Management of Hypothyroid and Pregnancy
•Download as PPTX, PDF•
3 likes•1,465 views

Invited lecture delivered by Dr Sujoy Dasgupta in a webinar organized by Thyronorm division of Abbott, held in June, 2021

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Management of Hypothyroid and Pregnancy
Similar to Management of Hypothyroid and Pregnancy (20)
More from Sujoy Dasgupta
More from Sujoy Dasgupta (20)
Recently uploaded
Recently uploaded (20)
Management of Hypothyroid and Pregnancy
- 1. Proprietary and confidential — do not distribute April 8, 2022 Enter title via "insert>header and footer>footer" | 1 Dr Sujoy Dasgupta MBBS (Gold Medalist, Hons) MS (OBGY- Gold Medalist) DNB (New Delhi) MRCOG (London) Advanced ART Course for Clinicians (NUHS, Singapore) Consultant: Reproductive Medicine, Genome Fertility Centre, Kolkata Visiting Consultant, RSV Hospital, Kolkata Bhagirathi Neotia Women and Child Care centre Woodlands Multispeciality Hospital, Kolkata Managing Committee Member, Bengal Obstetric & Gynaecological Society (BOGS) Secretary, Subfertility and Reproductive Endocrinology Committee, BOGS Executive Committee Member, Indian Fertility Society (IFS)- West Bengal Chapter Executive Committee Member, Indian Society for Assisted Reproduction (ISAR)- Bengal Member, Endocrinology Committee, Federation of Obstetric and Gynaecological Societies of India (FOGSI) Winner, Prof Geoffrey Chamberlain Award, RCOG World Congress, London, 2019 Thyroid disorders in pregnancy
- 2. Proprietary and confidential — do not distribute April 8, 2022 Enter title via "insert>header and footer>footer" | 2 Thyroid physiology in pregnancy
- 3. Pregnancy is a Natural Stress Test for Thyroid Gland 3 ↑Oestrogen in pregnancy 2-3 fold ↑TBG ↑TT4, ↑TT3 Similar structure of hCG and TSH hCG stimulates release of T3 / T4 Transient TSH ↓ in 8-14wks ↑ Peripheral metabolism of TH ↓ fT3 & fT4 1. Jameson JL. Harrison's Principles of Internal Medicine. 2008:2224-2247. 2. Lazarus JH. Br Med Bull.2010;1-12. 3. Galofre JC, Davies TF. J Womens Health (Larchmt). 2009;18(11):1847-1856.. ↑ Plasma vol Non-functioning fetal thyroid until 10-12 wks ↑ Demand of T3/T4 (30-50%) Total T4 1.5x non preg range
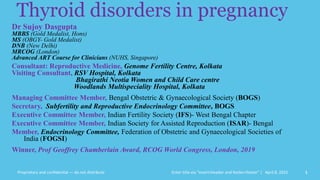
- 4. Proprietary and confidential — do not distribute 10 20 30 40 0 +50 % Change vs. Non-pregnant -50 1st. Trimester 2nd. Trimester 3rd. Trimester E2 TBG hCG TT4 FT4 TSH
- 5. Thyroid disease in Pregnancy: Maternal and Fetal consideration T3 presence in fetal brain at 7 weeks of gestation Fetal thyroid tissue at ~11 weeks HPT axis starts function at ~ 20 weeks Placenta is permeable to T4 Iodine TSH R antibodies Antithyroid drugs Contempre JCEM 1993; Szinnai et. al. JCEM 2006; Vulsma et. al. N Engl J Med 1989
- 6. Proprietary and confidential — do not distribute April 8, 2022 Enter title via "insert>header and footer>footer" | 6 Screening for thyroid disorders in pregnancy
- 7. Results of a Survey answered by 140 Members of the American Thyroid Association 7 Pavani Srimatkandada,1 Alex Stagnaro-Green,2 and Elizabeth N. Pearce1 74% advocated for Universal Screening. 18% against universal screening in pregnancy. 8% were unsure.
