Download to read offline
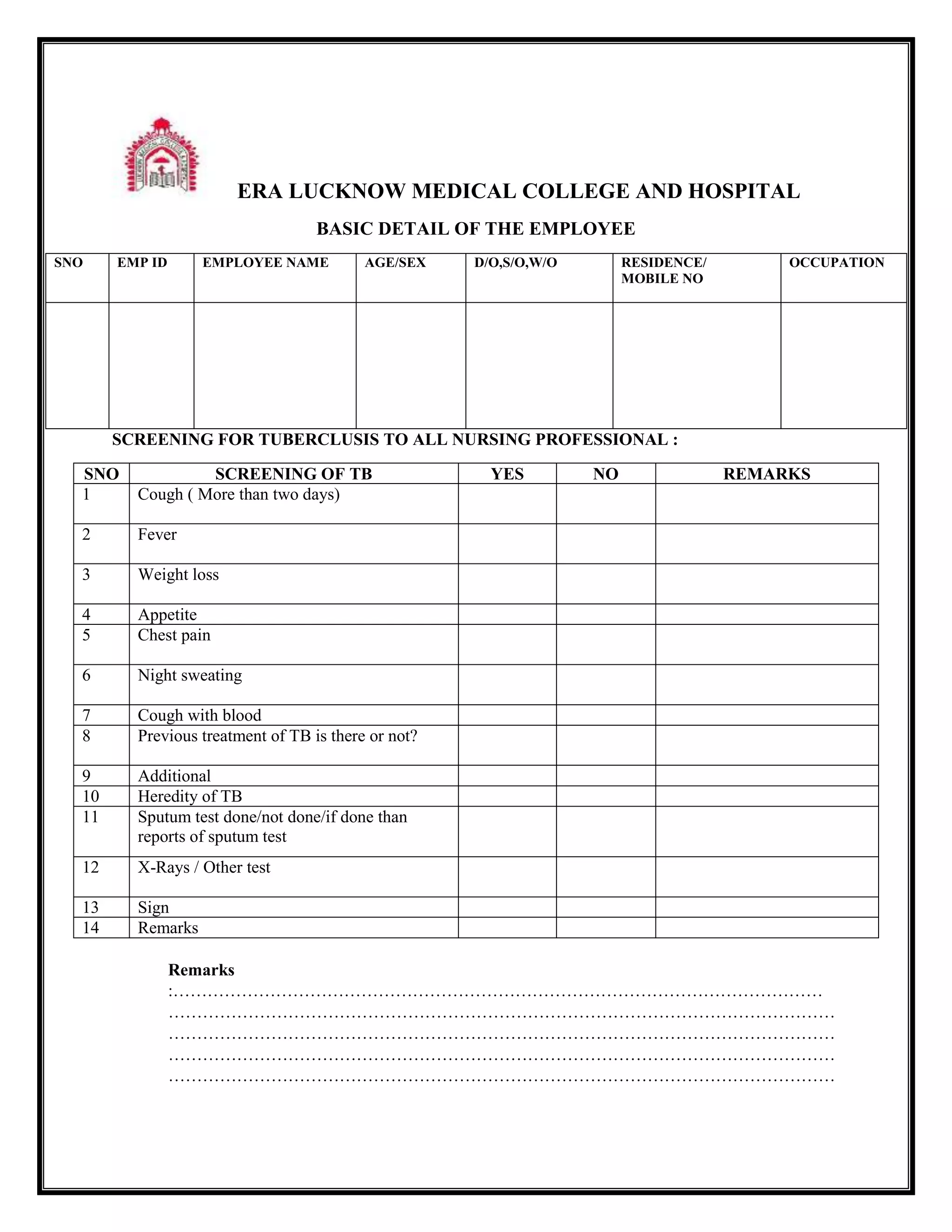
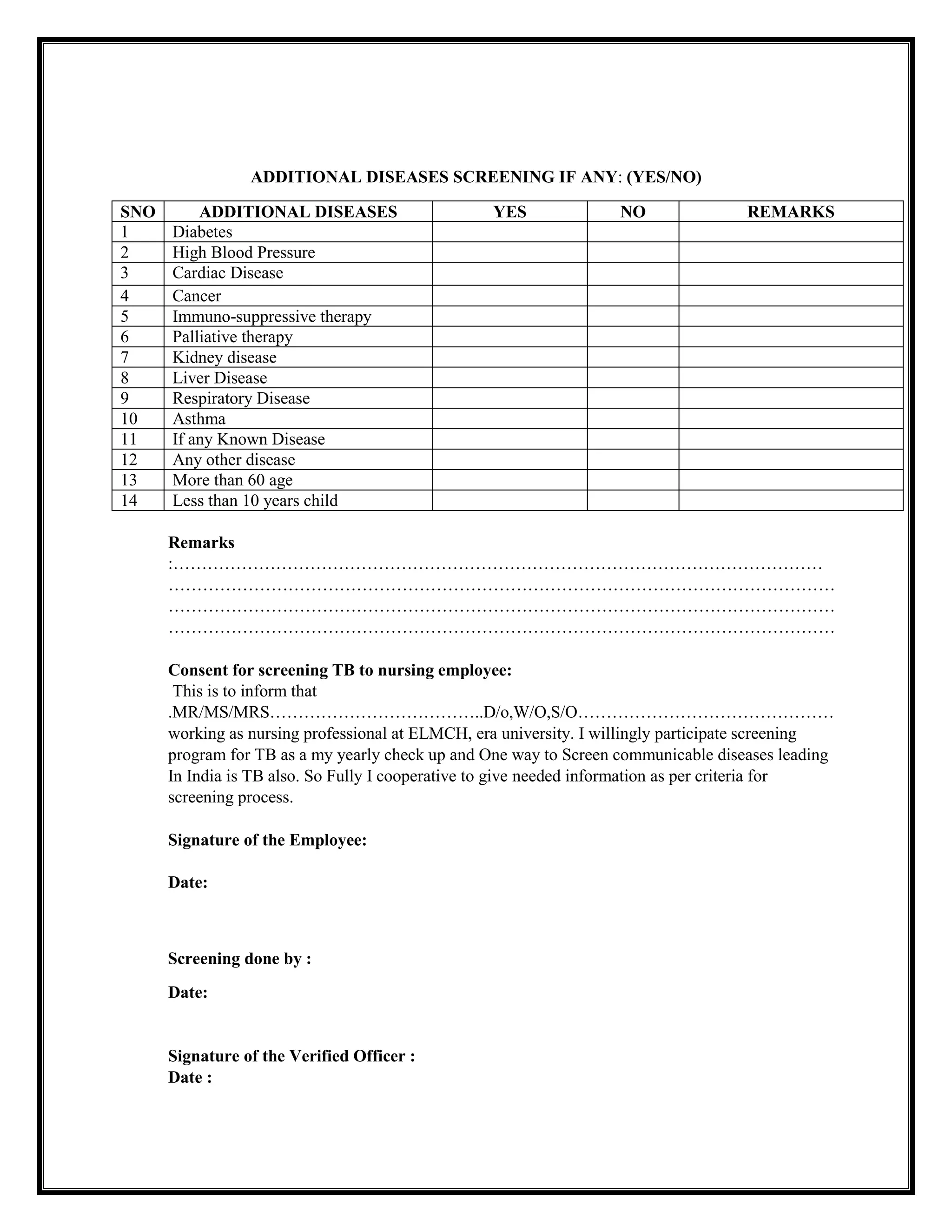

This document contains forms for screening nursing professionals for tuberculosis (TB) and other diseases at ERA Lucknow Medical College and Hospital. It lists questions about TB symptoms, previous treatment, family history, and test results. It also screens for additional diseases like diabetes, high blood pressure, cancer, and respiratory illnesses. The final section is a consent form for an employee to agree to TB screening as part of their annual checkup since TB is a communicable disease prevalent in India.
































![Number_Guessing_Game_Dsbsbssbzboc[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/numberguessinggamedoc1-251206215042-a076fc05-thumbnail.jpg?width=640&height=640&fit=bounds)








