
Recommended
More Related Content
Similar to final peptic ulcer.pptx
Similar to final peptic ulcer.pptx (20)
Recently uploaded
Recently uploaded (20)
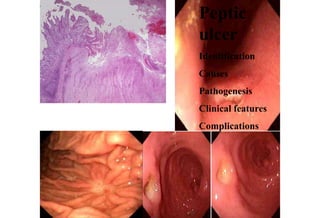
final peptic ulcer.pptx
- 2. • Acute gastritis: transient mucosal inflammation • maybe asymptomatic or cause variable degrees of epigastric pain, nausea and vomiting. • In severe cases there may be mucosal erosion , ulceration ,hemorrhage , hematemesis ,melena. • Chronic gastritis: (Helicobacter pylori, autoimmune, chronic bile reflux) • Nausea and upper abdominal discomfort • Symptoms are less severe but more persistent
- 3. Stomach, acute gastric ulcers Ulcers
- 4. Erosions: breach in mucosal epithelium only Ulcers: Breach in mucosa that penetrate through muscularis mucosae into submucosa, muscularis propria or deeper Peptic ulcers: chronic most often solitary, recurrent lesions can occur in any part of GIT exposed to aggressive action of acid peptic juices 98% - first part of duodenum or stomach in ratio of 4:1
- 5. PEPTIC ULCER • impair the quality of life rather than shorten it. • Most common in gastric antrum and first portion of duodenum • Acute peptic ulceration: focal lesions as result of NSAIDs and physiologic stress. 1cm – Stress ulcers (shock, sepsis, trauma) – Curling ulcers (severe burns, trauma) – Cushing ulcers (intracranial disease) • Peptic ulcer disease
- 7. Causes • H.pylori, NSAIDs • GERD (gastroesophageal reflux disease) • Ectopic mucosa secreting acid • Gastric heteropia in Meckel diverticulum
- 8. Pathogenesis • Imbalance between the mucosal defense forces & the damaging forces • Key conditions for development of peptic ulcer – mucosal exposure to gastric acid & pepsin and hyperacidity, parietal cell hyperplasia, excessive secretary response, impaired inhibition of stimulatory mechanisms like gastrin – Zollinger Ellison syndrome – H. Pylori infection. 70% of PUD associated with H. Pylori out of these 5-10% develop ulcers
- 9. Pathogenesis • Imbalance between the mucosal defense forces & the damaging forces • Key conditions for development of peptic ulcer – mucosal exposure to gastric acid & pepsin and hyperacidity, parietal cell hyperplasia, excessive secretary response, impaired inhibition of stimulatory mechanisms like gastrin – Zollinger Ellison syndrome – H. Pylori infection. 70% of PUD associated with H. Pylori out of these 5-10% develop ulcers
- 13. Pathogenesis: • Co factors • Chronic NSAID use • Cigarette smoking • Corticosteroid high doses • Psychologic stress
- 14. Predisposing factors • Diagnosed in middle to older age group, may become evident in young • Male female ratio 10:4 • Alcoholic cirhosis • Chronic obstructive pulmonary disease • Chronic renal failure • Hyperparathyroidism • Hypercalcemia stimulate gastrin secrtion
- 15. Host defenses •Secretion of Mucus •Secretion of bicarbonate in the surface mucus •Secretion of acid and pepsin containing fluid from the gastric pits as jets •Rapid gastric epithelial regeneration • Robust mucosal blood flow •Mucosal elaboration of prostaglindins which help to maintain mucosal blood flow
- 16. Pathogenesis - HelicobacterPylori • Gram negative rod. Lies in superficial mucous layer & among the microvilli of epithelial cells • Present in 70% patients. Antibiotic t/m promotes healing • No invasion. • Induces inflammation and immune response – ↑production of pro-inflammatory cytokines, IL-1, IL- 6, TNF,IL-8 by mucosal cells activate neutrophils • activation of T & B lymphocytes - cause damage to mucosa • proliferation of lymphoid tissue(MALT),transforms into lymphoma.
- 17. Morphology • Favored sites - first portion of the duodenum & near interface of body and antrum of stomach • Solitary in 80% patients, less than 0.3cm diameter, shallow, but more than 0.6cm are deep. round sharply punched out appearance. • Margins of crater perpendicular. mild edema of adjacent mucosa. no significant elevation or beading of
- 18. Four zones can be seen: 1) Necrotic fibrinoid debris 2) Active inflammation 3) Granulation tissue 4) Fibrous
- 19. Clinical picture • Middle age to older adults, precipitating conditions • Epigastric pain gnawing, burning or aching discomfort • Duodenal ulcer: pain occurs 1-3 hrs after a meal & typically awakens patient in middle of night. Relieved by alkali or food • Gastric ulcer: The relationship between pain & food is more variable
- 20. Complications • Bleeding – Most frequent complication – Accounts for 25% of ulcer deaths • Perforation – Occurs in only 5% of patients – Accounts for 66% of ulcer deaths • Obstruction from edema or scarring • Intractable pain
- 21. Treatment • Antibiotics • Proton pump inhibitors • H-2 receptor inhibitors • Antacids - Neutralization of acids • Surgery
- 22. TRIPLE THERAPY • Triple therapy consists of two antibiotics and one proton pump inhibitor for 7 to 14 days. • Clarithromycin – 500mg tablet BD • Amoxicillin- 1000mg BD or • Metronidazole • Rabeprazole or Esomeprazole 40mg per day
- 23. NSAIDs Inhibit prostaglandin synthesis Increase secretion of HCL Reduce bicarbonate and mucus production Reduce glutathione synthesis Some impair angiogensis
- 34. Stomach, Helicobacter pylori gastritis inflammatory infiltrate
- 35. Stomach, Helicobacter pylori gastritis The presence of neutrophils within the gastric glands signifies active inflammation
- 36. Stomach, chronic peptic ulcer
- 37. Stomach, chronic peptic ulcer
- 38. Stomach, Helicobacter pylori gastritis Lamina propria
- 40. Stomach, Helicobacter pylori gastritis