8. What is research?
Research is a systematic investigation
of our environments, using a variety of
research tools to develop our knowledge
providing insight on projects.
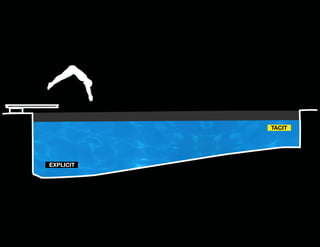
10. How do we “know”?
Tacit Knowledge
In our heads, “gut-feeling”
95%
11. How do we “know”?
Explicit Knowledge
Consciously acknowledged
and organized.
5%
Tacit Knowledge
In our heads, “gut-feeling”
95%
“The value of research is
making the tacit explicit”
SALLY AUGUSTINE (2012)
The Designer’s Guide to Doing Research
13. Environmental Design
Research & Health Timeline
1980s
Roger Ulrich, Pioneering studies on
healing environments
1968
Environmental Design
Research Association
(EDRA) formed
300 BC
Greek Healing
Temples
1986
Carpman & Grant,
Design that Cares
1969
William Whyte, NYC
Behavior Observation
1854
Florence Nightingale,
Crimean War
1973
First Arch. Psych.
course, UK at U.
of Surrey
1993
Center for Health
Design formed
2003
Evidence-based
design (EBD) defined
by Kirk Hamilton
2008
Health Environments
Research & Design
Journal
2001
Institute of Medicine,
Crossing the Quality Chasm
14. Environmental Design
Research & Health Timeline
1980s
Roger Ulrich, Pioneering studies
on healing environments
1968
Environmental Design
Research Association
(EDRA) formed
300 BC
Greek Healing
Temples
1854
Florence Nightingale,
Crimean War
1986
Carpman & Grant,
Design that Cares
1969
William Whyte, NYC
Behavior Observation
1973
First Arch. Psych.
course, UK at U.
of Surrey
1993
Center for Health
Design formed
2003
Evidence-based
design (EBD) defined
by Kirk Hamilton
2008
Health Environments
Research & Design
Journal
2001
Institute of Medicine,
Crossing the Quality Chasm
15. Environmental Design
Research & Health Timeline
1980s
Roger Ulrich, Pioneering studies on
healing environments
1968
Environmental Design
Research Association
(EDRA) formed
300 BC
Greek Healing
Temples
1854
Florence Nightingale,
Crimean War
1986
Carpman & Grant,
Design that Cares
1969
William Whyte, NYC
Behavior Observation
1973
First Arch. Psych.
course, UK at U.
of Surrey
1993
Center for Health
Design formed
2003
Evidence-based
design (EBD) defined
by Kirk Hamilton
2008
Health Environments
Research & Design
Journal
2001
Institute of Medicine,
Crossing the Quality Chasm
16. Environmental Design
Research & Health Timeline
1980s
Roger Ulrich, Pioneering studies on
healing environments
1968
Environmental Design
Research Association
(EDRA) formed
300 BC
Greek Healing
Temples
1854
Florence Nightingale,
Crimean War
1986
Carpman & Grant,
Design that Cares
1969
William Whyte, NYC
Behavior Observation
1973
First Arch. Psych.
course, UK at U.
of Surrey
1993
Center for Health
Design formed
2003
Evidence-based
design (EBD) defined
by Kirk Hamilton
2008
Health Environments
Research & Design
Journal
2001
Institute of Medicine,
Crossing the Quality Chasm
17. HOK Research Services
Primary Research
• Facility Evaluations
• Behavior Observation
• Mock-Ups: Virtual and Physical
Secondary Research
• Literature Review
• Benchmarking
• Guidelines for Hospital System
18. Infusing Research on Projects
Innovation & Validation Process
“If I were given one hour to save
the planet, I would spend 59
minutes defining the problem
and one minute resolving it.”
ALBERT EINSTEIN
Existing
Facility
Assess
Innovate
New
Facility
Validate
20. Shared Goals
Continuum of project types
Broad Review of
Best Practice
Critical Literature
Review
New York
Presbyterian
Mercy Hospital
System
On-site Data
Collection
Mercy Hospital
System
Experimentation
Parkland
Hospital
22. Shared Goals
Institute of Healthcare Improvement’s Triple Aim
The best care
At the
lowest cost
For the whole
population
M. Stiefel & K. Nolan (2012). A Guide to Measuring the Triple Aim: Population Health,
Experience of Care, and Per Capita Cost. IHI Innovation Series white paper. Cambridge,
Massachusetts: Institute for Healthcare Improvement; 2012. (Available on www.IHI.org)
23. Cost & Value
Savings from Research-Informed Design
Essays
“Fewer payers will reimburse hospitals
and physicians for the costs of
preventable harm. Building designs
that help reduce harm are key elements
in a hospital’s survival strategy. ”
Evidence shows that changes in the architecture, design, and decor of health care
facilities can improve patient care and in the long run reduce expenses. These
essays detail the state of the research, look inside two hospitals that put some of
these innovations into practice, and consider how design fits into the moral
mission of health care.