- 8. Study Study Design Sample Size TSH Cut-Off % of patients missed with hypothyroidism in pregnancy Wang et al Multicenter Cohort Study Approx 3000 >4mIU/L 81.6% Matsuzek et al Case-Control Study 270 >2.5mIU/L 46.4% Goel et al Prospective Case Control 1,020 >2.5mIU/L 32% Vaidya et al Single Centre Case- Control Study 1,560 >4.2mIU/L 30% Horacek et al Cross Sectional 400 >3.5mIU/L 55% • Meta-analysis has shown that case-based screening can miss up to 49 % of pregnant women with thyroid dysfunction. • Further support for advocacy of universal screening methods for thyroid disorders in pregnancy. Zahra Jouyandeh, Endocrine; 2015
- 9. Proprietary and confidential — do not distribute ATA, 2017 Insufficient evidence to recommend for or against universal screening for abnormal TSH concentrations in early pregnancy. Universal screening to detect low ft4 concentrations in pregnant women is NOT recommended. 08-04-2022 9
- 10. Proprietary and confidential — do not distribute ATA, 2017 All patients seeking pregnancy, or newly pregnant, should undergo clinical evaluation. If any of the following risk factors are identified, testing for serum TSH is recommended: 1. H/O hypothyroidism/hyperthyroidism or current symptoms/signs of thyroid dysfunction 2. Known thyroid antibody positivity or presence of a goiter 3. H/O head or neck radiation or prior thyroid surgery 4. Age >30 years 5. Type 1 diabetes or other autoimmune disorders 6. H/O pregnancy loss, pretermdelivery, or infertility 7. Multiple prior pregnancies (≥2) 8. Family history 9. Morbid obesity (BMI ≥40 kg/m2) 10. Use of amiodarone or lithium, or recent administration of iodinated radiologic contrast 11. Residing in an area of known moderate to severe iodine insufficiency 08-04-2022 10
- 11. ITS & FOGSI 2019 Recommendations For The Management of Thyroid Dysfunction In Pregnancy 11 All pregnant females should be screened at 1st antenatal visit by measuring TSH levels (IIa/B).
- 12. Proprietary and confidential — do not distribute April 8, 2022 Enter title via "insert>header and footer>footer" | 12 TSH reference ranges in pregnancy
- 13. 08-04-2022 13
- 14. Recommendations from Guidelines on Upper TSH limit during pregnancy 14 Guidelines Country of Origin Trimester specific Ref ranges recommended ITS Guidelines 2012 India 1st : 2.5 mIU/L 2nd : 3.0mIU/L 3rd : 3.0 mIU/L ETA Guidelines 2014 European 1st : 2.5 mIU/L 2nd : 3.0mIU/L 3rd : 3.0 mIU/L ATA Guidelines 2017 American • Use locally derived Reference ranges from a specified Pregnant population • If the above is not available use and upper TSH reference limit of 4.0 mIU/L • Only a modest reduction in the upper reference limit 1. Around 0.5 to 1.0 mIU/L reduction 2. Reduction typically occurs at week 7 or later
- 15. Proprietary and confidential — do not distribute T4 estimation in pregnancy Following conception, TBG and TT4 concentration increase by week 7 of gestation, and reach a peak by approximately week 16 • Around 50% increase above pre-pregnancy level is seen at week 16 • This level is sustained throughout pregnancy Ref: Alexander MD et al.. Thyroid, 2017;27(3):315-89. Week Recommendation regarding pregnancy TT4 levels Up to week 7: Use pre-pregnancy range Week 7-16: Increase upper reference range by 5% per week (starting week 7) Week 16 onwards: Increase upper reference range by 50%
- 16. Proprietary and confidential — do not distribute T4 estimation in pregnancy Commonly available automated immunoassays serve well in many situations However, FT4 concentration assessed by automated immunoassays is complicated by • Increase in TBG and NEFA • Decrease in albumin FT4 assessed by equilibrium dialysis, ultrafiltration, or LC/MS are more reliable than automated immunoassays, but • Are much more expensive • Not commonly available Free T4 (FT4) vs. Total T4 (TT4) TBG: Thyroid binding globulin; NEFA: Non-esterified fatty acids; LC/MS: Liquid chromatography/tandem mass spectrometry; Ref: Alexander MD et al.. Thyroid, 2017;27(3):315-89.
- 17. Proprietary and confidential — do not distribute ATA, 2017 TT4 measurements may be superior (with a pregnancy- adjusted reference range) to immunoassay measurement of FT4 measurements in pregnant women, especially during the last part of pregnancy. Accurate estimation of the FT4 concentrations can also be done by calculating a FT4 index.
