
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Antero Lateral thigh flap
Similar to Antero Lateral thigh flap (20)
More from Satish Kumar
More from Satish Kumar (12)
Recently uploaded
Recently uploaded (20)
Antero Lateral thigh flap
- 2. HISTORY • 1984- Song and colleagues –ALT flap based on septocutaneous br of the descending br of LCFA • Koshima et al and kimata - Reconstruction of head and neck defects
- 3. Early anatomic dissections showed that the • Vascular anatomy was variable and • Majority were septocutaneous Recent studies have shown its predominantly musculocutaneous perforators (87% vs 13%)
- 4. INTRODUCTION • Reliable blood supply • Provide a long pedicle with large- diameter vessels • Is pliable • Can be thinned to a significant degree without compromising blood supply
- 5. The flap can also provide different tissue components such as • Muscle, • Fascia, and • Skin in a variety of combinations.
- 6. REGIONAL ANATOMY Anterolateral thigh extends from • Superiorly- anterior superior iliac spine (ASIS) • Inferiorly - lateral femoral condyle • Anteriorly (medially) -medial edge of the rectus femoris muscle • Posteriorly (laterally)- the iliopubic tract.
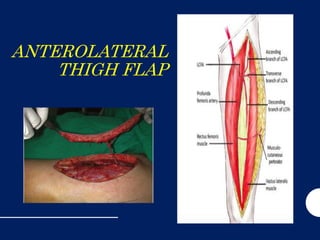
- 7. REGIONAL ANATOMY • Blood supply -branches of the lateral circumflex femoral artery • Venous drainage network of superficial cutaneous veins that drain into the femoral vein. • The lateral femoral cutaneous nerve, (L2–L3 ) provides the sensory innervation to the area
- 11. • French anatomists- described the descending branch autonomously as the 'quadriceps artery' • Though it does not supply vastus medialis • Origin is highly variable but is simplified by classification into three types
- 12. Quadriceps artery origins • TYPE 1 Arises independently from the profunda femoris • Type 2 arises by a common trunk with the lateral circumflex • Type 3 arises from the femoral artery • Salmon also foundType 2 to be the most common (62%) • Territory of lateral circumflex femoral artery - anterior part of vastus lateralis and its overlying skin • Posterior part of the muscle - perforators from the profunda femoris
- 13. • The 'quadriceps artery' gives off the following: • Principal pedicle of rectus femoris • Inferior pedicle of vastus Iateralis • Inferior pedicle of vastus intermedius • The branch to vastus Iateralis is the most constant and the largest of these.
- 14. VENOUS ANATOMY • Venae comitantes accompany the musculocutaneous and septocutaneous branches of the descending branch of the LCFA
- 15. NERVES IN THE REGION • The lateral femoral cut nerve (L2–L3) • Direct branch of the lumbar plexus
- 16. FLAP ANATOMY • Dominant: • Descending branch of the LCFA • Length: 12cm (range 8–16cm) • Diameter: 2.1mm (range 2–2.5mm)
- 17. • Minor: perforator of transverse branch of LCFA • Length: 11cm (range 9–13cm) • Diameter: 2.1mm (range 1.5–2.5mm) • Less commonly, the septocutaneous vessel or musculocutaneous perforator arises from the transverse branch of the LCFA and runs parallel with the vastus lateralis muscle.
- 18. VENOUS DRAINAGE OF THE FLAP • Primary: venae comitantes accompanying lateral circumflex femoral vessel and its branches • Length: 12cm (range 8–16cm) • Diameter: 2.3mm (range 1.8–3.3mm) • Two venae comitantes accompany the arterial pedicle of the anterolateral thigh flap.
- 19. FLAP INNERVATION Sensory • Harvested as a sensate flap by including the lateral femoral cutaneous nerve proximally with the flap and anastomosing it to a sensory nerve at the recipient site Motor • Myocutaneous flap with the vastus lateralis preserving the motor branch to the accompanying muscle
- 20. FLAP COMPONENTS • Cutaneous flap • Composite flap • consisting of a fascial (fasciocutaneous anterolateral thigh flap) • Muscular component (vastus lateralis myocutaneous anterolateral thigh flap)
- 21. CHIMERIC FLAPS Including • Rectus femoris muscle, • Tensor fascia lata, • Anteromedial thigh skin
- 22. FLAP DESIGN • Important landmarks include • Anterior superior iliac spine • Superior lateral border of the patella.
- 23. • The flap is centered at the midpoint of a longitudinal line drawn between these two landmarks. • A circle of 3 cm radius defines the area at which the skin vessels, either septocutaneous vessels or musculocutaneous perforators, exit. • Often found in the inferior lateral quadrant of the circle.
