Decision Support Systems: State of the Art, cited several studies and provided insight into other challenges in the building and using of clinical decision support systems. Discussions were split between the impact on care process and patient health outcomes and the impact on structure. For the first one, impact on care process and patient health outcomes, the three challenges
- 45. identified were matching of clinical decision support to user intentions, user control, disruptiveness, and risk, and integration of CDS into work processes. Each one of these challenges presents issues which need to be addressed when building clinical decision support systems. For example, according to the report, “…integrating CDS into the workflow often requires unique customization to local processes, and sometimes to changes in processes (when previous clinical processes were found to be inefficient or ineffective). CDS also needs to be minimally disruptive to the clinician’s “cognitive workflow” and this, too, can be a challenge. For instance, accessing the data needed for the CDS can be disruptive if the clinical systems are not well integrated or if the necessary data are not in a form that the CDS can use. If the lack of data leads to inappropriate alerts, these alerts may be overridden. In addition, to the extent that using CDS or following its advice is disruptive to the clinician’s work or thought processes, the CDS is likely to be ignored” (Berner, 2009, p.
- 46. 11). Another group of discussion points addressed studies on the structural impact of CDS. The conclusion was “It is important to recognize that the development, implementation, and maintenance of CDS will have an impact on the structure or work system in which it will be used. The changes that the CDS will introduce need to be incorporated in the planning so that the impact on clinician time is not excessive” (Berner, 2009, p. 13) 8 In addition, often IT resources are limited due to implementation of other EHR modules, support of systems already in place, and compliance demands, which causes barriers to CDS deployment. 8 There are six barriers to the effective implementation of CDS. The first three identified are:
- 47. 1. Acquisition and validation of patient data – The issues here are the need to have 1) effective techniques for capturing data accurately, completely, and efficiently and 2) a standardized way to express clinical situations that a computer can interpret Musen et al. (2006). 2. Modeling of medical knowledge – Described by Musen et al. (2006) as “deciding what clinical distinctions and patient data are relevant, identifying the concepts and relationships among concepts that bear on the decision-making task, and ascertaining a problem-solving strategy that can use the relevant clinical knowledge to reach appropriate conclusions” (p. 713). 3. Elicitation of medical knowledge – keeping the knowledge- base up-to-date is portrayed by Musen et al. (2006) as an important problem for CDSS. 9
- 48. The last three barriers to the effective implementation of CDS are: Representation of and reasoning about medical knowledge - Musen et al. (2006) stated “among the ongoing research challenges is the need to refine the computational techniques for encoding the wide range of knowledge used in problem-solving by medical experts” (p. 715). Another part to this is the need to obtain an understanding of the psychology of human problem-solving for use in the development of clinical decision support tools so they more closely reproduce the process by which clinicians move through the diagnostic process (Musen et al. (2006). Validation of system performance – Here Musen et al. (2006) pointed out issues of having a responsible party for validating the clinical knowledge bases and the challenges in determining how best to evaluate the performance of the tools that use the knowledge particularly when a “gold standard” in which to perform the evaluation doesn’t exist.
- 49. Integration of decision-support tools – Musen et al. (2006) state the need for “…more innovative research on how best to tie knowledge-based computer tools to programs designed to store, manipulate, and retrieve patient-specific information” (p. 716). 10 One legal barrier to the implementation of clinical decision support systems is the lack of detailed case laws on issues for dealing with clinical decision support systems and under which category of law the systems will fall. Musen et al. (2006) provide the following explanation regarding this barrier: “Under negligence law (which governs medical malpractice), a product or activity must meet reasonable expectations for safety. The principle of strict liability, on the other hand, states that a product must not be harmful. Because it is unrealistic to require that decision support programs make correct assessments under all circumstances— we do not apply such standards to physicians themselves—the determination of which legal principle to apply will have important
- 50. implications for the dissemination and acceptance of such tools” (p. 731). 11 Another legal barrier described by Musen et al. (2006) is the issue of who will bear the liability. Should it be the physicians or the builders of the systems? Musen et al. (2006) state “A related question is the potential liability borne by physicians who could have accessed such a program, and who chose not to do so, and who made an incorrect decision when the system would have suggested the correct one. As with other medical technologies, precedents suggest that physicians will be liable in such circumstances if the use of consultant programs has become the standard of care in the community” (p. 731). With no case law yet to establish the precedent, recommendations have been for stronger regulation and guidelines. 12
- 51. There are also regulatory barriers that could affect distribution of clinical decision support systems. One identified by Musen et al. (2006) is the validation of decision-support tools before their release and what role the government should play. Where should the government fall with regards to prerelease regulations of medical software? Musen et al. (2006) point out that “Programs that make decisions directly controlling the patient’s treatment (e.g., closed loop systems that administer insulin or that adjust intravenous infusion rates or respirator settings) are viewed as medical devices subject to FDA regulation” (p. 732). However, the IOM report Health IT and Patient Safety: Building Safer Systems for Better Care did not recommend the FDA, ONC, CMS, or AHRQ as the regulatory body to oversee health IT safety but did recommend the creation and funding of a new independent federal agency, similar in structure to the National Transportation Safety Board (IOM, 2012, p. 128). Other barriers include data privacy and security. Identifiable