- 18. Proprietary and confidential — do not distribute April 8, 2022 Enter title via "insert>header and footer>footer" | 18 Hypothyroidism in pregnancy
- 19. Complications of Untreated Hypothyroidism in Pregnancy 19 R V Jayakumar guidelines for Management of thyroid disorder in
- 20. Maternal Medical & Obstetric Variables Assessed in Antenatal Period 0 5 10 15 20 25 %Prevalence Anemia PIH GD IUGR IUD Variables Control Overt Hypothyroid Subclinical Hypothyroid
- 21. Perinatal Outcomes : Delivery & Neonatal Variables 0 10 20 30 40 50 60 Preterm Delivery CS for fetal destress overall CS rate APGAR <7 @ 1 min Neonatal compications Variables % prevalence Control Overt Hypothyroidism Sub clinical Hypothyroidism
- 22. Proprietary and confidential — do not distribute April 8, 2022 Enter title via "insert>header and footer>footer" | 22 Sub Clinical Hypothyroidism in pregnancy
- 23. 23 Thyroid. 2016 Apr;26(4):580-90. SCH during pregnancy is associated with multiple adverse maternal and neonatal outcomes.
- 24. The Haddow Study TSH measured in >25,000 pregnant women 62 mild hypothyroidism; 48 not on thyroxine Mean IQ of children (age 7-9) of the women with high TSH was 4-point lower than the controls Children of the women not on thyroxine • Mean IQ 7-point lower than controls • 15% had IQ 85 or lower (vs. controls 5%) • Undiagnosed hypothyroidism in pregnant women may adversely affect their fetuses; therefore, screening for thyroid deficiency during pregnancy may be warranted. N Engl J Med 1999;341:549-55
- 25. Proprietary and confidential — do not distribute Treatment of Subclinical Hypothyroidism The 2017 ATA Guidelines conclude that the aggregate data available “appear to suggest a benefit of treatment, especially as it applies to reducing miscarriage in TPOAb-positive women.” Five studies published since 2017 Timing of intervention may play an important role in the effectiveness of intervention Casey et al. -No benefit of treating subclinical hypothyroidism starting at a mean gestational age of 16.7 weeks. Hales et al. which began treatment at a mean gestational age of 13.4 weeks, reported no benefit of intervention Zhao et al. reported an overall reduction in pregnancy complication rate in women treated in the first trimester, but not in those treated in the second trimester Nazarpour et al. initiated treatment soon after the first prenatal visit, and found a reduction in the rate of preterm delivery in treated women Gynecol Endocrinol. (2018) 34:845–8 J Clin Endocrinol Metab. (2018) 103:926–35 N Engl J Med. (2017) 376:815–25. J Clin Endocrinol Metab. (2018) 103:1583–91
- 26. Effect of LT4 therapy on pregnancy loss rate and preterm birth rate among pregnant women with SCH Study Study design Patient profile Outcomes Nazarpour S et al. 2018 Double-blind randomized clinical trial Pregnant women with SCH TSH > 2.5 mIU/L Group 1: SCH TPOAb negative (183) received LT4 Group 2: SCH TPOAb negative (183) not received LT4 Group 3: euthyroid TPOAb negative women (1028) • TSH 2.5 to 4 mIU/L with TPOAb negative: No significant difference in preterm delivery [RR: 0.86; CI: 0.47 to 1.55; P = 0.61] • TSH > 4.0 mIU/L TPOAb negative: significantly lower rate of preterm delivery in LT4-treated women compared with those who received no treatment (RR: 0.38; 95% CI: 0.15 to 0.98; P = 0.04). Rao et al. 2019 Systematic review and meta- analysis LT4-treated pregnant women with SCH or TPO-Ab positivity (n=7970) In women with SCH and/or TPOAb positive, LT4 supplementation significantly decreased • Pregnancy loss [RR = 0.56, 95% CI: 0.42–0.75, I2 = 1%, 12 studies] • Preterm birth (RR = 0.68, 95% CI: 0.51–0.91, I2 = 21%, 8 studies) J Clin Endocrinol Metab. 2018 Mar 1;103(3):926-935 Hum Reprod Update. 2019 May 1;25(3):344-361.
- 27. Proprietary and confidential — do not distribute TSH monitoring during pregnancy How frequently to monitor Ref: Alexander MD et al.. Thyroid, 2017;27(3):315-89. Who should be monitored Women with overt or subclinical hypothyroidism (either treated or untreated), or those at risk of hypothyroidism (e.g., patients who are euthyroid but TPOAb or TgAb positive, post-hemithyroidectomy, or treated with radioactive iodine), should be monitored for serum TSH 0 4 8 12 16 20 24 28 32 36 Every 4 weeks till mid-gestation At least once near week 30 Strong recommendation, High quality evidence
- 28. Proprietary and confidential — do not distribute Any other monitoring? In the care of women with adequately treated hypothyroidism, NO OTHER MATERNAL OR FETAL TESTING (such as serial fetal ultrasounds, antenatal testing, and/or umbilical blood sampling) is recommended beyond measurement of maternal thyroid function unless needed due to other circumstances of pregnancy. An exception to this is women with GD effectively treated with 131-I2 ablation or surgical resection, who require TSH receptor antibody (TRAb) monitoring.
