Effects of Community-Based Health Worker
Interventions to Improve Chronic Disease
Management and Care Among Vulnerable
Populations: A Systematic Review
Kyounghae Kim, RN, MSN, Janet S. Choi, MPH, Eunsuk Choi, RN, PhD, MPH, Carrie L. Nieman, MD, MPH, Jin Hui Joo, MD, MA,
Frank R. Lin, MD, PhD, Laura N. Gitlin, PhD, and Hae-Ra Han, RN, PhD
Background. Community-based health workers (CBHWs) are frontline
public health workers who are trusted members of the community they
serve. Recently, considerable attention has been drawn to CBHWs in pro-
moting healthy behaviors and health outcomes among vulnerable pop-
ulations who often face health inequities.
Objectives. We performed a systematic review to synthesize evidence
concerning the types of CBHW interventions, the qualification and
characteristics of CBHWs, and patient outcomes and cost-effectiveness
of such interventions in vulnerable populations with chronic, non-
communicable conditions.
Search methods. We undertook 4 electronic database searches—PubMed,
EMBASE, Cumulative Index to Nursing and Allied Health Literature, and
Cochrane—and hand searched reference collections to identify randomized
controlled trials published in English before August 2014.
Selection. We screened a total of 934 unique citations initially for titles
and abstracts. Two reviewers then independently evaluated 166 full-
text articles that were passed onto review processes. Sixty-one studies
and 6 companion articles (e.g., cost-effectiveness analysis) met eligi-
bility criteria for inclusion.
Data collection and analysis. Four trained research assistants extracted
data by using a standardized data extraction form developed by the
authors. Subsequently, an independent research assistant reviewed
extracted data to check accuracy. Discrepancies were resolved through
discussions among the study team members. Each study was evaluated
for its quality by 2 research assistants who extracted relevant study
information. Interrater agreement rates ranged from 61% to 91% (av-
erage 86%). Any discrepancies in terms of quality rating were resolved
through team discussions.
Main results. All but 4 studies were conducted in the United States.
The 2 most common areas for CBHW interventions were cancer pre-
vention (n = 30) and cardiovascular disease risk reduction (n = 26). The
roles assumed by CBHWs included health education (n = 48), counseling
(n = 36), navigation assistance (n = 21), case management (n = 4), social
services (n = 7), and social support (n = 18). Fifty-three studies provided
information regarding CBHW training, yet CBHW competency evalua-
tion (n = 9) and supervision procedures (n = 24) were largely under-
reported. The length and duration of CBHW training ranged from 4
hours to 240 hours with an average of 41.3 hours (median: 16.5 hours) in
24 studies that reported length of training. Eight studies reported the
frequency of supervision, which ranged from weekly to monthly. There ...
Effects of Community-Based Health WorkerInterventions to Imp.docx
1. Effects of Community-Based Health Worker
Interventions to Improve Chronic Disease
Management and Care Among Vulnerable
Populations: A Systematic Review
Kyounghae Kim, RN, MSN, Janet S. Choi, MPH, Eunsuk Choi,
RN, PhD, MPH, Carrie L. Nieman, MD, MPH, Jin Hui Joo, MD,
MA,
Frank R. Lin, MD, PhD, Laura N. Gitlin, PhD, and Hae-Ra Han,
RN, PhD
Background. Community-based health workers (CBHWs) are
frontline
public health workers who are trusted members of the
community they
serve. Recently, considerable attention has been drawn to
CBHWs in pro-
moting healthy behaviors and health outcomes among
vulnerable pop-
ulations who often face health inequities.
Objectives. We performed a systematic review to synthesize
evidence
concerning the types of CBHW interventions, the qualification
and
characteristics of CBHWs, and patient outcomes and cost-
2. effectiveness
of such interventions in vulnerable populations with chronic,
non-
communicable conditions.
Search methods. We undertook 4 electronic database searches—
PubMed,
EMBASE, Cumulative Index to Nursing and Allied Health
Literature, and
Cochrane—and hand searched reference collections to identify
randomized
controlled trials published in English before August 2014.
Selection. We screened a total of 934 unique citations initially
for titles
and abstracts. Two reviewers then independently evaluated 166
full-
text articles that were passed onto review processes. Sixty-one
studies
and 6 companion articles (e.g., cost-effectiveness analysis) met
eligi-
bility criteria for inclusion.
