Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (18)
Similar to cfDNA and TP53 Mutation Diagnostic for HBV-HCC in Africans
Similar to cfDNA and TP53 Mutation Diagnostic for HBV-HCC in Africans (20)
cfDNA and TP53 Mutation Diagnostic for HBV-HCC in Africans
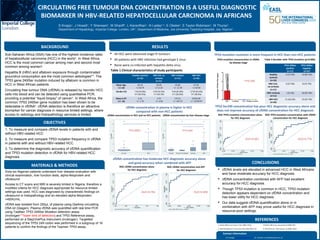
- 1. Table 1.Clinical characteristics of study participants CIRCULATING FREE TUMOUR DNA CONCENTRATION IS A USEFUL DIAGNOSTIC BIOMARKER IN HBV-RELATED HEPATOCELLULAR CARCINOMA IN AFRICANS BACKGROUND Sub-Saharan Africa (SSA) has one of the highest incidence rates of hepatocellular carcinoma (HCC) in the world1 . In West Africa, HCC is the most common cancer among men and second most common among women2 . Hepatitis B (HBV) and aflatoxin exposure through contaminated groundnut consumption are the most common aetiologies**. The TP53 gene 249Ser mutation induced by aflatoxin is common in HCC in West African patients. Circulating free tumour DNA (cfDNA) is released by necrotic HCC cells into blood and can be detected using quantitative PCR, providing a potential “liquid biopsy” of cancer3 . In West Africa, the common TP53 249Ser gene mutation has been shown to be detectable in cfDNA4 . cfDNA detection is therefore an attractive biomarker for cancer diagnosis in resource limited settings, where access to radiology and histopathology services is limited. OBJECTIVES 1. To measure and compare cfDNA levels in patients with and without HBV-related HCC 2. To measure and compare TP53 mutation frequency in cfDNA in patients with and without HBV-related HCC 3. To determine the diagnostic accuracy of cfDNA quantification and TP53 mutation detection in cfDNA for HBV-related HCC diagnosis RESULTS All HCC were advanced stage IV tumours All patients with HBV infection had genotype E virus None were co-infected with hepatitis delta virus CONCLUSIONS REFERENCES MATERIALS & METHODS Sixty-six Nigerian patients underwent liver disease evaluation with clinical examination, liver function tests, alpha-fetoprotein and ultrasound. Access to CT scans and MRI is severely limited in Nigeria, therefore a modified criteria for HCC diagnosis appropriate for resource-limited settings was used. HCC was diagnosed by characteristic findings on ultrasound or histopathology and an elevated alpha-fetoprotein >400IU/mL. cfDNA was isolated from 250μL of plasma using QiaAmp circulating DNA kit (Qiagen). Plasma cfDNA was quantified with real time PCR using TaqMan TP53 249Ser Mutation detection assay (Invitrogen***lower limit of detection) and TP53 Reference assay, performed on a StepOnePlus instrument (Invitrogen). Targetted sequencing of the TP53 249 codon was performed in a subgroup of 16 patients to confirm the findings of the Taqman TP53 assay. cfDNA levels are elevated in advanced HCC in West Africans and have moderate accuracy for HCC diagnosis. cfDNA concentration combined with AFP had excellent accuracy for HCC diagnosis. Though TP53 mutation is common in HCC, TP53 mutation detection appears dependent on cfDNA concentration and has lower utility for HCC diagnosis. Our data suggest cfDNA quantification alone or in combination with AFP may prove useful for HCC diagnosis in resource-poor settings. 1. Parkin DM et al; Cancer J Clin 2005; 55(2). 2.Parkin DM et al; Lancet Oncol 2008; 9(7) 3. Alix=Panabieres C et al; Annu Rev Med 2012; 63. 4. Kirk GD et al; J Nat Cancer Ins 2000; 92(2) Contact Information Dr S Knapp: s.knapp@imperial.ac.uk; Dr J Howell: j.howell@imperial.ac.uk S Knapp1 , J Howell1 , Y Sherwani1 , M Shariff1 , L Karanfilian1 , N Ladep1,2 , E Okeke2 , S Taylor-Robinson1 , M Thursz1 . Department of Hepatology, Imperial College, London, UK1 ; Deparment of Medicine, Jos University Teaching Hospital; Jos, Nigeria2 . Healthy Controls (n=16) HBV CLD, no cirrhosis (n=11) HBV cirrhosis (n=11) HBV HCC (n=26) Mean Age (+/-sd) 44.19 +/-16.75 42.09 +/-11.23 45.00 +/- 11.39 47.50 +/-16.50 Gender (%) 7 M (43.8%) 9 F (56.2%)) 6 M (54.5%) 5 F (45.5%) 9 M (81.8%) 2 F (18.2%)) 17 M (63.4%) 9 F (36.6%) Mean α-FP (+/- sd) 2.14 +/- 1.70 3.72 +/- 3.04 175.21 +/- 547.27 15434.38 +/- 13730.97 cfDNA concentration in plasma is higher in HCC compared with non-HCC patients cfDNA concentration has moderate HCC diagnostic accuracy alone and good accuracy when combined with AFP P=0.0003 P=0.004 AUC=0.762 AUC=0.958 ROC cfDNA concentration alone for HCC diagnosis ROC cfDNA concentration and AFP for HCC diagnosis TP53 Ser249 concentration has poor HCC diagnostic accuracy alone and does not improve accuracy of cfDNA concentration for HCC diagnosis AUC=0.661 AUC=0.778 TP53 mutation mutation is more frequent in HCC than non-HCC patients ROC TP53 mutation concentration alone for HCC diagnosis ROC TP53 mutation concentration with cfDNA concentration for HCC diagnosis TP53 mutation concentration in cfDNA by disease stage Table 2.Number with TP53 mutation (p=0.006) HCC Cirrhosis CLD Healthy controls 0 1 2 3 ConcentrationTP53SerDNA(ng/μL) P=0.026 cfDNA concentration in HCC and no HCC patients cfDNA concentration by liver disease stage TP53 249Ser positive (n=17) TP53 249Ser negative (n=47) Healthy controls (n=16) 2 (12.5%) 14 (87.5%) HBV CLD, no cirrhosis (n=11) 3 (27.3%) 8 (72.7%) HBV cirrhosis (n=11) 1 (9.1%) 10.(91.9%) HBV HCC (n=26) 11 (42.3%) 15 (57.7%)