- 29. Proprietary and confidential — do not distribute April 8, 2022 Enter title via "insert>header and footer>footer" | 29 Management of Hypothyroidism in pregnancy
- 30. Problems for Optimum Management of Hypothyroidism in Pregnancy Belief thyroxine might harm the baby Nausea and vomiting Other drugs interfering thyroxine absorption Iron Calcium Antacids
- 31. ITS & FOGSI 2019 Recommendations For The Management of Thyroid Dysfunction In Pregnancy During Pregnancy • All overt hypothyroidism with TSH > 2.5 mIU/L should be treated • For overt hypothyroidism Levothyroxine dose to be 1.6-2.0 μg/kg/day • Maintain the target TSH levels ≤2.5 mIU/L (but above lower Ref range) • Patients with pre-existing hypothyroidism, LT4 dose increased by 30% as soon as pregnancy is diagnosed. • One option is to add two additional doses per week (nine doses) ~29% increment 31 Management of overt hypothyroidism
- 32. ITS & FOGSI 2019 Recommendations For The Management of Thyroid Dysfunction In Pregnancy LT4 therapy is recommended for: • Women with a TSH greater than 10.0 mIU/L • TPOAb positive women with a TSH between 4 mIU/L and 10.0 mU/L LT4 therapy can be considered for: • TPOAb negative women with a TSH between 4 mIU/L and 10.0 mU/L • TPOAb positive women with a TSH between 2.5 mIU/L and 4 mU/L Management of Subclinical hypothyroidism in pregnancy
- 33. 2017 ATA guidelines Algorithm for diagnosis & treatment of pregnant women TSH values mentioned are in mIU/L units (ULRR can be con be considered as 4 in absence of local population data) Ref: Alexander MD et al.. Thyroid, 2017;27(3):315-89. In high-risk group women, check TSH as soon as pregnancy is confirmed. Check TPOAb if TSH is between 2.5 and 10 mIU/L TSH 0.1-2.5 TSH 2.5-10 TSH >/=10 No further workup Treat with L- thyroxine TPOAb +ve TPOAb -ve TSH ULRR-10 TSH 2.5-ULRR TSH ULRR-10 TSH 2.5-ULRR Consider treatment No treatment Treat with L- thyroxine Consider treatment
- 34. • Isolated hypothyroxinemia should NOT be routinely treated in pregnancy.
- 35. Postpartum in patients with pre-existing hypothyroidism • Post-delivery the patient should be reverted back to the prepregnant dosage and TSH levels should be rechecked after 6 weeks • Some patients (e.g. some patients with Hashimoto’s thyroiditis) may require a higher dose than pre-pregnancy dose Patients with newly diagnosed hypothyroidism in pregnancy • Some women in whom LT4 is initiated during pregnancy may not require LT4 postpartum. Such women are candidates for discontinuing LT4, especially when the LT4 dose is ≤50 mcg daily. • If LT4 is discontinued, serum TSH should be evaluated in ~ 6 weeks. • Women with thyroid autoimmunity need annual monitoring with TSH. 35 ITS & FOGSI 2019 Recommendations For The Management of Thyroid Dysfunction In Pregnancy Management of hypothyroidism Post-partum
- 36. Proprietary and confidential — do not distribute Hypothyroidism and Lactation • As maternal hypothyroidism can adversely impact lactation, women experiencing poor lactation without other identified causes should have TSH measured to assess for thyroid dysfunction. • Given its adverse impact upon milk production and letdown, subclinical and overt hypothyroidism should be treated in lactating women seeking to breastfeed. • All patients with depression, including postpartum depression, should be screened for thyroid dysfunction.