Data collection and analysis. Four trained research assistants
extracted
data by using a standardized data extraction form developed by
3. the
authors. Subsequently, an independent research assistant
reviewed
extracted data to check accuracy. Discrepancies were resolved
through
discussions among the study team members. Each study was
evaluated
for its quality by 2 research assistants who extracted relevant
study
information. Interrater agreement rates ranged from 61% to 91%
(av-
erage 86%). Any discrepancies in terms of quality rating were
resolved
through team discussions.
Main results. All but 4 studies were conducted in the United
States.
The 2 most common areas for CBHW interventions were cancer
pre-
vention (n = 30) and cardiovascular disease risk reduction (n =
26). The
roles assumed by CBHWs included health education (n = 48),
counseling
(n = 36), navigation assistance (n = 21), case management (n =
4), social
4. services (n = 7), and social support (n = 18). Fifty-three studies
provided
information regarding CBHW training, yet CBHW competency
evalua-
tion (n = 9) and supervision procedures (n = 24) were largely
under-
reported. The length and duration of CBHW training ranged
from 4
hours to 240 hours with an average of 41.3 hours (median: 16.5
hours) in
24 studies that reported length of training. Eight studies
reported the
frequency of supervision, which ranged from weekly to
monthly. There
was a trend toward improvements in cancer prevention (n = 21)
and
cardiovascular risk reduction (n = 16). Eight articles
documented cost
analyses and found that integrating CBHWs into the health care
delivery
system was associated with cost-effective and sustainable care.
Conclusions. Interventions by CBHWs appear to be effective
when
5. compared with alternatives and also cost-effective for certain
health
conditions, particularly when partnering with low-income, un-
derserved, and racial and ethnic minority communities. Future
re-
search is warranted to fully incorporate CBHWs into the health
care
system to promote noncommunicable health outcomes among
vul-
nerable populations. (Am J Public Health. Published online
ahead of
print February 18, 2016; e3–e28.
doi:10.2105/AJPH.2015.302987)
PLAIN-LANGUAGE SUMMARY
We conducted a review of the studies in
which the effect of community-based health
workers (CBHWs)—public health workers
who are trusted members of the community
they serve—was tested for chronic disease
management and care among people who are
at risk for health disparities. We found 67
relevant studies. Most studies focused on
preventing cancer and cardiovascular diseases.
In these studies, CBHWs carried out several
tasks. The tasks included providing health
education and counseling, helping patients
navigate the health care system, managing
6. care, and providing social services and sup-
port. How CBHWs were trained or verified
for their ability to carry out certain tasks,
or who supervised their work was mostly
underreported. Compared with no in-
tervention or other alternatives, partnering
with CBHWs tended to result in increasing
screening tests for breast, cervical, and co-
lorectal cancers; decreasing blood pressure,
blood glucose, and weight; and promotion of
exercise in study samples. In several studies
reporting costs, CBHWs tended to save costs
as well. Our findings support the benefits of
working with CBHWs in promoting health
among people who are at risk for health
disparities.
April 2016, Vol 106, No. 4 AJPH Kim et al. Peer Reviewed
Systematic Review e3
AJPH RESEARCH
Vulnerable populations—defined as those“capable of being
hurt” or “susceptible
to injury or disease”1—refer to a wide range
of groups including the economically disad-
vantaged, the uninsured, racial and ethnic
minorities, the elderly and children, or those
who encounter barriers to accessing health
care.2 Their health problems often intersect
with social factors such as housing, poverty,
absence of a usual source of care, and in-
adequate education.3
7. The needs of vulnerable populations are
multifold and require extensive medical and
nonmedical outreach and services. However,
current health care financing and service de-
livery arrangements do not always address the
complexityandbreadth ofneeds.For example,
since the advent of the Patient Protection
and Affordable Care Act (ACA; Pub L No.