- 52. data used for research purposes are afforded protections which is one view of what data used for CDS is. Aggregated data can be used without consent, but de-identification and aggregation of clinical data across systems is difficult. While there are challenges and barriers, including legal and regulatory ones, in the building, use, and distribution of clinical decision support systems, their benefits such as avoidance of errors and adverse events, are seen as worth the work involved. A description of the various efforts and initiatives are discussed in the next few slides. 13 Legislative and regulatory efforts needed to support widespread adoption of clinical decision support systems were identified by the AHIC CDS Workgroups. As explained in a letter to Secretary HHS Leavitt the recommendations were as follows (AHIC,
- 53. 2008): 1. Drive measurable progress toward priority performance goals for health care quality improvement through effective use of CDS 2. Explore options to establish or leverage a public-private entity to facilitate collaboration across many CDS development and deployment activities. 3. Accelerate CDS development and adoption though federal government programs and collaborations. One of these recommendations has been implemented as the next few slides will show. 14 There are a number of projects shaping the future directions for clinical decision support systems. These include the Office of the National Coordinator’s initiatives, the Institute of Medicine’s studies, and the meaningful use criteria, objectives and measures. Each will be
- 54. explored in the slides that follow. 15 The Office of the National Coordinator for Health IT (ONC), which is charged with coordinating federal efforts regarding HIT adoption and meaningful use, has stated their commitment and facilitated a number of projects for the purpose of moving CDS development and deployment ahead. The major activities include: The “Advancing CDS” is a project intended to: “Advance the widespread dissemination of successful CDS implementation practices to promote broad CDS adoption Improve the acceptance and usability of medication CDS systems through the development of a clinically important drug-drug interaction list Advance the practical sharing of effective CDS interventions across care settings
- 55. Identify CDS-related gaps and goals specific to a broad range of clinical specialties” (ONC, 2011, para. 3) Another ONC initiative related to CDS includes the report Development of a Roadmap for National Action on Clinical Decision Support that recommended ways to improve CDS development, implementation and use. Three pillars for fully realizing the promise of CDS were identified. They are: 1) Best knowledge available when needed, 2) High adoption and effective use, and 3) Continuous improvement of knowledge and CDS methods (Osheroff, et al., 2006, p.5). Other projects include the development of CDS recommendations by the AHIC workgroups mentioned previously, an ONC-sponsored Clinical Decision Support (CDS) Workshop, and the CDS Federal Collaboratory. 16
- 56. The final ONC initiative is an Institute of Medicine study carried out under a $989,000 contract awarded in September 2010. The next slide will provide more information on this work. 16 The Institute of Medicine (IOM) has for many years published key bodies of work. A press release on September 29, 2010 included a quote from Dr. David Blumenthal who at the time was national coordinator for health information technology which explained IOM’s role “Since 1999, when the IOM published its ground-breaking study To Err Is Human, the Institute has been a leader in the movement to improve patient safety” (CMS, 2010). The To Err is Human report emphasized “…mistakes can best be prevented by designing the health system at all levels to make it safer--to make it harder for people to do something wrong and easier for them to do it right” (National Academy of
- 57. Sciences, 2000). The IOM study launched in 2010 was aimed at examining a comprehensive range of patient safety-related issues, including prevention of HIT-related errors and rapid reporting of any HIT- related patient safety issues. IOM saw its charge as “recommending ways to make patient care safer using health IT so that the nation will be in a better position to realize its potential benefits” (National Academy of Sciences, 2011). As mentioned previously, one of the recommendations was the creation and funding of a new independent federal entity that would have the responsibility to oversee health IT safety. Another recommendation was funding a new Health IT Safety Council to set standards for safety. 17 The final endeavor having an impact on future directions for CDSS is the American Recovery and Reinvestment Act or ARRA and the associated Health Information Technology for Economic
- 58. and Clinical Health (HITECH) provision. ARRA, officially Public Law 111-5 signed into law February 2009, provides many different stimulus opportunities, one of which is $19.2 billion for health IT. HITECH is a provision of the American Recovery and Reinvestment Act. The HITECH section of ARRA deals with many of the health information communication and technology provisions. It established programs under Medicare and Medicaid to provide incentive payments for the "meaningful use" of certified EHR technology. According to the Centers for Medicare and Medicaid Services (CMS, 2011), “The Medicare and Medicaid EHR Incentive Programs will provide incentive payments to eligible professionals, eligible hospitals and critical access hospitals (CAHs) as they adopt, implement, upgrade or demonstrate meaningful use of certified EHR technology” (para. 1). On July 13, 2010, the Secretary of HHS published in the Federal Register a final rule that adopted standards, implementation specifications, and certification criteria for HIT. The final rule
- 59. was released in conjunction with the Medicare and Medicaid EHR Incentive Programs final rule. The CMS regulations specify the objectives that providers must achieve in payment years 2011 and 2012 to qualify for incentive payments. The ONC regulations specify the technical capabilities that EHR technology must have to be certified and to support providers in achieving the “meaningful use” objectives. Following are meaningful use requirements that must be met to qualify for incentive payments (CMS, 2010, p. 44350): • For the eligible professional: Implement one clinical decision support rule relevant to specialty or high clinical priority along with the ability to track compliance with that rule. • For the hospital: Implement one clinical decision support rule related to a high priority hospital 18 condition along with the ability to track compliance with that rule
- 60. 18 This concludes Clinical Decision Support Systems. Lecture a defined clinical decision support, described system requirements, and explained the effects of clinical practice guidelines and evidence-based practice on CDSS. Lecture b described challenges and barriers, including legal and regulatory ones, in the building, use, and distribution of clinical decision support systems. To move forward requires further effort. A number of projects shaping the future directions for clinical decision support systems have come to fruition in the last few years, and more initiatives are underway. These include the ONC initiatives and the meaningful use requirements tied to clinical decision support. 19 No audio.