- 24. FLAP DIMENSIONS Skin island dimensions • Length: 21cm (range 4–35cm) • Maximum to close primarily: 22cm • Width: 8cm (range 4–25cm) • Maximum to close primarily: 8cm • Thickness: 5mm (range 3-20 mm)
- 25. MUSCLE DIMENSIONS • Length: from 2cm (cuff) to 20cm (entire muscle) • The descending branch of the LCFA sends branches to the vastus lateralis muscle and a segment can be harvested based on one or more branches. • The tensor fascia lata muscle can be included if the ascending branch of the LCFA is included with the flap. • The rectus femoris muscle or a portion of it can be harvested based on the branch from the descending branch of the LCFA.
- 26. • Although a large skin paddle up to 35cm long and 25cm wide can be harvested on a single dominant perforator • When possible, incorporation of two perforators within the flap ensures greater success. • An eccentric flap with the skin vessel entering at the proximal portion of the flap will allow for greater pedicle length.
- 27. PRE-OP EVALUATION • Functional evaluation of knee extension • Previous scars that may affect flap design. • Prior skin graft donor sites can be incorporated as part of the flap.
- 28. SUPRAFASCIAL • Thin flaps • Preservation of sensory innervation
- 29. SUBFASCIAL • Easier identification of vessels • Better exposure of the intermuscular septum
- 30. FLAP DISSECTION • Identify rectus femoris • Proceed laterally till septum (RF &VL) • Retract RF medially • Identify des br of LCFA • Dissection performed retrograde • Intramuscular dissection- musculocutaneous perforators
- 34. FLAP MODIFICATION • Thin flap • Adipofascial flap • Innervated flap • Functional muscle flap • Flow-through flap • Pedicled flap • Muscle component only • Use of fascial component
- 35. DONOR SITE CLOSURE AND MANAGEMENT • Closed primarily, longitudinal linear scar, if width of the flap harvested is less than 8cm. • Wider defects will require closure with a split-thickness skin graft. • Primary closure of the donor site using V-Y advancements of proximal and distal island flaps based on other perforators, is an alternative method of donor site management.
- 36. FLAP USAGE Pedicled • Lower abdominal wall • Groin • Suprapubic Perineum and penis • Lateral gluteal area • Knee Free flap • Head and neck • Orofacial • Esophagus • Abdominal wall • Breast reconstruction • Penile reconstruction • Perineal reconstruction • Upper extremity • Lower extremity
- 37. PEDICLED FLAP
- 39. TYPICAL INDICATIONS FOR THE USE OF THIS FLAP Head and neck reconstruction • Oral lining and cheek skin • Cervical or thoracic esophageal reconstruction • Pharyngoesophageal reconstruction
- 42. Lower extremity reconstruction Upper extremity reconstruction
- 43. Atypical indications for the use of this flap Esophageal reconstruct ion
- 45. FLOW- THROUGH FLAP • Trauma with vascular compromise • To preserve the arterial vasculature at the recipient site
- 46. POST-OP CARE • Flap viability checked – doppler – 24hrs • Avoid compression on the flap or the pedicle. • Pharyngoesophageal reconstruction are withheld from oral intake for 2 weeks • Protective abdominal binder is used for 12 weeks post abdominal wall reconstruction
- 47. OUTCOMES Success rates are greater than -96%, • Head and neck reconstructions -96% • Lower extremity reconstruction -93% (113 of 121 flaps successful), • Upper extremity reconstruction 93% (54 of 58 flaps successful) • Trunk reconstruction 100% study byWei
- 48. FLAP FAILURE • With adequate experience, the success rate is greater than 95% • Twisting • Compression of the pedicle • Inadequate venous outflow • Hematoma and • Venous or arterial thrombosis • 2% of cases, there is lack of or inadequacy of the skin vessels.
- 49. ADVANTAGES • Ease of harvest • Relatively constant anatomy • Long length and large pedicle. • Versatility in design with variable thickness and incorporation of various tissue components. • Ability to provide sensory innervation. • Lack of significant donor site morbidity • Decreased operative time with two- team approach.
- 50. DISADVANT AGES • Color mismatch in some patients for facial reconstruction. • Presence of hair in some male patients. • Skin graft requirement at donor site if greater than 8 cm width of harvested tissue. • Lack of vessels with reasonable size in rare cases. • Excess flap bulk -requiring secondary flap debulking. • Fistula and stricture -- pharyngoesophageal reconstruction. • Breast reconstruction--fat necrosis
- 51. A CASE OF POST TRAUMATIC RAW AREA OF FOOT – ALT FREE FLAP
Editor's Notes
- (fasciocutaneous flap) on small vessels that extend from the
- This artery is important in the context of flaps because it sends musculocutaneous and fascioc utaneous perforators to the antero-lateral part of the thigh. It will be described in some detail. The lateral circumflex femoral is larger than the medial circumflex and arises from the profunda femoris in 75% ofcases, and from the femoral in the remainder. It passes laterally, usually lying posterior to the divisions of the femoral nerve, to run behind sarto rius and rectus femoris where it divides into ascending, transverse and descending branches (ascending and transvers e generally together).
