
Recommended
More Related Content
Similar to Anal fissure (fissure in ano)
Similar to Anal fissure (fissure in ano) (20)
Recently uploaded
Recently uploaded (20)
Anal fissure (fissure in ano)
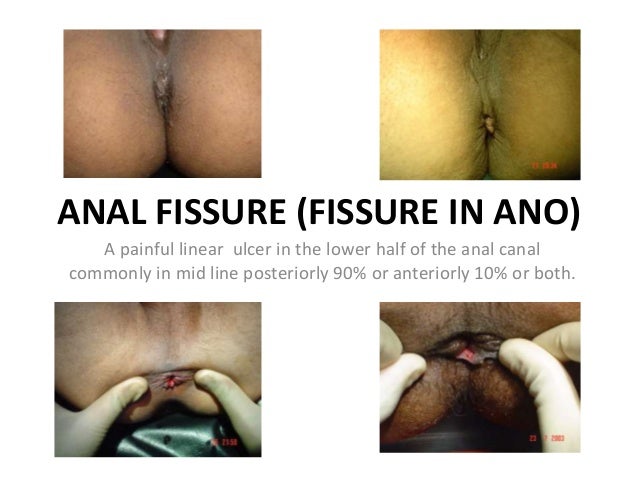
- 1. ANAL FISSURE (FISSURE IN ANO) A painful linear ulcer in the lower half of the anal canal commonly in mid line posteriorly 90% or anteriorly 10% or both.
- 2. Anal Fissure • An elongated ulcer in the long axis of the lower half of the anal canal usually at midline posteriorly or anteriorly or both, and rarely laterally. • It extends from the pectinate line (dentate line) to the margin of the anal verge where a sentinel pile is common in chronic cases. • It is a painful condition, associated with extreme increase in anal tone, leading to distressful constipation. • It may be acute, chronic or recurrent and usually occurs alone and sometimes with other anal diseases e.g. hemorrhoids. • It is more common in young females, usually after child birth or lower abdominal operations eg, C section, TAH, etc.
- 5. Etiology slide a • The primary anal fissure is due to trauma on defecation and secondary anal fissure is due to diseases, (like inflammatory bowel diseases, sexually transmitted diseases, tuberculosis, malignancy and rarely the passage of a sharp foreign body). • Midline affection is due to comparative fixation of the anal canal anteriorly by perineal body and posteriorly by coccyx (which do not allow much dilatation on defecation), while laterally ischiorectal fossas allow dilatation on defecation, leads to stretching anteriorly and posteriorly, so fissures in midline. • More frequent posterior fissures are due to more rigidity of coccyx posteriorly.
- 6. Etiology Slide b • Lower anal canal affection is due to unsupportive anal verge and on sudden passage of hard stools after resistance of coccyx and perineal body, to no resistance of anal verge leading to trauma. • The acute anal fissure on repeated trauma and infection becomes chronic. • Sentinel pile formation is due to over-healing and non stretching of perineal skin as compared to the anoderm where healing gives away on repeated trauma. • This anal fissure leads to increased anal tone, so constipation and vicious circle started; pain leads to constipation which leads to exaggeration of ulcer.
- 7. Examination of anal fissure in a child in out door.
- 8. Pathophysiology Slide a Acute anal fissure • It is an acute ulcer of lower half of anal canal and its base is formed by the anal sphincter muscles with little inflammatory induration or oedema of its edges. • Because the fissure occurs in the sensitive stratified squamous epithelium of the anal canal, pain is the most prominent symptom. • The accompanying spasm of the anal sphincter is marked. • It is not palpable. • Sentinel pile is not present.
- 9. Acute anterior and posterior anal fissures
- 10. Acute anterior and posterior anal fissure
- 11. Pathophysiology Slide b Chronic anal fissure • It is characterized by inflamed indurated thick margins, a base consisting of either scar tissue or the lower border of the anal sphincter muscles and an oedematous tag of skin at its lower end (sentinel pile). • In chronic fissure, there may be spasm of musculature of the anal sphincter and in long-standing cases, this muscle becomes organically contracted by infiltration of fibrous tissue. • Infection of the base may lead to an abscess, which may rupture through the base of the fissure or through the skin, a short distance away, leaving a short subcutaneous fistula.
- 12. Diagnosis Slide a • In acute fissure , tearing, cutting, burning , or agonizing pain starting during defecation, lasting for a variable period afterwards is the main symptom. • The typical history with tightly closed, puckered anus, is almost pathognomonic of the condition. • A simple longitudinal epithelial ulcer situated anteriorly or posteriorly or both, visible at lower anal canal can be seen on slight traction at anal verge. • An acute fissure being a shallow ulcer, is impalpable though the sphincter while spasm is marked and proctoscopy is not tolerable. Examination under anesthesia is recommended. • The patient tends to become constipated, rather than go through the agony of defecation, so a vicious cycle of pain, constipation, and pain is set up. • Bleeding is usually slight and consists of bright streaks on one side of stool, rarely profuse bleeding is presentation. • No age group is exempted, common in women during the meridian of life (pregnancy, delivery and operations of abdomen).