- 37. Proprietary and confidential — do not distribute Other thyroid preparations? During pregnancy, majority of fetal T3 in CNS is derived from maternal T4 Fetal CNS is relatively impermeable to T3 Ratio of T4:T3 • Desiccated thyroid preparation: 4.2:1 • Secreted by human thyroid: 14:1 Patients using desiccated thyroid or T3+T4 are likely at risk for having insufficient transfer of maternal T4 to fetal brain T3: Triiodothyronine; T4: Thyroxine; Ref: Alexander MD et al.. Thyroid, 2017;27(3):315-89. Recommendation Other thyroid preparations such as T3 or desiccated thyroid should not be used in pregnancy (strong recommendation, low-quality evidence)
- 38. Proprietary and confidential — do not distribute April 8, 2022 Enter title via "insert>header and footer>footer" | 38 Euthyroid pregnant women with thyroid autoimmunity
- 39. Treatment with LT4 decreases the risk of preterm delivery in women who are positive for TPOAb. Eur J Endocrinol (2017) 176, 253–2 Treated Not treated Control
- 40. Effect of Rx with LT-4 in Thyroid autoimmunity and miscarriage/Pre-term delivery 0 5 10 15 20 25 Frequency (%) Miscarriage Pre-term delivery TPOAb+ TPOAb+ LT4 Control Negro et al, J Clin Endocrinol Metab, 2006 *P<0.05 vs. others * * 115 pregnant TPO Ab+ women, TSH <3, randomized to LT4 Rx or placebo LT4 Rx in euthyroid TPOAb+ women ↓ miscarriage & preterm delivery
- 41. Proprietary and confidential — do not distribute ATA, 2017 Although a clear association has been demonstrated between thyroid antibodies and spontaneous pregnancy loss, it does not prove causality and the underlying mechanisms for such an association remain unclear. 1. Ab-mediated mild thyroid hypofunction, 2. cross-reactivity of antithyroid antibodies with hCG receptors on the zona pellucida, 3. the presence of concurrent non–organ-specific autoimmunity, 4. Increased levels of endometrial cytokines in women with thyroid autoimmunity Sporadic loss
- 42. Proprietary and confidential — do not distribute ESHRE, 2018 1. Increased risk of APS positive 2. All women with RPL should be screened for TSH and anti-TPO Checking for T4 should be done in women with abnormal TSH and anti-TPO levels 3. Anti-TPO antibodies are more prevalent in women with RPL and may be associated with increased risk of future loss 4. Women who are euthyroid but anti-TPO positive should NOT be treated with L-thyroxine but TSH should be checked in early pregnancy RPL
- 43. Proprietary and confidential — do not distribute Insufficient evidence exists to conclusively determine whether LT4 therapy decreases pregnancy loss risk in TPOAb-positive euthyroid women who are newly pregnant. However, administration of LT4 to TPOAb-positive euthyroid pregnant women with a prior history of loss may be considered given its potential benefits in comparison with its minimal risk. In such cases, 25–50 mcg of LT4 is a typical starting dose. Treatment with IVIG, selenium, of euthyroid women with a history of recurrent pregnancy loss are NOT recommended. ATA, 2017
- 44. ITS & FOGSI 2019 Recommendations For The Management of Thyroid Dysfunction In Pregnancy Women with thyroid autoimmunity who are euthyroid in the early stages of pregnancy are at risk of developing hypothyroidism and should be monitored with TSH at least once and in every trimester at least up to 2nd trimester. (I/A) LT4 therapy can be considered in euthyroid pregnant women with TPOAb positive and history of pregnancy loss. (IIb/C) 44 Euthyroid pregnant women with thyroid autoimmunity
- 45. Proprietary and confidential — do not distribute • Insufficient evidence exists to recommend for or against treating euthyroid pregnant women who are thyroid autoantibody positive with LT4 to prevent preterm delivery. ATA, 2017
- 46. Proprietary and confidential — do not distribute April 8, 2022 Enter title via "insert>header and footer>footer" | 46 Maternal Hyperthyroidism
- 47. Pregnancy and overt/subclinical hyperthyroidism Overt hyperthyroidism complicates 0.05–0.2% of pregnancies Graves disease is most common (80% to 85%) Subclinical hyperthyroidism has a prevalence of around 1.7% It is often associated with ↑ hCG levels during early pregnancy Hyperemesis gravidarum seems to be associated with SChyper Effects on pregnancy, peri- and neonatal outcome and on later maternal health. ACTA UNIVERSITATIS OULUENSIS D Medica 1092, 2011 Neale D, Burrow G. Thyroid disease in pregnancy. Obstet Gynecol Clin North Am 2004;31(4):893-905, xi