- The descending branch usually courses inferiorly along the medial edge of the vastus lateralis muscle or, rarely, over the vastus intermedius muscle. In 30% of patients, the descending branch further divides into a medial and lateral branch at the midpoint of a line extending from the ante- rior superior iliac spine to the lateral aspect of the patella. The medial branch courses medially under the rectus femo- ris muscle to supply both the rectus femoris and the skin overlying the anteromedial thigh. The lateral branch trav- els inferiorly along the intermuscular septum between the vastus lateralis and rectus femoris, giving rise to musculo- cutaneous perforators through the vastus lateralis or septo- cutaneous branches, or both, that supply the skin of the anterolateral thigh. Eventually, the lateral branch pierces the vastus lateralis close to the knee. More commonly, the descending branch does not divide and continues inferiorly along the intermuscular septum and, after giving off perfo- rators to the anterolateral thigh, it communicates with the lateral superior genicular artery or profunda femoral artery approximately 3–10 cm above the patella.
- (Fig. 6.96a). Less commonly, proximal to (b) or at the same level as (c) the lateral circumflex.
- and enters the thigh deep to the lateral end of the inguinal ligament. It travels under the tensor fascia lata for approximately 10cm before ris- ing through it and dividing into anterior and posterior branches that supply the skin of the anterolateral thighIt is found in the deep subcutaneous tissue just above the fascia. The motor branch to vastus lateralis muscle originates from the femoral nerve and accompanies the descending branch of the LCFA along the intermuscular septum.
- The descending branch of the LCFA courses obliquely along the intermuscular septum between the rectus femoris and vastus lateralis muscles. It exits in the majority of cases within a circle of 3cm radius located at the midpoint of a line drawn between the anterior superior iliac spine and the superior lateral border of the patella as either a septocuta- neous vessel or a musculocutaneous perforator, or both Septocutaneous vessels run between the rectus femoris and vastus lateralis and traverse the fascia to supply the skin of the anterolateral thigh Septocutaneous vessels run between the rectus femoris and vastus lateralis and traverse the fascia to supply the skin of the anterolateral thigh.
- he sensory nerve branches pierce the muscle fascia 10cm below the inguinal ligament medial to the ten- sor fascia lata muscle. The nerve in that area splits into ante- rior and posterior branches to innervate the anterolateral aspect of the thigh.
- skin and subcutaneous tissue based on either a septocutaneous vessel or musculocutaneous perfo- rator.
- on a separate perforator) based on blood supply from the descending branch or any other branches of the lateral femoral circumflex system For example, a fascio- cutaneous anterolateral thigh flap based on a musculocuta- neous perforator may be harvested with the rectus femoris muscle that is based on an independent pedicle from the lateral circumflex femoral system and would be termed a chimeric fasciocutaneous anterolateral thigh myocutaneous perforator and rectus femoris muscle flap.
- Patients with impair- ment in knee extension or with knee instability may have increased functional deficit after anterolateral thigh flap har- vest and intramuscular dissection of the vastus lateralis as the vastus lateralis muscle is a large component of quadriceps function
- Thinning after flap elevation and before transection of the vascular pedicle. The pedicle entrance into the skin is marked. Preservation of at least a 2cm radius of tissue around the pedicle is recommended to insure adequate perfusion of the flap. The flap is thinned, beginning with the deep fat tissue (wide and flat fat lobules) and progressing up to the junction with the more superficial fat (small and round fat lobules). Usually the quality of fat at these two levels is different, with a thin fascia present between them. Noting this characteristic of the fat lobules results in uniform defatting. Defatting before vessel liga- tion allows for continuous monitoring of flap perfusion throughout the defatting process and for coagulation of bleeding points when necessary. The flap can be thinned up to 3 mm without compromise to the blood supply provided that the flap is within 9cm around the perforator. ----- Meeting Notes (26/11/14 21:48) ----- adipofascial-exposed tendons, gliding surfaces
- he blood supply to the distal island flap is from retrograde flow of the descending branch of the LCFA via the lateral superior genicular artery and the proximal island flap is supplied by anterograde flow by the descending branch of the LCFA.
- econstruction of extensive com- posite defects of the mandible may require two free flaps, both an osteoseptocutaneous flap for bone reconstruction and an anterolateral thigh flap to fill the soft tissue deficit. flap is designed with a width of approximately 9 cm to achieve a 3 cm diam- eter tube and is based on two separate skin vessels to allow for two skin paddles: one for tube reconstruction and one externalized for flap monitoring.