- 61. 20 No audio. 21 Working with Health IT Systems is available under a Creative Commons Attribution-NonCommercial- ShareAlike 3.0 Unported license. © Johns Hopkins University. UMUC has modified this work and it is available under the original license. http://knowledge.amia.org/onc-ntdc/working-with-health-it- systems-1.379705 https://creativecommons.org/licenses/by-nc-sa/3.0/us/ https://creativecommons.org/licenses/by-nc-sa/3.0/us/ Welcome to Quality Improvement: Decision Support for Quality Improvement. This is Lecture a. This unit is designed to provide information on Clinical Decision Support as it is used to enhance patient care quality and safety. 1
- 62. The Objectives for Decision Support for Quality Improvement are to: •Define decision support, its importance, and why it is difficult to implement. •Compare decision support tools that help improve quality. 2 According to Healthcare Information and Management Systems Society (HIMSS), “Clinical Decision Support is a process for enhancing health- related decisions and actions with pertinent, organized clinical knowledge and patient information to improve health and healthcare delivery. Information recipients can include patients, clinicians and others involved in patient care delivery; information delivered can include general clinical knowledge and guidance, intelligently processed patient data, or a mixture of both; and information delivery formats can be drawn from a rich palette of options that includes data and order entry facilitators, filtered data
- 63. displays, reference information, alerts, and others.” Clinical Decision Support Systems (CDSS) are typically designed to integrate a medical-knowledge base, patient data, and an inference engine to generate care- specific advice. These systems are designed to help healthcare providers make decisions at the point of care. This unit will present examples of Clinical Decision Support (CDS) and more complex decision support systems. CDS can occur without a complex system to support it and should be pervasive in HIT systems. It is also important to consider that CDS systems are support tools and must be surrounded by a strategy and an overall aim. Whether you choose CDS or CDSS they will be of no use unless you have an overarching goal for their implementation. 3 Here are some examples of how the CDS can help improve the
- 64. care of patients. Hospital example: a physician is writing an order for an antibiotic that has to be dosed depending on the kidney function. When he adds the antibiotic at its full dose, the computer will prompt him to reconsider the dose based on the latest creatinin (a blood test of kidney function) and pulls up a dose calculator. Primary-care example: a medical assistant is rooming a patient and reviews a reminder that informs her that the patient is due for a PAP and a mammogram. She tells the patient and they decide she would like to have it today. By the time the clinician walks in, the patient is undressed and ready for the PAP, the mammogram order papers are ready, and the patient has been informed about how to perform her breast self-exam. As you can see, CDS systems are important tools for increasing the safety and efficiency of the health care system. 4
- 65. The CDS Five Rights model states that we can achieve CDS- supported improvements in desired healthcare outcomes if we communicate following these five premises: •The information has to be evidence based, pertinent, and actionable. There is no point to adding information if you cannot do anything about it. •There is a tendency to have the clinician be the recipient of all information. As teams organize around the patient-centered care model, one should consider which member of the team is the appropriate recipient. •CDS can be administered in many different formats. Consider the use of alerts, order sets, or reference information as different CDS formats. Each has a role in the development of an institutional strategy. •The delivery channel is also an important component of the CDS design. A delivery model example could include a PHR (personal health record) a
- 66. mobile device, an EHR (Electronic Health Record) or a more general channel such as the Internet. •The final component of a sound CDS strategy is the time when the information is delivered. When are the decisions made and when are actions taken? 5 There are a number of CDS systems, including relevant data displays, smart documentation forms, order facilitators such as smart order sets, consequents and modifiers, extended-time guidelines and protocols, targeted reference, such as contextually relevant medical references or information buttons, reactive alerts and so on. 6 Other CDS systems include task assistants for tasks such as drug dosing and
- 67. acknowledging laboratory results, diagnostic suggestions, patient summaries for hand-offs between clinicians, procedure refreshers, training, and reminders; performance dashboards with prompts for areas needing attention; and tracking and management systems that facilitate task prioritization and whole-service management. 7 Let’s review some of the research that supports the effectiveness of CDSS. Kuperman and his research team report that clinical decision support systems, when combined with CPOE, have the potential to improve medication safety and reduce medication-related expenditures. In addition to the obvious benefits of increasing legibility of orders, these systems introduce automation at the time the prescriber places an order. Decision support can also assist to ensure the safety of
- 68. the order as well as compliance with clinical practice guidelines. An example is provided by Seidling and colleagues, who developed a comprehensive algorithm that pulled relevant patient data—such as age and renal function—and adjusted upper dose limits for these patient characteristics. They have been able to decrease prescription of excessive medication doses using this type of decision support. 8 Despite the potential usefulness of decision support systems, there is concern over the lack of widespread clinical acceptance by clinicians. In the early development of clinical decision support systems, there were three basic assumptions, which strongly influenced the development of these systems. These assumptions have been challenged and are now seen as myths. The first myth is that diagnosis is the
- 69. dominant decision-making issue in medicine. In reality, clinicians usually ask “what can I do for this patient?” rather than “what does this patient have?” The second myth is that clinicians will use knowledge- based systems if the programs can be shown to function at the level of experts. We know that there is significant variation in practice, even among experts. The final myth is that clinicians will use stand- alone decision support tools. We know now that we need to integrate decision support into the context of routine clinical workflow. 9 Four key functions of electronic Clinical Decision Support Systems have been identified. These include: administrative, managing clinical complexity and details, cost control, and decision support. 10