Fable Hospital 2.0:
could return the incremental investment in one year by
reducing operating costs and increasing revenues. Reactions to the Fable paper varied. Many felt it presented
a compelling case and stimulated health care leaders
and architects to think differently about balancing onetime building costs with ongoing operating costs. OthBLAIR L. SADLER, ET AL (2011). Fable Hospital 2.0: The Business
ers voiced skepticism about whether the benefits were as
great as described and asked for more evidence.
Case for Building Better Health Care Facilities. Hastings Center Report
Today, the Fable hospital is no longer imaginary. Dur21, no. 1: 13-23.
ing the past six years, numerous hospitals have implemented many of its attributes and have evaluated their
impact on patients, families, and staff.2 Several are members of the Center for Health Design’s Pebble Project,
a group of organizations that apply evidence-based deBY Bl A I R l . SA d l E R , l E O N ARd l.
signs to improve quality and financial performance. Two
BE R RY, R OBI N GuE NTHE R , d. KIRK
Pebble hospitals are featured in essays accompanying this
H A m I lT ON , F R E d E R ICK A. HE S S l E R,
article. These and other pioneering organizations and
their architecture/design teams are introducing such inC l AYT ON m E R R I T T, AN d dE RE K PARKE R
terventions as larger single-patient rooms, which reduce
espite deep and vocal disagreements over health
the incidence of health care-associated infections; wider
care reform, virtually everyone believes that the
bathroom doors, which reduce patient falls; HEPA filtracurrent system is not economically sustainable.
tion and other indoor air quality improvements, which
Table 3. Improved Outcomes and We are spending too much and getting too little in re- reduce health care-associated infections; appropriate task
Cost Savingshas spurred health care leaders to lighting in medication dispensing areas, which reduces
turn. This recognition
examine every aspect of hospital operations. But what
medication-related errors; hydraulic ceiling lifts in paabout the health care building itself, the physical envitient rooms and bathrooms, which
patient and
We calculated the following savings based on published information. We used our best judgment to attribute a portion of the savings to and art and music, reduce reduce anxironment within which patient care occurs? Too often,
staff lift injuries;
which
cost-cutting discussions have overlooked the hospital
ety and depression and speed recovery.
evidence-based design improvements and attempted to be conservative.
structure. Changes in the physical facility provide real
Since 2004, much has changed that affects decisionopportunities for improving patient and worker safety
making about health care construction and design. It is
and quality while reducing operating costs.
time for a fresh look at the Fable hospital. Drawing on
Improved
Savings or
Calculations
Design Details
The “Fable hospital,” an imaginary amalgam of the
the latest design and health care knowledge, research, the
Outcomes
Increased
best design innovations that had been implemented
2010 health reform law’s emphasis on value and quality
and measured by leading organizations, was an early atimprovement, and our collective experience, we present
Revenue
tempt to analyze the economic impact of designing and
Fable hospital 2.0.
1
building an optimal hospital facility. The Fable analysis,
published in 2004, showed that carefully selected rooms, larger patient
Patient Falls
$1,534,166
300 beds @ 80% occupancy = 240 beds or 87,600 patient days; Acuity-adaptable de- The Changing Health Care Landscape
sign innovations, though they may cost more initially,
Reduced
three falls per 1,000 patient days = 263 falls/year;
bathrooms with double-door access,care trends are relevant to our analyive major health
$17,500/fall = $4,602,500 spent on falls/year. Blair L. Sadler, Leonard L. Berry, Robin Guenther, D. Kirk Hamilton, quality the growth of evidence-based design, the safety/
patient lifts, decentralizedsis: revolution, pay for performance and increasing
nursing
Frederick A. Hessler, Clayton Merritt, and Derek Parker, “Fable Hospital
Incidence of falls ranges from 2.3 to 7/1,000 patient days.Case for Buildingsubstations, family/social spaces
consumer transparency, sustainability and green design,
2.0: The Business
Better Health Care Facilities,” Hastings Center Report 41, no. 1 (2011): 13-23.
and access to capital.
1
The Business Case for
Building Better Health
Care Facilities
D
F
Average cost of patient falls in hospitals is $17,500.