111–148), the rate of the uninsured dropped
initially (nearly 4%) in early 2014, but there has
been no substantial change in this statistic from
the second to the third quarter of 2014.4 In
addition, the proportion of US adults who
delay medical treatment of serious conditions
in the past year has risen since 2013 (from 19%
to 22%).5 In 2013, more than 41 million US
individuals younger than 65 years did not have
health insurance, because in large part of the
fact that they could not afford coverage.6
Compared with their insured counter-
parts, the uninsured were less likely to receive
timely preventive care within the past year
(33% vs 67% of the nonelderly with Medicaid
and 74% of nonelderly individuals with
employer-based insurance) or to have access
to appropriate follow-up care after abnormal
screening results.6 More than half (58%) of the
uninsured with a chronic illness reported that
they did not buy a prescription drug because
of cost, compared with 39% of those with
publicly funded insurance and 34% of those
with private insurance.7 Other vulnerable
populations such as the elderly or individuals
with disabilities also have high levels of unmet
8. health care needs. For example, the State of
Aging and Health in America 2013 report
revealed that only about 51% of male and 53%
of female older adults (aged ‡ 65 years) were
up to date on certain preventive care such as
influenza vaccination or colorectal cancer
screening.8 Similarly, individuals with dis-
abilities had more than 1.5-times-higher odds
of delaying care because of costs compared
with those without.9
Novel approaches to address the risks
and multiple needs of vulnerable populations
is an important public health imperative.10,11
An emerging approach is to work with
community-based health workers
(CBHWs)—indigenous public health
workers who not only share the same ethnicity,
language, or geographic community of the
patients they serve, but also share the life
experiences with target populations and
communities.12 Hence, they are uniquely aware
of the ethnic, linguistic, socioeconomic, cultural,
and experiential factors that may influence
that community’s use of health care services.13
With their unique ability to provide “bridges”
betweenthecommunityandhealthcareservices,
CBHWs play a role that could address health
inequities: culturally appropriate health educa-
tion, individual and community capacity
building, advocacy, and informal counseling
and social support in diverse settings (e.g.,
community-based organizations, community
clinics,orprimaryandemergencycarecenters).14
9. A number of systematic reviews were
published with regard to CBHW in-
terventions.15–21 Previous systematic reviews
found that CBHW interventions are effective
in promoting a wide range of healthy be-
haviors, such as breast cancer screening15;
self-management of diabetes,16–18 hyperten-
sion,19 and asthma20; and medication ad-
herence among patients with HIV/AIDS.21
Only a few reviews highlighted the additional
emphasis on the roles and training of
CBHWs, however.16–18 Furthermore, the
field is rapidly evolving with greater attention
to the synergistic effects of CBHWs as part of
patient-centered care teams. A comprehen-
sive systematic review on CBHW in-
terventions to control noncommunicable
diseases among vulnerable populations is
needed, to develop a better understanding
of integrating CBHWs into the delivery of
care to vulnerable populations.
The purpose of this article is to provide
a critical review of the evidence on CBHW
interventions. Specifically, we examined the
types of interventions in which CBHWs were
employed, the qualifications and character-
istics of CBHWs, and the patient outcomes
and cost-effectiveness of such interventions
in vulnerable populations with non-
communicable chronic conditions. We also
considered the integration of CBHWs into
the mainstream health care workforce for
both the prevention and management of
10. noncommunicable chronic diseases that
overburden vulnerable populations. Our re-
view systematically extends the previous ef-
forts by providing an understanding of (1)
how CBHWs are trained before the delivery
of an intervention, (2) how CBHWs im-
plement an assigned intervention, (3) how
CBHW interventions achieve desired effects,
and (4) how CBHWs are integrated into the
current health care system.
METHODS
We searched 4 electronic databases—
PubMed, EMBASE, Cumulative Index to
Nursing and Allied Health Literature, and
Cochrane—and conducted hand searches of
reference collections for potential studies.
Following consultation with a health science
librarian, we used a combination of keywords
that contained Medical Subject Headings
terms: “vulnerable populations,” “commu-
nity health worker,” and “randomized con-
trolled trials.” More detailed information
about search terms is given in Appendix A
(available as a supplement to the online
version of this article at http://www.ajph.
org). The searches were restricted to articles
published in peer-reviewed journals in En-
glish before August 2014 (for studies focused
on individuals with diabetes since 2011). The
ABOUT THE AUTHORS
Kyounghae Kim and Hae-Ra Han are with The Johns Hopkins
University School of Nursing, Baltimore, MD. Janet S. Choi,
Carrie L. Nieman, and Frank R. Lin are with Center on Aging
11. and Health, The Johns Hopkins University. Eunsuk Choi is
with College of Nursing and Research Institute of Nursing
Science, Kyungpook National University, Daegu, South Korea.