- 70. Decision support has the potential to be helpful to support clinical coding. In addition to assisting with authorization of procedures and referrals, decision support can assist in selection of appropriate diagnostic codes for billing purposes. Coding accuracy, that is, the extent to which the code accurately reflects the underlying patient’s disease, directly affects the quality of billing decisions. The quote on the slide from Peters illustrates this point. Since coding is based on clinical documentation, with the advent of electronic-health records, administrators are looking for opportunities to capture accurate billing information from the data documented by clinicians, especially documentation of coded problem lists and data contained in history and progress notes. Other researchers are investigating the use of decision-support tools that employ algorithms based on clinical data in the EHR, to display a proposed list of coded diagnoses to guide prescribers to make the most appropriate
- 71. selections. 11 Decision support is used to manage the complexity of the clinical environment, especially in academic medical centers. Academic medical centers have a combined clinical and research mission and very complex business operations. With respect to clinical research, alerts can be established to assist with the recruitment efforts of clinical researchers by identifying eligible research participants based on inclusion and exclusion criteria. Clinical Decision Support is also used to manage follow-up of multiple referrals and tracking of orders. Clinical guidelines and outcomes related to preventive care and treatment of patients with chronic disease is another area in which investigators are studying the effectiveness of clinical decision support. 12
- 72. Decision support can be used to help control the costs of care. By monitoring prescribing practices with respect to high cost medication orders, alerts can be generated to suggest lower cost alternatives. When institutions place restrictions on prescribing high cost drugs, decision rules can ensure that indications for use are present. Duplicate or unnecessary laboratory and radiologic testing can be avoided by applying decision rules that warn the prescriber that the test has already been ordered, or that the test is inappropriate for the particular patient. 13 General decision support functions promote use of best practices and facilitate evidence-based population management. For example, rules- based logic can scan available patient information and flag patients who are not in compliance with
- 73. wellness or disease management regimens and alert the provider or the patient that interventions are due. Formulas and algorithms can present relevant patient data and perform complex calculations that the providers used to have to perform by hand. Important patient information can be tracked in disease registries. For example, diabetes-disease registries may include pertinent laboratory tests, dates of last foot and eye exams, and due dates for next services. Summary screens, usually the first to appear when the electronic record is opened, display patient problems, medications, recent laboratory test results, and other pertinent clinical information in a, “patient-at-a-glance,” display. These summary screens serve as reminders for the patient’s care team about chronic issues to factor into decisions as well as for covering providers who may have gaps in knowledge about the patient. Clinical situations can also be addressed as preassembled order sets for
- 74. typical clinical scenarios. For example, annual physical examinations for females over age 45 may aid the provider to order the appropriate preventive tests as needed. 14 Researchers have looked at unintended consequences related to Clinical Decision Support. These consequences can be categorized into consequences related to content and presentation. There are three themes related to content. The first is elimination or changing of roles of clinicians and staff, especially clerical staff. For example, one case study noted that clinicians underestimated the gatekeeper function of the clerical staff, who in the paper world, questioned daily X-ray orders after a certain amount of time, but once they automated this function, chest X-ray orders went on ad infinitum. A second unintended consequence related to currency
- 75. of Clinical Decision Support content. For example, changes in coding for billing or compliance and difficulties updating order sets may cause problems. Another content-related consequence is wrong or misleading clinical decision support content. An example of this would be a clinical decision support rule that leads clinicians to order something that is not adequately stocked. Another example is when contradictory advice is offered by two separate clinical decision support rules. The second category of unintended consequences is presentation. This category includes rigidity of systems, alert fatigue, and other sources of potential error. For example, the way in which workflow is changed by the insertion of the computer into the clinical workspace represents a presentation consequence. Alert fatigue is so great a problem that there is an entire unit devoted to that issue. Other sources of potential error include such things as the auto-complete feature that may insert the
- 76. wrong medication or alerts that are seen when it is too late for action. 15 This concludes Lecture a of Decision Support for Quality Improvement. In summary, Clinical Decision Support Systems are usually designed to integrate a medical knowledge base, patient data, and an inference engine to generate care- specific advice. Despite the potential usefulness of Clinical Decision Support, its use has not led to widespread adoption. In planning to implement Clinical Decision Support, IT professionals need to know that it will be used by clinicians and that its use will alter clinical decision-making, change behaviors, and improve patient outcomes. Four key functions of Clinical Decision Support are: administrative, managing clinical complexity and details, cost control, and decision support. 16
- 77. No audio. 17 No audio. 18 Working with Health IT Systems is available under a Creative Commons Attribution-NonCommercial- ShareAlike 3.0 Unported license. © Johns Hopkins University. UMUC has modified this work and it is available under the original license. http://knowledge.amia.org/onc-ntdc/working-with-health-it- systems-1.379705 https://creativecommons.org/licenses/by-nc-sa/3.0/us/ https://creativecommons.org/licenses/by-nc-sa/3.0/us/ Welcome to The Culture of Healthcare: Privacy, Confidentiality, and Security. This is Lecture (a). The component, The Culture of Healthcare, addresses job expectations in healthcare settings. It discusses how care is organized within a practice setting, privacy laws, and professional and ethical issues encountered in the workplace.
