
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Vernal catarrh/ vernal keratoconjuctivitis
Similar to Vernal catarrh/ vernal keratoconjuctivitis (20)
Recently uploaded
Recently uploaded (20)
Vernal catarrh/ vernal keratoconjuctivitis
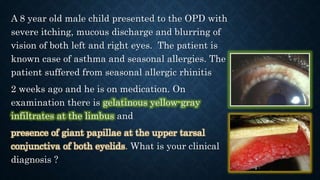
- 1. A 8 year old male child presented to the OPD with severe itching, mucous discharge and blurring of vision of both left and right eyes. The patient is known case of asthma and seasonal allergies. The patient suffered from seasonal allergic rhinitis 2 weeks ago and he is on medication. On examination there is gelatinous yellow-gray infiltrates at the limbus and presence of giant papillae at the upper tarsal conjunctiva of both eyelids. What is your clinical diagnosis ?
- 2. By : SUGUNESHWARAN R (89) SRIRAMKUMAR R (88) SUWATHEESWARAN M (91) S.UMASHRI (94)
- 3. INTRODUCTION • Vernal keratoconjunctivitis also Spring catarrh or Vernal catarrh • It is potentially sight-threatening allergic disorder of children, characterized by chronic inflammation of the ocular surface • It is recurrent, bilateral, interstitial, self limiting, allergic inflammation of conjunctiva having a periodic seasonal incidence. • It is due to hypersensitivity reaction to some exogeneous allergens like pollen grains
- 4. ETIOLOGY • PREDISPOSING FACTORES Age: 4-20 years Gender: boys> girls Season : summer (aka warm weather conjunctivitis) Climate: prevalence tropic > temperate >>> cold climate (non existant) Family history of atopy (40-60% patients) other atopic manifestations (40-75% patients) : eczema or asthma or hay fever Due to Th2 lymphocyte alteration and the exaggerated IgE response to common allergens is a secondary event.
- 6. PATHOLOGY CONJUCTIVAL EPITHELIUM The mast cells, eosinophils that present in papillary region will undergo hyperplasia due to which there is a downward projections into subepithelial tissues ADENOID LAYER Will show marked cellular infiltration by mast cells, eosinophils, plasma cells, lymphocytes and histiocytes FIBROUS LAYER This layer undergoes proliferation and later undergoes hyaline changes CONJUCTIVAL VESSELS These vessels show proliferation, increased permeability and vasodilation Leads to formation of multiple papillae in the upper tarsal conjunctiva
- 7. SYMPTOMS • BURNING AND ITCHING SENSATIONS. ITCHING IS MORE MARKED IN PALPEBRAL FORM OF DISEASE • MILD PHOTOPHOBIA • LACRIMATION • STRINGY DISCHARGE (ropy or mucoid) • HEAVINESS OF EYELIDS CLINICAL COURSE : • SELF LIMITING AND USUALLY BURNS OUT SPONTANEOUSLY AFTER 5-10 YEARS
- 9. PALPEBRAL VKC • Present in upper tarsal conjunctiva of both eyes in involved • COBBLE STONE or PAVEMENT STONE : hard, flat topped papillae fashion along the conjunctival hyperemia • Papillae may hypertrophy to produce cauliflower like structures –GIANT PAPILLAE • White ropy discharge is present • Differential diagnosis :it needs to be differentiated with trachoma with TRACHOM A
- 10. BULBAR VKC • Dusky red triangular congestion of bulbar conjunctiva in palpebral part • Limbal papillae occurs as gelatinous, thickened confluent accumulations of tissue around limbus • Horner Tranta spots: it is discrete whitish raised dots along the limbus
- 11. MIXED VKC • Combined of both palpebral and bulbar forms
- 13. VERNAL KERATOPATHY • Corneal involvement in vernal keratoconjunctivitis is called as VERNAL KERATOPATHY. • It is more common with palpebral form of VKC.
- 14. TYPES OF LESIONS • Types of lesions produced are : 1) Superior punctate epithelial keratitis 2) Epithelial macro erosions 3) Vernal corneal plaques 4) Ulcerative vernal keratitis 5) Subepithelial scarring 6) Pseudogerontoxon
- 15. 1) SUPERIOR PUNCTATE EPITHELIAL KERATITIS : Involves upper cornea , associated with palpebral VKC. Caused by irritation from the inflamed tarsal conjunctiva. Stained with – Rose Bengal stain and fluorescent dyes.
- 16. 2) EPITHELIAL MACRO EROSIONS : due to coalescence of punctate lesions and here BOWMAN’S membrane is intact 3) VERNAL CORNEAL PLAQUES : due to coating of eroded areas with exudate.
- 17. 4) ULCERATIVE VERNAL KERATITIS : SHIELD ULCERATION , presenting as shallow transverse ulceration in upper cornea. due to enlargement of epithelial macro erosions. complicated by bacterial keratitis.
- 18. 5) SUBEPITHELIAL SCARRING - occurs as a ring scar. 6) PSEUDOGERONTOXON develops in recurrent limbal VKC characterised by CUPID’S BOW outline.
- 20. TREATMENT 1. Topical anti-allergic & anti-inflammatory drugs • Dual action antihistamine & mast cel stabilizers -control & prevention exacerbation -1st line of treatment in mild to severe case -olopatadine(0.1%),azelastine,bepotastine(1.5%) • Mast cell stabilizers -Sodium cromoglycate(2%) drops 3-4 times a day controlling VKC especially atopic cases
- 21. • Topical steroids -Effective in all VKC -reserved for moderate to severe & recalcitrant cases as they cause steroid induced glaucoma -monitoring of IOL is very important -intensive but short tapering course i.e instillation (2 hrs) for 7days tapering dose for 3-4 weeks - fluorometholone(0.1%),loteprednol(0.5%),prednisolone,betamethasone, dexamethasone • Topical immunomodulators -indicated whed steroids are ineffective,inadequate,or poorly tolerated, or given as steroid sparing agent in severe disease -cyclosporine(0.5-1%) tacrolimus(0.03% ointment)-------refractory cases
- 22. 2. Topical lubricating and mucolytics • Artificial tears – carboxy methyl cellulose – soothing effect • Acetyl cysteine(0.5%) – mucolytics – early plaque formation 3. Systemic therapy • Oral antihistamines – itching in severe cases • Oral steroids – advanced, very severe, non-responsive cases 4. Treatment of large papillae • Very large papillae can be tackled • Supratarsal injection of long acting steroid • Cryoapplication • Surgical exciion – extraordinarily large papillae
- 23. SUPPORTIVE MEASURES • Dark goggles to prevent photophobia • Cold compresses and ice packs – soothing effect • Eye rubbing should be avoided as it causes mast cell degranulation • Change of places from hot to cold area is recommended for recalcitrant cases
- 24. TREATMENT FOR VERNAL KERATOPATHY • Punctate epithelial keratitis requires no extra treatment except instillation of steroids should be increased • Large vernal plaque – surgical excision by superficial keratectomy • Severe shield ulcer resistant to medical therapy may need surgical treatment in form of debridement, superficial keratectomy, excimer laser therapeutic keratectomy as well as amniotic membrane transplantation to enhance re-epithelialization