Carrie L. Nieman and Jin Hui Joo are with Johns Hopkins
University School of Medicine. Laura N. Gitlin is with Center
for Innovative Care in Aging, Johns Hopkins University School
of Nursing and Medicine. Hae-Ra Han is also with Center
for Cardiovascular and Chronic Care, Johns Hopkins University
School of Nursing.
Correspondence should be sent to Hae-Ra Han, RN, PhD, Johns
Hopkins University School of Nursing, 525 N Wolfe St,
Baltimore, MD 21205-2110 (e-mail: [email protected]). Reprints
can be ordered at http://www.ajph.org by clicking the
“Reprints”
link.
This article was accepted November 2, 2015.
doi: 10.2105/AJPH.2015.302987
AJPH RESEARCH
e4 Systematic Review Peer Reviewed Kim et al. AJPH April
2016, Vol 106, No. 4
http://www.ajph.org
http://www.ajph.org
mailto:[email protected]
http://www.ajph.org
hand searches involved review of reference
lists from articles obtained from the 4 elec-
tronic databases.
Study Selection Process
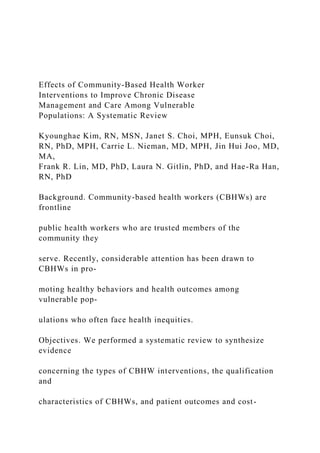
12. Figure 1 summarizes the results of the
literature search. Initially, we retrieved 922
studies from 4 electronic databases after we
discarded 575 duplicates. We obtained 12
additional studies from hand searches of
reference collections. Two reviewers in-
dependently conducted an initial screening
of titles and abstracts with relevance to
noncommunicable chronic diseases. After
screening the initial titles and abstracts, they
passed 397 abstracts onto a second review
process to exclude (1) studies focused
on children, (2) non–data-based articles (e.g.,
editorials, commentaries), and (3) studies
focused on nonvulnerable populations. Of
397 abstracts, we included 166 abstracts in
a full-text review.
Two reviewers (K. K. and B. A.) in-
dependently evaluated full-text articles to
determine whether studies met the following
inclusion criteria: (1) randomized controlled
trials published in English in peer-reviewed
journals, (2) studies testing CBHW-led in-
terventions, (3) studies focused on adults, and
(4) studies focused on chronic conditions. We
excluded 89 articles for the following reasons:
1. full texts were unavailable (i.e., con-
ference abstracts; n = 16);
2. they were nonrandomized controlled
trials (n= 55);
13. 3. studies did not include a CBHW-led
intervention (n = 6);
4. they were studies focused on diabetes
that were published before 2011, given
their inclusion in a recent systematic
PubMed: 621
EMBASE: 532
CINAHL: 165
Cochrane: 179
934 titles with abstracts
reviewed
Excluded (n = 231)
Articles focusing on children: 43
Nondatabased articles: 62
Nonintervention studies: 119
Nonvulnerable populations: 7
397 abstracts passed onto
second review process
Excluded (n = 89)
Conference abstracts: 16
Non-RCTs: 55
No CHW involvement: 6
Focusing on diabetes before 2011: 8
RCT among CHWs: 1
14. Reporting preliminary findings: 3
166 full-text articles passed
onto review process
67 full text articles selected
and included in the review
(61 primary + 6 companion
articles)
12 of additional records
identified through reference
collection
575 duplicates removed
537 of records excluded because
nonrelevant to chronic disease
FIGURE 1—Review and Selection Process for Systematic
Review of Randomized Controlled Trials on the Effect of
Community-Based Health
Workers on Chronic Disease Management and Care Among
People at Risk for Health Disparities, up to August 2014
AJPH RESEARCH
April 2016, Vol 106, No. 4 AJPH Kim et al. Peer Reviewed
Systematic Review e5
15. review on CBHWs for individuals with
diabetes (n= 8);
5. they were studies that tested the effec-
tiveness of an intervention to change
behaviors among CBHWs (n= 1); and
6. articles reported preliminary or inter-
mittent findings or reported the long-
term findings of other articles (n = 3).