- 78. 1 The objectives for Privacy, Confidentiality, and Security are to: • Define and discern the differences between privacy, confidentiality, and security • Discuss the major methods for protecting privacy and confidentiality, including through the use of information technology • Describe and apply privacy, confidentiality, and security under the tenets of HIPAA Privacy Rule • Describe and apply privacy, confidentiality, and security under the tenets of the HIPAA Security Rule 2 This unit defines these important terms and discusses reasons for concerns about privacy and security related to health information. Tools for protecting health information will be examined, followed by a discussion of the Health Insurance Portability and Accountability Act, or HIPAA [hip-uh] regulations and what additions have been made in the HITECH [high-tehk]
- 79. (Health Information Technology for Economic and Clinical Health Act) legislation. 3 This lecture discusses Privacy and Security. Privacy is one’s right to keep information to one’s self. It is the right to be left alone, the right to keep personal information secret, and in essence, the right to control personal information. Confidentiality, on the other hand, is one’s right to keep information about one’s self from being disclosed to other people. When a patient vests confidentiality in a physician and a healthcare system, it is expected that personal information is kept confidential and not disclosed to others. Data is only shared or disseminated to those with a “need to know.” Security is the activity of protecting personal information. It consists of mechanisms to assure the safety of data and the systems in which the data reside. 4
- 80. Individually identifiable health information, or IIHI [eye-eye-H- eye] is any data that can be correlated with an individual, for example information in a medical record or a database that can be linked up to an individual. A related term is personal health information. This is individually identifiable health information as defined explicitly by the HIPAA [hip-uh] privacy rule in the US. Finally, consent is actually a broader term but it will be defined here in the context of privacy. When consent is given to the healthcare system, it entails written or verbal permission to allow use of individually identifiable health information for the activity of providing healthcare or for participation in a research project or related activity. 5 The remainder of this lecture focuses on concerns about privacy and security beginning with concerns about privacy followed by the notion of personal privacy versus the common good. The discussion continues with disclosures of personal health information, examining some of the concerns that the public has
- 81. about the privacy of health information. Finally, the lecture will close with a few comments about de-identified data. 6 Consider the notion of personal privacy versus the common good. Some of the concerns are well demonstrated in a video that was produced in 2004 by the American Civil Liberties Union, to which a link is provided. In this video, a pizza restaurant has access to customer’s medical information and they penalize them for things like ordering extra cheese when their cholesterol levels are shown to be high. It is a video worth watching, even though it takes a very specific point of view. There is a broad spectrum of views here, often times reflecting underlying political beliefs. At one end of the spectrum is the view that while personal privacy is important, there are some instances when the common good of society outweighs personal privacy. An example that is often given is biosurveillance [buy-oh-sur-vay-lehns], whether it is monitoring emerging natural diseases or things like
- 82. bioterrorism. Early intervention and response is possible with more information. Another example is clinical research. When more clinical research is conducted, the ability to provide quality healthcare is increased. The other end of the spectrum holds that personal privacy trumps everything, that there should really be no reason to violate one's privacy without explicit consent. Some of the organizations that are prominent in promoting this point of view include the Privacy Rights Clearinghouse that has written specifically about medical information even though they typically deal with broader privacy rights topics. Another group is called patientprivacyrights.org, and is headed by Dr. Deborah Peel, a Texas 7 psychiatrist who is very well known and outspoken on personal privacy. Others have called for a more balanced approach between personal privacy and the common good. For more information on this topic,
- 83. some good articulations of this can be found in documents from the California Healthcare Foundation, an editorial by Dr. Don Detmer, and a policy paper from the American College of Physicians.As with many ethical issues, there are no explicitly right or wrong answers, and each individual has to decide where their views fall on the spectrum; however the US political process, not the individual, will more than likely determine how personal privacy and common good in terms of healthcare are balanced. 7 It is important to know about patient information disclosure and how to prevent it from happening in the future. One particularly egregious [ih-gree-juhs] story happened in Portland, Oregon on New Year's Eve, 2005. On that date, an individual left in his car a number of disks, backup tapes, and other media that contained the records of about 365,000 patients who were seen by a visiting nurse association. This naturally received a lot of press and demonstrated the need to be careful and not, for example, leave items in your car, especially if they contain personal health information.
- 84. The Veterans Administration system has had a number of episodes, probably the largest of which was when a laptop with the data of over a million veterans was stolen. The laptop was recovered and it appeared that the data was not accessed, but of course, no one knows exactly what went on with the machine when it was in the hands of those who stole it. More recent data shows that disclosures continue to be a problem. Two Web sites are devoted to ongoing documentation of the problem. The Privacy Rights Clearinghouse provides a searchable Chronology of Data Breaches. The data includes medical breaches but is not limited to them. The site can be linked to from http://www.privacyrights.org/data-breach. The Department of Health and Human Services (HHS, aych- aych-ess) is now required under the HITECH Act to post a list of breaches of unsecured protected health information affecting 500 or more individuals. It is called by some their “wall of shame.” It can be accessed at http://www.hhs.gov/ocr/privacy/hipaa/administrative/breachnoti ficationrule/breachtool.html.
- 85. 8 By end of 2011, this site had documented 380 incidents affecting 18,059,831 individuals. 8 The Ponemon [pone-eh-mon] Institute publishes an annual report on the impact of security breaches on healthcare organizations. The 2011 report found that the number of breaches increased by 32% over 2010. It also found that the average cost per breach to an organization was $2.2 million and took one to sixth months to resolve. A significant part of cost was “lost business” by the organization. About 41% of the breaches were discovered as a result of a patient complaint. The top causes of data breaches were unintentional employee action, lost or stolen computing devices, or third-party problems. Of note, most organizations believe their EHR makes data more secure. 9
- 86. There are newer challenges from the proliferation of health IT technologies and applications. For example, there is an ever- growing use of electronic data in clinical workflows. Likewise, health information exchange (HIE) moves data across networks and cloud computing alters the perimeter of data protection. There are also new models of healthcare, such as accountable care organizations (ACOs, ay-see-ohs) that require more members of a team to access information. Finally, clinicians want to increasingly use their own devices, such as personal laptops, tablet devices, smartphones, and so forth. 10 And, of course, technology itself can worsen the problem. A widely cited study by Wright looked at the USB drives commonly plugged into computers (sometimes called thumb drives). These drives run a program that enables their use when they are plugged in, and that program can be modified to extract data from the computer. So if that computer has personal health information on it, the thumb drive can basically copy it off the computer.