Pebble Partner Clarion Methodist Hospital reduced falls by2011 2
January-February 80%.
Design features help reduce falls by one-third.
Patient
$877,500
25% of 19,500 patient stays are in the ICU/step-down unit.
HASTINGS CENTER REPORT
Acuity-adaptable rooms
13
24. Care Experience
Influencing Experience with Environment
% of Patients Responding
with “5 - Excellent”
“...patients perceived their
overall quality of care as
better in the more attractive
physical environment.”
F. BECKER & S. DOUGLASS (2008). The ecology
of the patient visit: Physical attractiveness,
waiting times, and the perceived quality of care,
J. Ambulatory Care Management, 31(2), 128-141.
38.9%
The care I received
here today was
The service I received
here today was
Overall my interactions
with staff were
Overall, my interactions
with my doctor were
27.8%
70.9%
58.2%
25%
50.9%
61.1%
74.5%
26. System Guidelines
Develop hospital unit
guidelines based on:
‚‚ Research literature
‚‚ Investigation of
existing Mercy
facilities
‚‚ Case studies/
benchmarks of other
existing facilities
27. Customer Experience
Safety
‚‚
‚‚
‚‚
‚‚
‚‚
‚‚
‚‚
‚‚
‚‚
‚‚
Positive distraction & day lighting
Social support & family-centered care
Acoustical privacy & noise reduction
Staff fatigue & satisfaction
Standardization
& Flexibility
‚‚ Spatial flexibility
‚‚ Operational flexibility
‚‚ Room standardization
Unit visibility
Continuum of care post-hospital
Virtual connectivity & care
Infection control
Reduction of toileting-related falls
Reduced staff injury (MSI)
Efficient Operations
‚‚ Eliminated wasted time & travel
‚‚ Point-of-care testing for rapid results
‚‚ Pod-based unit planning to transform
care at bedside
‚‚ Charting location to increase staff at
bedside
28. VA Design Guidelines & Call for Research
POE
Design
Guides
“Potential recommendations
may result in change in policy
and guidelines. ”
Existing
Building
Future
Building
VA Defined Benefits of POE:
• Customer Satisfaction emphasized
• Performance and Facility Functionality
• Standards incorporating Lessons Learned
29. Patient-Aligned Care Team (PACT) Model
DESIGN
How does provider/exam space
configuration impact staff
collaboration, concentration, efficiency
and patient perception of care?
RESEARCH
How can we measure this impact
with minimum disruption to care
and flow of work?
30. Evidence-based Design
The process of basing decisions
about the built environment on
credible research to achieve the
best possible outcomes.
31. Evidence-based Design
The process of basing decisions
about the built environment on
credible research to achieve the
best possible outcomes.
36. Medical Error | Standardization
LIKE-HANDED
PRIVATE ROOM
300 SQ FT
37. Infection | Sink Location
HAND WASHING
SINK AT ENTRY
LIKE-HANDED
PRIVATE ROOM
300 SQ FT
38. Patient Falls | Toilet Location
TOILET LOCATED
ON HEADWALL
HAND WASHING
SINK AT ENTRY
SLIDING
DOOR
IL
PRIVATE ROOM
300 SQ FT
DRA
HAN
LIKE-HANDED
39. Transfers | Variable-acuity Headwall
TOILET LOCATED
ON HEADWALL
HAND WASHING
SINK AT ENTRY
SLIDING
DOOR
IL
PRIVATE ROOM
300 SQ FT
DRA
HAN
LIKE-HANDED
VARIABLE-ACUITY
HEADWALL
40. Staff Efficiency | Nurse Server
NURSE SERVER
TOILET LOCATED
ON HEADWALL
HAND WASHING
SINK AT ENTRY
SLIDING
DOOR
IL
PRIVATE ROOM
300 SQ FT
DRA
HAN
LIKE-HANDED
VARIABLE-ACUITY
HEADWALL
41. Satisfaction | Family Zone
NURSE SERVER
TOILET LOCATED
ON HEADWALL
HAND WASHING
SINK AT ENTRY
SLIDING
DOOR
IL
PRIVATE ROOM
300 SQ FT
DRA
LIKE-HANDED
HAN
WARDROBE
W/ LOCKABLE
STORAGE
VARIABLE-ACUITY
HEADWALL
FLAT
SCREEN TV
FAMILY ZONE
ROOMING-IN
42. Depression, Sleep | Daylight & Views
NURSE SERVER
TOILET LOCATED
ON HEADWALL
HAND WASHING
SINK AT ENTRY
SLIDING
DOOR
IL
PRIVATE ROOM
300 SQ FT
DRA
LIKE-HANDED
HAN
WARDROBE
W/ LOCKABLE
STORAGE
VARIABLE-ACUITY
HEADWALL
FLAT
SCREEN TV
FAMILY ZONE
ROOMING-IN
DAYLIGHT
& VIEWS
44. Access | Unit Design
“Nurses are the primary hospital
caregivers. Increasing the efficiency
and effectiveness of nursing care is
essential to hospital function and
the delivery of safe patient care.”