- 13. Inspection of anal verge
- 14. Diagnosis Slide b • In chronic fissure, irritation and discharge, which soil the underclothing is present. • A chronic fissure is felt as an indurated ulcer, but the sphincter spasm is variable. • In cases of chronicity a sentinel skin tag (sentinel pile) is commonly seen and is of varying sizes. • Periods of remission may occur for days or weeks.
- 15. Posterior anal fissure with sentinel pile
- 16. Posterior anal fissure with sentinel pile
- 17. Anterior anal fissure with sentinel pile
- 18. Anterior and posterior anal fissure with sentinel piles
- 19. 25 years old long standing anal fissure with large sentinel pile
- 20. 25 years old long standing anal fissure with large sentinel pile and its treatment.
- 21. Perianal soiling due to anal fissure
- 22. Bleeding from anal fissure is uncommon.
- 23. Bleeding from anal fissure is uncommon.
- 24. A rare unusual small fistulae in anal fissure
- 25. A fistula with anal fissure
- 26. Perianal abscess in anal fissure
- 27. Infection of base may lead to an abscess, which may rupture through the base of the fissure or through the skin, a short distance away, leaving a short subcutaneous fistula.
- 28. Differential Diagnosis Slide a • An acute fissure should be differentiated from an anal abrasion. The latter is superficial with flat edges and is transient. It is not associated with a sentinel pile and responds to conservative treatment. • If anal fissure is situated away from the midline, do suspect pathology (e.g., tuberculosis, syphilis, leukemia, squamous cell carcinoma, or inflammatory bowel disease, especially Crohn's disease, sexually transmitted diseases, etc, and needs biopsy confirmation.)
- 29. Lateral anal fissure Rare one
- 30. Lateral anal fissure with sentinel pile (Rare one)
- 31. Differential Diagnosis Slide b • Tuberculosis ulcer has an undermined edge, the discharge is thin and watery while the presence of a lesion in the chest, a raised erythrocyte sedimentation rate, sputum examination, biopsy may be necessary to reach a diagnosis. • Anal chancre may present as a painful rather than a painless ulcer, has a good deal of induration along with inguinal lymphadenopathy and the serous discharge contains spirochetes. • Secondary syphilis presents as multiple fissures associated with mucous patches in the perianal region and the Wasser mann reaction is strongly positive. • Carcinoma of the anus an epitheliomatous ulcer (malignant) is indurated with raised edges, biopsy is needed for the diagnosis, as in early stages to differentiate it from a fissure and is resistant to the usual local treatment.
- 32. Differential Diagnosis Slide C • Fissures in inflammatory bowel disease tend to be multiple, broad, and situated away from the midline. • Multiple fissures in the perianal skin are commonly seen as a complication of skin diseases, scratching, homosexual practices (sodomy, fisting, use of anorectal sex toys) and anorectal venereal disease. • The possibility of AIDS virus (HIV) being transmitted through this route should be kept in mind: • Specific fissures of this type are often less painful than the appearances of the lesion would suggest and usually associated with delay in wound healing or an early recurrence.
- 33. An example of histopathology of anal fissure
- 34. Anal abrasions- D/D anal fissure
- 35. Conservative treatments Slide a • It consist of application of local anesthetic ointment (xylocaine 5 %) with anal dilators, oral analgesics, metronidazole, suitable broad- spectrum antibiotic, mild laxatives to soften stool, and frequent sitz baths, but it takes prolong time with frequent recurrence. • Should these measures prove ineffective, or if the fissure is chronic with fibrosis, a skin tag (sentinel pile), a hypertrophied anal papilla, presence of large haemorrhoids, or a subcutaneous fistula are indications for operation.
- 36. Operative treatment Slide b • The simplest procedure is controlled dilatation of the sphincter in young adults and children, while moderate dilatation in old age and weak patients by experienced surgeon. • It can be done under caudal, saddle, spinal or SSS with locoregional anaesthesia. • The index and middle finger of each hand are inserted simultaneously into the anus and pulled apart, up to point when sphincter tone gives away. • Apply injection SKL to every case it will almost completely subside post maneuver pain, no infection,no abscess formation and immediate recovery is only possible with this. • No bed rest, no precautions, no incontinence, just normal life.
- 37. Treatment of anal fissure
- 39. Treating acute anal fissure
- 40. Operative treatment Slide C • Lateral internal sphincterotomy is not recommended, it is full of complications, incontinence is serious issue, recurrence is high, and no two surgeons on same page. • You can not differentiate between the internal and external sphincter during operation, it is just an anal sphincter complex, so no fun in cutting the sphincter. • It should be condemned. • Many other procedures are also not required.
- 41. Treatment (Final verdict) • Simplest, and definite treatment is to over come on increased anal tone by controlled calculated anal dilation (up to the point where sphincter tone definitely gives away). • It can be done under saddle, spinal, or SSS with loco regional anesthesia. • Inject SKL in anal sphincter is a must and due to this is no infection, no abscess formation, no post operative pain and early recovery ensues. • Do excise the sentinel pile. • The fissure will heal itself after spasm has disappeared. • No recurrence noted after this way of treatment. • Incontinence is not an issue in routine. (Only old, weak, debilitated patients needs gentle handing). • Immediate back to normal life with no precautions or medications.
- 42. Treatment of anal fissure (Final verdict)
- 43. Thanks