- 87. There are many people who have developed personal health record systems based on tools like Microsoft Access, which has some encryption functionality, but is very easily compromised. Another interesting analysis found that ten percent of hard drives sold by second-hand retailers in Canada had remnants of personal health information (PHI) on them. Often when computers are disposed of, the hard drives are not completely wiped clean, potentially providing access to personal information to the next user, if they know how to extract it. Also of note is that PHI can be discovered by files available from peer-to-peer (P2P, pee-two-pee) file-sharing networks. One analysis found that half of one percent of all IP addresses on the Internet in the US have discoverable PHI. Finally, another technology that can store PHI is the digital photocopier, which stores all copies on an internal hard disk. If this information is compromised, PHI can potentially be leaked. 11
- 88. Two analyses have shown that healthcare organizations are not well-prepared for security challenges. A report by Deloitte [deh-loyt], the consulting firm, looked at security issues in healthcare organizations and came to the following conclusions: The primary threat to information is data leakage, or data that gets out in the routine care of patients. The report also concluded that identity and access management is a top priority. The trend towards outsourcing of IT in healthcare organizations raises many third-party security concerns. The role of the chief information security officer or chief security officer in most healthcare organizations, particularly large ones, then takes on greater significance. Every decision about information systems needs to be assessed from the standpoint of security. This report also found that despite the increasing complexity of the security environment and the growing number of regulations, the budgets of financially strapped healthcare organizations were not keeping pace with security needs. The annual security readiness survey by HIMSS [himz] Analytics reached roughly the same conclusions: healthcare
- 89. organizations, in general, are not keeping pace with security threats and readiness. This analysis found, for example, that 85% of organizations share electronic data but only 61% perform a risk analysis annually or more frequently. 12 One question to ask is, “What is the role of government in protecting privacy and confidentiality?” This discussion will begin by looking at the US and then move to other countries. In the US, the National Center for Vital & Health Statistics, or NCVHS [N-C-V-H-S], has weighed in over the years on a number of privacy and security issues. In 2006, it released a set of twenty-six recommendations for policies concerning health privacy for the Nationwide Health Information Network. Further recommendations have been released for personal control of health information, and again called for a consistent and coherent policy.
- 90. Another activity has been the HISPC [hisp-see] effort, the health information security and privacy collaboration, a project funded by the government that looked at forty-two states and territories and assessed the various approaches and laws to privacy. A wide range of privacy policies were found and it was concluded that a nationwide approach would be difficult due to the sometimes conflicting laws. There probably needs to be more harmonization of privacy laws as more health information exchanges that move personal health information across state lines are developed. More recently, the Office of the National Coordinator for Health Information Technology (ONC) has established a Privacy & Security Tiger Team charged withdeveloping policies and vetting them with other ONC policy and standards committees. 13 The US is not the only government that has been addressing privacy. In fact, the European Commission has devoted even more efforts to the protection of individual privacy. The directive, 95/46/EC, is a set of fairly stringent rules that essentially
- 91. allows data processing only with consent or in some highly specific circumstances, such as a legal obligation, or what is defined as a public necessity, usually revolving around public health. The countries that implement this directive provide examples of how “consent” around information could be used for efforts in the US in the Nationwide Health Information Network. 14 There are a number of related issues for medical privacy. One of these issues, and again, there is no right or wrong answer,, is who owns medical information. As the articles by Hall and Rodwin point out, historically the owner of the information medium was considered to be the owner of the information. For example, if an office practice or hospital had paper charts, and had bought and owned the paper the charts were printed on, it was presumed that the practice or hospital owned the information on that paper. However, in the electronic era, information moves freely across networks from one system to another, and ownership of that information becomes less clear - in fact, a growing view is that the patient owns their own information.
- 92. As the amount of information increases, there is an increased economic value to health systems, pharmaceutical companies, and others who may want to use that data for various purposes. The article by Rodwin, in particular, argues that when there is an economic advantage gained by the use of that information, then at least some of that gain should be shared back to the patient. Another concern is compelled disclosures of information, that is, even though laws and regulations may highly protect information, individuals may sometimes be compelled to disclose information for nonclinical care reasons in the healthcare setting. Healthcare providers need to be aware of requiring individuals to disclose information that is not really being used for 15 health-related activities. Another growing issue concerns the human genome, which may be a person’s ultimate personal identifier. A person’s genome is what
- 93. makes them an individual. Individual genes and the variation that they have from others’ genes, are unequivocally unique to each person. Health information can be de-identified, but with genomic information, individuals may be easily identifiable. Access to the genomic information manifests itself in a number of ways. For example, a person's genome [jee-nohm] can be identified by the genomic [ ji-noh-mik] information in their siblings. There are a growing number of genome wide association studies where an attempt is made to associate variation in an individual’s genome [jee-nohm] with different diseases. There is actually a requirement for researchers to put this data in public databanks, although usually the individual personal information is protected, with the exception of the researchers who can legitimately get to that information. It is not too difficult to identify who the individual is from that data, so as research moves forward with genomics [ ji-noh-miks] and personalized medicine, more privacy issues will come to the fore. 15
- 94. Another number of organizations have tried to define health information rights. One example is the Declaration of Health Data Rights, which comes from a group of mostly personal health record (PHR, pee-aych-are) vendors, accessible at HealthDataRights.org. This group advocates that individuals should all have the right to their own health data. Theyshould also have the right to know the source of each health data element. In addition, individuals should have the right to take possession of a complete copy of their individual health data, without delay, at minimal or no cost. If data exists in computable form, it must be made available in that form. Finally, individuals should have the right to share their health data with others as they see fit. The American Health Information Management Association (AHIMA, a-hee-mah) also has a Health Information Bill of Rights that is slightly more detailed but has similar provisions. 16 When data is referred to as being de-identified, this refers to the removal of personally identifying characteristics of the data,
- 95. such as name or address, or other fields that make up personal health information. Is de-identified secure? It may not always be as secure as intended. One researcher, Dr. LaTonya Sweeney, brought this to light and has received notice in the popular press is. When she was completing her PhD at MIT, she did a widely cited study that essentially identified William Weld, the Governor of Massachusetts at the time, from information found by linking up to publicly available data sources. Her research also showed that eighty- seven percent of the US population could be uniquely identified by their five-digit ZIP code, gender, and date of birth. So when relatively common data elements are combined, individual identities may be easily identified. In the case of William Weld, Dr. Sweeney was able to access a health insurance database for state employees, and Governor Weld was obviously a state employee, and she was also able to purchase the voter registration list for the city of Cambridge, Massachusetts, where he lived. She then combined these two databases, linking up the ZIP code, gender, and date of birth, and was able to identify the Governor, as will be demonstrated further in the next slide.