- 48. Effect of Pregnancy on Graves’ Disease Aggravated symptoms of Graves’ disease during the 1st trimester due to increased hCG production Thyrotoxicosis improves in the 2nd & 3rd trimester of pregnancy • Reduction of TSH receptor stimulating antibody levels during pregnancy improves symptoms of Graves’ disease Postpartum, symptoms increase due to a sudden rise in the level of TSH receptor stimulating antibodies 1st trimester 2nd trimester 3rd trimester Post-partum
- 49. First time detection in pregnancy (ATA, 2017) • When a suppressed serum TSH is detected in the first trimester (TSH less than the reference range), a medical history, physical examination, and measurement of maternal serum FT4 or TT4 concentrations should be performed. • Measurement of TRAb and maternal TT3 may prove helpful in clarifying the etiology of thyrotoxicosis. • The appropriate management of abnormal maternal thyroid tests attributable to gestational transient thyrotoxicosis and/or hyperemesis gravidarum includes 1. supportive therapy 2. management of dehydration, and hospitalization if needed 3. ATDs are not recommended 4. Beta blockers may be considered. 08-04-2022 49
- 50. Graves’ disease in pregnancy 50
- 51. Prevalence of various congenital anomalies in previously reported cases (total n = 31) of carbimazole/methimazole embryopathy Systems Congenital anomalies % Skin Aplasia cutis 29 Upper airways Choanal atresia 65 Tracheo-oesophageal fistula 13 GI Patent vitello-intestinal duct 16 Oesophageal atresia 13 Omphalocele 6 Others (e.g. imperforate anus, microcolon, umbilical hernia, gallbladder aplasia) 10 CVS Ventricular septal defects 10 Others (e.g. overriding aorta) 3 Others Dysmorphic facies 68 Nipple anomalies (e.g. athelia, hypoplastic nipples) 23 Developmental delay 16 Deafness 6 Iris/retinal coloboma 6
- 52. J Clin Endocrinol Metab, November 2013, 98(11):4373– 4381 Conclusion: • PTU and MMI/CBZ use in early pregnancy were associated with increased prevalence of birth defects (MMI/CBZ > PTU) • Use of ATD in early pregnancy should be limited • It may be optimal to shift MMI/CBZ to PTU before pregnancy start
- 53. ATA, 2017 In pregnant women with a high risk of developing thyrotoxicosis continued antithyroid medication may be necessary. Factors predicting high clinical risk 1. currently hyperthyroid 2. requirement of >5–10 mg/d MMI or >100–200 mg/d PTU to maintain a euthyroid state. (a) PTU through 16 weeks of pregnancy. (b) Pregnant women receiving MMI should be switched to PTU as early as possible. (c) When shifting from MMI to PTU, a dose ratio of approximately 1:20 should be used (e.g., MMI 5 mg/d = PTU 50 mg twice daily). (d) If ATD therapy is required after 16 weeks gestation, it remains unclear whether PTU should be continued or therapy changed to MMI. 08-04-2022 53
- 54. ATA, 2017 • In women being treated with ATDs in pregnancy, FT4/TT4 and TSH should be monitored approximately every 4 weeks. • Antithyroid medication during pregnancy should be administered at the lowest effective dose of MMI or PTU, targeting maternal serum FT4/TT4 at the upper limit or moderately above the reference range. • A combination regimen of LT4 and an ATD should not be used in pregnancy, except in the rare situation of isolated fetal hyperthyroidism. 08-04-2022 54
- 55. ITS & FOGSI 2019 Recommendations For The Management of Thyroid Dysfunction In Pregnancy • Does not warrant any treatment. Subclinical hyperthyroidism • PTU is recommended during the 1st trimester followed by a switch to methimazole/carbimazole beginning in the second trimester. Choice of Anti-thyroid drug • In women on a low dose of MMI (<5–10 mg/day) or PTU (<100– 200 mg/day), ATD may be stopped. Such patients should be monitored every 1-2 weeks (2-4 wk in 2/3 TM) to assess maternal and fetal thyroid status. Patients on low dose of ATD 55 Maternal Hyperthyroidism
- 56. ITS & FOGSI 2019 Recommendations For The Management of Thyroid Dysfunction In Pregnancy • When ATDs fail to control the hyperthyroid disease (300 mg of PTU or 40 mg/d methimazole/ carbimazole) • 2nd trimester is the safest time suggested for surgery. Surgery is indicated: • Contraception is recommended: at least 3 months following 131I. • There are no data for or against recommending termination of pregnancy after inadvertent 131I exposure Use of 131I is contraindicated (possible teratogenic effects) Maternal Hyperthyroidism