PATIENT CARE ACTIVITIES
ANN HENDRICH (2008). The ecology of the patient visit:
Physical attractiveness, waiting times, and the perceived quality
of care, J. Ambulatory Care Management, 31(2), 128-141.
19.3%
7.2%
ASSESSMENT / VITALS
35.3%
DOCUMENTATION
20.6%
CARE COORDINATION
17.2%
MEDICATION ADMINISTRATION
58. PETER CAREY (2013). KI & IIDA NY Healthcare Forum: Resilience As
Sustainability. Teknion Office Insights. Issue: 9-30-2013, (3).
59. MYTH 1: Design is only for the carriage trade
FACT: What was once privileged is now common
60. “Globalization 3.0 is shrinking
the world from a size small to
a size tiny and flattening the
playing field at the same time.”
Thomas L. Friedman (2005). The world is flat. New
York: Farrar, Strauss and Giroux.
62. Determinants of Decision Making
values (belief)
ORIENTED TO
THE FUTURE
3
VALUES
DRIVEN
2
GET HERE
GET HERE
innovate
ECONOMY
lag - baseline
DRIVEN
2
1
ORIENTED TO
THE PRESENT
value $$$
63. MYTH: Designers have secret sources
FACT: “To the Trade” is now an open source mouse click away
64. “...translators take ideas and
information from a highly
specialized world and translate
them into a language the rest of us
can understand.”
Malcolm Gladwell (2000) The Tipping Point. Boston:
Little, Brown and Company.
68. MYTH: A four year degree
leads to professionalism
FACT: Requisite for professionalism is
a multi-disciplinary graduate education
69. “But epiphanies rarely occur in familiar surroundings. The key to
seeing like an iconoclast is to look at things you have never seen
before. It seems almost obvious that breakthroughs in perception
do not come from simply staring at an object and thinking harder
about it. Breakthroughs come from a perceptual system that is
confronted with something that it doesn’t know how to interpret.”
Gregory Berns (2008). Iconoclast. Boston: Harvard Business Press.
70.
71. “Opposite of beauty is
injury not ugliness.””
Elaine Scarry (1999). On Beauty
and Being Just. Princeton: Princeton
University Press.
72. MYTH: “Trust me” I have an amazing
portfolio of award winning work
FACT: Time honored traditions need
validation, “Show me results”
73. “Unselfconscious cultures contain, as a feature of their form
producing systems, a certain built-in fixity – patterns of
myth, tradition and taboo which resist willful change. Form
builders will only introduce change under strong compulsion
where there are powerful (and obvious) irritations in the
existing forms which demand correction.”
Christopher Alexander (1964). Notes on the synthesis of form. Cambridge: Harvard University Press.
76. The Future of the Interior Design Profession is on a springboard...
77. The Future of the Interior Design Profession is on a springboard...
Interiors need to be created within an
interdisciplinary team using evidence-based
hypothesized outcome driven solutions for
all who inhabit built environments
78. The Future of the Interior Design Profession is on a springboard...
Interior Designers need to be translators of
productive, safe, resilient environments for
the betterment of mankind
Interiors need to be created within an
interdisciplinary team using evidence-based
hypothesized outcome driven solutions for
all who inhabit built environments
79. The Future of the Interior Design Profession is on a springboard...
Post graduate programs need to evolve
around a finite group of topics that can build
a strong foundation for the profession and all
whom we serve
Interior Designers need to be translators of
productive, safe, resilient environments for
the betterment of mankind
Interiors need to be created within an
interdisciplinary team using evidence-based
hypothesized outcome driven solutions for
all who inhabit built environments
80. The Future of the Interior Design Profession is on a springboard...
A shift in practice methodology must lead to
evidence-based design
Post graduate programs need to evolve
around a finite group of topics that can build
a strong foundation for the profession and all
whom we serve
Interior Designers need to be translators of
productive, safe, resilient environments for
the betterment of mankind
Interiors need to be created within an
interdisciplinary team using evidence-based
hypothesized outcome driven solutions for
all who inhabit built environments