- 96. While it has been found that genomic data that can be generated in clinical research studies, some recent research has shown how Social Security numbers of individuals can be predicted from public data because so many data sets have Social Security 17 numbers. 17 This slide demonstrates how Governor Weld was identified. On the left is the so-called de-identified state employee health database, which included state employees’ ethnicity, visits to healthcare providers, diagnosis, procedures, medications, and charges. It also contained ZIP codes, dates of birth, and gender. The Cambridge voter registration database included name, address, registered party affiliation, and the same ZIP codes, date of births, and gender. Governor Weld was one of those eighty-seven percent who had a unique combination of ZIP code, date of birth, and gender. So Dr. Sweeney was able to take Weld’s voter registration information and then access his entire
- 97. medical information; this was picked up by the national media and at the time caused quite a stir. 18 This concludes Lecture (a) of Privacy, Confidentiality, and Security. In summary, it is important to distinguish between privacy, which is the right to keep information to one’s self, from confidentiality, which is the right to keep information about one’s self from being disclosed to others. For many reasons, breaches and disclosures of patient information are increasing. In addition, the concept of “de-identified” information is not necessarily as secure as originally thought. 19 References slide. No audio. 20 References slide. No audio.
- 98. 21 References slide. No audio. 22 Working with Health IT Systems is available under a Creative Commons Attribution-NonCommercial- ShareAlike 3.0 Unported license. © Johns Hopkins University. UMUC has modified this work and it is available under the original license. http://knowledge.amia.org/onc-ntdc/working-with-health-it- systems-1.379705 https://creativecommons.org/licenses/by-nc-sa/3.0/us/ https://creativecommons.org/licenses/by-nc-sa/3.0/us/ Welcome to The Culture of Healthcare: Privacy, Confidentiality, and Security. This is Lecture (b). The component, The Culture of Healthcare, addresses job expectations in healthcare settings. It discusses how care is organized within a practice setting, privacy laws, and professional and ethical issues encountered in the workplace. 1
- 99. The Objectives of Privacy, Confidentiality, and Security are to: • Define and discern the differences between privacy, confidentiality, and security • Discuss the major methods for protecting privacy and confidentiality, including through the use of information technology • Describe and apply privacy, confidentiality, and security under the tenets of HIPAA Privacy Rule • Describe and apply privacy, confidentiality, and security under the tenets of the HIPAA Security Rule 2 This lecture discusses concerns that people have about the security of health information. One of the ways to protect privacy is to make information more secure. A comprehensive overview is the recent book, Information Security in Healthcare - Managing Risk, by Herzig. So what concerns do people have about security? The following slides will look at the many points of leakage in the system, some of the consequences of poor security and the related topic of medical identity theft.. It is important to remember that
- 100. security is not unique to electronic systems – it is also an issuefor paper systems. . 3 As anyone who works in a healthcare setting knows, there are many points where information can leak out of the system. This figure, adapted from Rindfleisch [rihnd-flahysh], shows how information flows through the healthcare system. Information is first generated in the provision of patient care by healthcare providers and clinics and hospitals. It then then flows to healthcare support activity, such as payers of healthcare, the insurance companies that reimburse, quality reviews thatmeasure the quality of care delivered, and other types of administration. There are also what Rindfleisch [rihnd-flahysh] describes as social uses of information, everything from insurance eligibility to reporting to public health authorities and using data in medical research - although it is regulated now by the Health Insurance Portability and Accountability Act (HIPAA) more so than when this figure was published. There are also commercial uses of information, things like marketing, participating in managed care
- 101. organizations that may use data for various purposes to try to improve the quality or efficiency of the care they deliver, and the monitoring of drug usage. There are many points along the way where information can leak out of the system. 4 It is important to note that even though the concerns about privacy and security are heightened with electronic systems, paper records have their own set of privacy and security problems. In fact, some have argued that they may be more prone to breaches of security and disclosure. Unlike electronic systems, it is very difficult to audit the trail of a paper chart. It is not clear exactly where the chart goes and who has looked at it - unlike most electronic systems that record which login has looked at a particular piece of information. There are also issues with fax machines. Even in this electronic era, many still rely on fax machines to move information. When the paper comes out of fax machines and is put into a basket, anyone can view this document and where this information goes is not always known.