- 57. Already Diagnosed GD Previously ablated (Surgery/ radio I2) Now Euthyroid Maternal serum TRAb in early pregnancy Not detected No further action Elevated Repeat TRAb at 18-22 wk Repeat at 30-34 wk Neonatal check up On ATD Maternal serum TRAb in early pregnancy and 18-22 wk 08-04-2022 57
- 58. Fetal evaluation • There is a possibility of fetal thyrotoxicosis [FHR >160bpm] If mother is euthyroid but positive for TRAb ((>3 times the upper reference for the assay): • Start mother on methimazole/carbimazole to control fetal thyrotoxicosis and LT4 to maintain maternal euthyroidism If all other causes of fetal tachycardia ruled out: • Fetal growth, liquor vol, goitre • Cordocentesis- Mother on ATD, fetal goitre to d/d between fetal hypo and hyperthyroidism Monitoring Maternal Hyperthyroidism
- 59. Proprietary and confidential — do not distribute April 8, 2022 Enter title via "insert>header and footer>footer" | 59 Thyroid Nodules in Pregnancy
- 60. Thyroid nodules in pregnancy Pregnancy is associated with growth of pre-existing thyroid nodules as well as the growth of new nodules Most palpated nodules of the thyroid are benign hyperplastic (or colloid) nodules; however, between 5–20% are true neoplasms, benign adenomas, or carcinomas. The approach to diagnosis in a pregnant woman with a palpable thyroid nodule is similar to that in the non-pregnant woman and includes a serum TSH and an ultrasound assessment of the neck and thyroid gland. 60 Obstet Gynecol Clin N Am. 2010;37(2):173–93 Obstet Gynecol Clin N Am. 2004;31(2):257-85
- 61. 08-04-2022 61
- 62. ITS & FOGSI 2019 Recommendations For The Management of Thyroid Dysfunction In Pregnancy A pregnant woman with a palpable thyroid nodule should be evaluated by measuring serum TSH and an ultrasound assessment of the neck and thyroid gland and FNAC (fine-needle aspiration cytology). (IIa/B) If nodule is malignant or shows rapid growth, consider surgery in the 2nd trimester. (IIa/B) If the nodule is benign, no further evaluation is needed, (except in the cases with elevated TSH), Levothyroxine is given to normalize the TSH and follow-up with USG of the neck. (IIa/B) Thyroid nodules in pregnancy
- 63. ITS & FOGSI 2019 Recommendations For The Management of Thyroid Dysfunction In Pregnancy LT4 suppression therapy should be initiated to maintain the serum TSH in the range of 0.1-0.8 mIU/L for papillary/ follicular cancer and <2.5 mIU/L for medullary cancer If the size of the nodule is stable, repeat biopsy should be performed only after delivery. (IIa/B) Postsurgically, patients should be maintained on LT4 therapy with monitoring of TSH and free T4 levels every 6 weeks. (IIa/C) Postsurgical whole-body scintigraphy and radioiodine remnant ablation are contraindicated during pregnancy and lactation. (I/B) Thyroid nodules in pregnancy
- 64. Proprietary and confidential — do not distribute April 8, 2022 Enter title via "insert>header and footer>footer" | 64 Post partum thyroiditis
- 65. Proprietary and confidential — do not distribute ATA, 2017 • During the thyrotoxic phase of PPT, symptomatic women may be treated with beta- blockers for a few weeks. • ATDs are not recommended for the treatment of the thyrotoxic phase of PPT. • Following the resolution of the thyrotoxic phase of PPT, serum TSH should be measured in approximately 4–8 weeks (or if new symptoms develop) to screen for the hypothyroid phase. • LT4 should be considered for women with symptomatic hypothyroidism due to PPT. • If LT4 is initiated for PPT, discontinuation of therapy should be attempted after 12 months, if not attempting pregnancy or is pregnant. • Women with a prior history of PPT should have TSH testing annually • Treatment of euthyroid thyroid Ab–positive pregnant woman with either LT4 or iodine to prevent PPT is ineffective and is not recommended.
- 66. Proprietary and confidential — do not distribute April 8, 2022 Enter title via "insert>header and footer>footer" | 66 Thyroid disorders and Infertility
- 67. Hypothyroidism & infertility resulting from interplay between HPT & HPO axis 67 Ovulatory disturbance ↓SHBG pool— Androgen Clearance ↓ ↑ TSH (analogy to FSH)Pseudo-Feed back inhibition of FSH/LH Hypothalamo-pituitary changes in Hypothyroidism impair LH response To GnRH-stimuli High TRH Hyper- prolactinemia ↑ Ovarian Volume ↑ Stromal Depots Clin Endocrinol. 2007;66(3):309-321.
