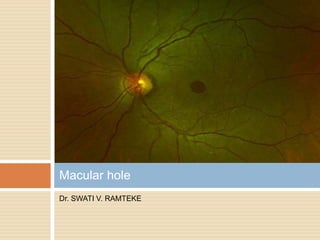
2. Macular hole (MH) is a round full-thickness
opening in the foveal center.
HISTORY:
MH was first described in 1869 by Knapp in a
traumatic case.
Gass - proposed a staging system - on the
basis of his biomicroscopic observations.
Hee et al. were the first to describe the stages
of MH on OCT scans.
3. Prevalence of MH reported in the literature
varies greatly.
1.7per 1000 in a study in Southern India.
Female-to-male ratio of 3.3.to 1. Bilateral in
5% to 16 % of patients.
Risk factors – age 65 or older and females.
4. Introduction
Idiopathic
Myopia
CME
Retinal vascular
diseases
Retinal detachment
Trauma
Lightening strike
Hypertensive
retinopathy
Most of the macular
holes occur as age
related idiopathic
condition not
related to specific
preceding events or
ocular problems
5. PATHOGENESIS
HYPOTHESIS :
Vitreomacular Traction (VMT) - anteroposterior
traction of vitreous fibers on the fovea.
FOVEAL CYSTS - foveal cyst formation due to
vitreous traction was the first step in MH
formation. It was considered to be a prehole
condition.
Contraction of Premacular Vitreous Cortex - Gass
postulated that the tangential contraction of the
prefoveal “posterior hyaloid membrane” resulted
in detachment of the central photoreceptors
and then in the opening of the fovea.
6. PVD - attachments of the posterior hyaloid to
the foveal center and optic disc are the last to
be released. It leads to the creation of oblique
tractional forces on the foveal floor.
7. SYMPTOMS – decrease in visual
acuity,metamorphosia,central scotoma
Amslers grid test and/or Watzke Allens test
DIAGNOSIS – slit lamp biomicroscopy,an
indirect peripheral examination,OCT.
OCT – diagnosis,staging,prognosis and fellow
eye screening.
11. OCT - replaced biomicroscopy for the
diagnosis of MH.
A new classification has been proposed based
on both the MH diameter and the status of the
vitreous attachment at the hole edge on OCT.
13. STAGE 1A MH
Perifoveolar
detachment of
posterior hyaloid.
Foveal cyst in the
inner foveola, and/or
foveolar detachment
of the cone outer
segment tip line.
VMT +
14. STAGE 1B MH
Perifoveolar
detachment of
posterior hyaloid.
Foveal cyst
extending in the
outer retina, causing
a break in the
photoreceptor layer.
“Occult Macular
Hole”.
VMT +.
15. STAGE 2 MH
Hole of various size.
Partial opening of the
roof of the cyst ,the
operculum staying still
attached to the edge of
the hole. Partial
detachment of the
posterior hyaloid, which
is still attached at the
operculum. The
operculum contains
retinal tissue. Small or
16. STAGE 3 MH
Hole of various size.
Posterior hyaloid
detached from the
macular surface, but
still attached to the
optic disc, most
often containing an
operculum.
Medium or large
FTMH with VMT
17. STAGE 4 MH
Hole of various size,
with complete PVD
on biomicroscopy.
The posterior
hyaloid is not visible
on OCT.
Small,medium, or
large FTMH without
VMT
18. Stage 1A ,B –
Foveal
pseudocyst,Impendi
ng MH
Stage 2 –lamellar
macular hole
Stage 3 – FTMH
without PVD
Stage 4 – FTMH
with PVD
19. DD’s of MH
Lamellar macular
hole (LMH) was
coined by Gass in
1975.
Results from
opening of central
cyst of CME.
20. Pseudohole
Thickening of the
macula contracted
by an ERM and the
U or V shape of the
fovea.
no loss of retinal
tissue at the umbo
of the fovea.
21. SECONDARY MH
ORBITAL TRAUMA
In children and young male
adults.
Due to sudden axial
compression of the eye
resulting in equatorial
expansion and retinal
rupture of the fovea.
Combined with other
fundus lesions such as
choroidal or Bruch's
membrane disruption,
commotio retinae,
sclopetaria, or peripheral
breaks.
22. SECONDARY MH
MYOPIC MH
Complications of high
myopia .
May be asymptomatic
MH occur after a
progressive decrease
in vision due to the
worsening of
foveoschisis.
Visual postoperative
prognosis for MH -
poor
24. TREATMENT
Stage 1A ,1B MH – Observation
Spontaneous closure in 50% or progress to
stage 2 MH.
Stage 2,3,4 MH – requires surgery – vitrectomy.
25. MACULAR HOLE SURGERY
Kelly and Wendel first initiated successful surgery
for MH and reported their results for 52 cases in
1990 with a success rate 58%.
Pars Plana Vitrectomy (PPV) - to separate the
posterior cortical hyaloid from the retinal surface
of the macula.
Internal limiting membrane peeling (ILM) – using
brilliant blue(BB), indocyanine green (ICG) or
tryphan blue (TP) dyes or triamcinolone (TA).
ICG dye – RPE toxicity, visual field defects noted.
Inverted ILM flap – large MH, myopic MH.
26. Tamponade - by dehydrating hole edge and then
by preventing fluid currents from hampering the
healing process.
Agents - Air, SF6, C3F8, SILICONE OIL.
Positioning - to maintain a face-down position for
10 to 14 days postoperatively.
Anatomical closure - 91% to 98% for FTMHs
Visual prognosis - better closure rates and better
final visual acuities when the duration of
symptoms is less than 6 months.
27. Complications – Cataract in phakic eyes within
1st few years.
Intraoperative Retinal tears.
Retinal detachment , visual field defect,
endophthalmitis.
IOP rise in case of gas tamponade in high
altitudes.
Late reopening of MH.
28. VITREOPHARMACOLYSIS
OCRIPLASMIN - a recombinant
protease,approved by the FDA in 2012 for the
management of symptomatic VMA.
Lower MH closure rates , electroretinographic
abnormalities, macular detachment, and
dyschromatopsia.