- 102. Records also continue to be photocopied. We photocopy for many reasons: the patient goes to a new provider, the insurance company needs to have documentation that a specific procedure was done or referral was made, and records get abstracted by individual people. Whether they are paper or electronic, records are also copied for research or quality assurance purposes. Most healthcare insurers belong to something called the Health Information Bureau, which monitors for insurance fraud. It has developed a huge database of individuals’ healthcare claims, looking very properly for health insurance fraud, but also collecting quite a bit of information on individuals’ personal health. 5 Aware of the consequences of poor security, Rindflesich [rihnd- flahysh] pointed out in the late 1990s that patients do various things to protect their security. They avoid seeking healthcare. They lie so things will not end up in their charts. Healthcare providers also have concerns about security, so they may avoid entering sensitive data that could be important in the care of a patient by others and they may also devise workarounds to entering that information.
- 103. A California Healthcare Foundation survey of healthcare consumers found that thirteen percent engaged in activity that the foundation termed privacy-protective - activities that might put their health at risk, such as asking a doctor to leave out a diagnosis, perhaps to prevent someone from knowing that they have a certain diagnosis. Some also pay for tests out-of-pocket because they do not want to submit an insurance claim, knowing that when a claim is submitted, the insurance company then knows that the test was done. Others avoid seeing their regular doctor for some problems because they are trying to protect their privacy over some piece of information. 6 A final security concern is medical identity theft. This is a growing concern, especially as more information is available electronically. With medical identity theft, the thief is using individually identifiable health information for obtaining access to property or services. When this happens, the victims are not only individuals whose medical records have been compromised,
- 104. but also health providers, health plans, and society at large that pays for healthcare, resulting in many victims. The American Health Information Management Association (AHIMA [uh-hee- muh]) has determined that the value of medical identity information is much higher than the information accessed through identity theft, like a Social Security number. The Department of Health and Human Services has also addressed this problem and has developed a report that outlines various approaches to prevention, detection, and remediation of medical identity theft. 7 The next slides will discuss tools for protecting health information. A good source to begin with is the Institute of Medicine (IOM) report that addresses issues of protecting electronic health information, entitled For the Record. It was commissioned by the National Library of Medicine and informed theHIPAA [hip-uh] legislation. It also made recommendations on immediate and future best practices. While some of the content in the book is dated, the framework provides a good way of thinking about the problem.
- 105. 8 There are many different threats to security. There are insider threats which may be accidental disclosure or the curiosity of individuals working in an institution, or insubordination, where a disgruntled or dissatisfied employee accesses information inappropriately. The latter is probably the major cause of security breaches. There are certainly secondary settings. There are also threats that come from outside the institution, such as a hacker that accesses information over the Internet. This type of threat to security has received a lot of press but there are actually relatively few examples. It is really insider threats that have proven to be more problematic. 9 There are a variety of technologies that can be used to secure information. There are deterrents, which do not exclude people from breaching security, but give them pause for doing so, such as putting up alerts when, for example, an employee’s medical record is about to be accessed. Another deterrent is the audit
- 106. trail. There are also system management precautions that can be taken. It turns out that a number of software systems do not protect information as well as they should, and there should be some kind of analysis of vulnerability. Here are some obstacles that can prevent individuals from getting to private information: • Authentication – such as having to use a password or other authentication • Authorization – where individuals have to be authorized to look at certain information • Integrity management – where the integrity of the overall system is assessed and maintained • Digital signatures – requiring a password or other type of digital process to ensure that an individual who is entering data is truly that individual • Encryption – which will be covered in the next two slides • Firewalls – that keep systems inaccessible from, say, the Internet • Rights management – such as restricting who can look at what aspects of different records
- 107. 10 The next slides will discuss encryption. While encryption is necessary, it is not sufficient to ensure security. Any medical communication, whether it is an e-mail or transmission of the medical record, should be encrypted over a public network, because anyone with the right know-how, could intercept that information. What actually is encryption? In essence, it is when information is scrambled using a key and then that key has to be used to unscramble it. There are different types of encryption. So-called symmetric encryption is when information is scrambled and unscrambled with the same key. Asymmetric encryption,sometimes called public-key encryption, is where there is a different key for scrambling than for unscrambling the information. 11 There are a number of important standards related to encryption and other functions that are listed on this slide. Not everyone in the informatics field needs to become an expert, but it is important to know what these standards are in different roles,
- 108. for example, how they will be mandated in the Health Insurance Portability and Accountability Act, HITECH [high-tech], criteria for the meaningful use of electronic health records. First, there is the encryption standard itself, the advanced encryption standard or AES [ay-ee-ess] that has been designated by the National Institute for Standards and Technology or NIST [nihst] as the standard for robust enough encryption and decryption to be used in computer systems for securing information such as health information. Of course information is not just encrypted and decrypted on individual machines; it moves across networks, so the movement of data from point to point also requires a process that not only encrypts the data, but make sure that it stays secure as it moves across those connections. The emerging standard is transport layer security, or TLS, which succeeds a standard that was a very prominent route in the early days of the World Wide Web, the secure sockets layer, or SSL. Of course information moves according to a protocol, such as IP [ei-pee], so there is an Internet Protocol Security, or
- 109. IPsec [ei-pee-sec]. This is part of the IP Internet protocol communications process that was developed for the new version of IP, version 6, but it has actually been pulled from that version and added to version 4, which is what most people use when they connect to the Internet. 12 In addition to making sure information is secure from one point to another across the network, the system needs to ensurethe integrity of the information - that it has not been altered, either due to transmission errors, or for malicious reasons where someone alters the information in transit. The secure hash algorithms, or SHA [ess-aych-ay], ensure the integrity of transmitted information documents. The original protocol was SHA [ess-aych-ay], but it was found to have some security flaws, so SHA-2 [ess-aych-ay-two] has emerged now and is the more robust way of ensuring the integrity of transmitting information across networks. Wikipedia has a nice overview explanation of these standards, as does the NIST [nihst] website, listed on this slide.