- 68. Hormonal changes in Thyroid disorders 68 Endocrine Reviews, October 2010, 31(5):702–755
- 69. Menstrual disturbances in Thyroid disorders 69 Endocrine Reviews, October 2010, 31(5):702–755
- 70. Proprietary and confidential — do not distribute Among infertile women with PCOS, the presence of antithyroid antibodies has been associated with a decreased likelihood of developing ovarian follicles in response to treatment with clomiphene citrate.
- 71. Proprietary and confidential — do not distribute Infertility and subclinical hypothyroidism (SCH) RCT: Randomized controlled trial; SCH: Subclinical hypothyroidism; LT4: Levo-thyroxine; # Estimated duration of infertility before LT4 treatment was 2.8+/-1.7 years, and duration until pregnancy after treatment was 0.9+/-0.9 years. Ref: 1. Alexander MD et al.. Thyroid, 2017;27(3):315-89. 2. Poppe et al. Thyroid, 2002;12(11):997-1001. 3. Abalovich M et al. Gynecol Endocrinol, 2007;23(5):279-83. 4. Yoshioka et al. Endocr J, 2015;62(1):87-92. Note No RCTs; a few observational studies1 Different SCH definitions used; results have been inconsistent1 Study Main observations Poppe et al.2 Prospective study • No increased rates of SCH among infertile women • However, there was slight increase in median serum TSH in infertile women compared to controls (1.3 vs. 1.1 mIU/L; p=0.006) Abalovich et. al.3 Retrospective study • Higher incidence of SCH in infertile women compared to fertile controls (13.9% vs. 3.9%; p<0.002) Yoshioka et. al.4 Retrospective study • 84.1% of infertile women with SCH (TSH > 3 mIU/L) conceived after LT4 therapy • Infertility duration was shortened in SCH women receiving LT4 (p<0.001#)
- 72. Evaluation of serum TSH concentration is recommended for all women seeking care for infertility. (IIa/B) LT4 treatment is recommended for infertile women with overt hypothyroidism. (I/B) LT4 may be considered in subclinical hypothyroidism women who are attempting natural conception given its potential benefits in comparison to its minimal risk. (IIb/C) 72 ITS & FOGSI 2019 Recommendations For The Management of Thyroid Dysfunction In Pregnancy Thyroid Disorders and Infertility
- 73. Proprietary and confidential — do not distribute Attempting natural conception (ATA, 2017) 1. Insufficient evidence exist to determine if LT4 therapy improves fertility in subclinically hypothyroid, thyroid autoantibody–negative women who are attempting natural conception (not undergoing ART). 2. However, administration of LT4 may be considered in this setting given its ability to prevent progression to more significant hypothyroidism once pregnancy is achieved. Furthermore, low dose LT4 therapy (25–50 mcg/d) carries minimal risk. 3. Insufficient evidence exists to determine if LT4 therapy improves fertility in nonpregnant, thyroid autoantibody– positive euthyroid women who are attempting natural conception (not undergoing ART). Therefore, no recommendation can be made for LT4 therapy in this setting.
- 74. SCH & AITD with ART 74
- 75. SCH & AITD with ART 75 miscarriage rate preterm birth rate Given its potential to reduce the miscarriage rate, LT4 supplementation is recommended for infertile women with SCH and/or TAI who are undergoing IVF/ICSI.
- 76. Proprietary and confidential — do not distribute Attempting IVF/ ICSI (ART, 2017) 1. Insufficient evidence exists to determine whether LT4 therapy improves the success of pregnancy following ART in TPOAb- positive euthyroid women. However, administration of LT4 to TPOAb-positive euthyroid women undergoing ART may be considered given its potential benefits in comparison to its minimal risk. In such cases, 25–50 mcg of LT4 is a typical starting dose. 2. Subclinically hypothyroid women undergoing IVF or ICSI should be treated with L-thyroxine, target TSH being <2.5 mIU/L 3. Glucocorticoid therapy is NOT recommended for thyroid autoantibody–positive euthyroid women undergoing ART.
- 77. Proprietary and confidential — do not distribute COS and Thyroid function (ART, 2017) 1. When possible, thyroid function testing should be performed either before or 1–2 weeks after controlled ovarian hyperstimulation because results obtained during the course of controlled ovarian stimulation may be difficult to interpret. 2. In women who achieve pregnancy following controlled ovarian hyperstimulation, TSH elevations should be treated according to the recommendations 3. In nonpregnant women with mild TSH elevations following controlled ovarian stimulation, serum TSH measurements should be repeated in 2–4 weeks because levels may normalize.