We merged articles that included a cost-
effectiveness analysis only into the main outcome
studies.Discrepanciesregardingtheextracteddata
(see data extraction selection in the next para-
graph) between 2 reviewers were reconciled
based on a series of team discussions. A total of 67
articlesmetcriteriaforinclusion.Figure1provides
a detailed outline of the article selection process.
Data Extraction
Four trained research assistants (RAs)
extracted relevant data by using a standard-
ized data extraction form developed by the
authors. They extracted the following data
from the selected studies: author, year,
country, randomization, intervention unit,
setting, sample (% non-White), the method
of outcome ascertainment, time to outcome
measure, theory use, CBHW selection cri-
teria, type of training, training frequency,
training intensity, duration of training,
16. participant satisfaction, delivery approach,
control group, types of CBHW in-
tervention, measurability of the CBHWs’
effect, intervention dose, intervention in-
tensity, intervention duration, number of
participants in the study groups, mean age
and gender proportion of the study sample,
proportion of target condition or behavior
for the treatment and control groups at
baseline and follow-up, fidelity, and study
quality. Subsequently, an independent RA
reviewed extracted data to check accuracy.
Discrepancies were resolved through dis-
cussions among all RAs and authors.
We evaluated each study for its quality,
based on published quality rating scales
(Table 1).22–25 Specifically, we used the
quality rating scales published by Jadad
et al.22 and Haynes and Sackett.25 Our
quality rating scale also incorporated addi-
tional evaluation items addressing in-
tervention setting and outcome assessment
methods used in published systematic
reviews.23 The total quality rating scale
score ranged from 0 to 12 with 0 being the
lowest quality and 12 indicating the highest
quality. Based on the possible range of scores,
we categorized studies with quality ratings of
0 to 4, 5 to 8, and 9 or more as low-, medium-,
and high-quality studies, respectively. Two
RAs who extracted relevant study information
rated each study for its quality independently.
Interrater agreement statistics using percentage
agreement ranged from 61% to 91% (average
17. 86%). Any discrepancies in terms of quality
rating were resolved through team discussions.
RESULTS
There were 67 publications including 61
studies26–86 with 6 companion articles.87–92
Table 2 summarizes the key characteristics of
studies included in this review. The com-
panion articles presented cost analysis of the
main studies. All but 4 of the 67 studies were
conducted in the United States; 2 studies were
conducted in India,47,83 1 in Pakistan,68 and 1
in Taiwan.86 Ethnic minorities were the focus
of all but 4 studies, which included pre-
dominantly low-income non-Hispanic
White participants (61% to 95%) at risk for
experiencing inequality in health care access
(e.g., Appalachians).37,44,48,49 Across the 67
articles, sample sizes varied widely from 2562
to 167 915.47 Participants generally ranged in
age from 32 years42 to 71 years,82 and 28%71
to 100%26–28,31–33,35-44,46,48–55,60,64,66,80 of
participants were women.
Of 67 articles, 30 studies involved CBHWs
for cancer prevention for specific cancer
types (cervical,28,32,33,35–39,41–44,49–52
breast,26,27,31,33,36,37,39–41,46,48,50,53–55 co-
lorectal,29,30,34,36,45 and oral47). Twenty-six
studies focused on cardiovascular disease
18. (CVD),56–59,62,64,67,73,80 and key risk
factors such as diabetes,63,69,70,76–79,81 and
TABLE 1—Study Quality Ratings for Systematic Review of
Randomized Controlled Trials on
the Effect of Community-Based Health Workers on Chronic
Disease Management and Care
Among People at Risk for Health Disparities, up to August 2014
Item Score
Research questions 1 = Clearly described
0 = Not clear
Type of facility where the study was conducted 1 = Described
0 = Not described
Participant inclusion or exclusion criteria 1 = Specified
0 = Not provided
Participants in sample 1 = Clearly described
0 = Unclear
Sample size justification 1 = Provided and justified before the
study was conducted
0 = Not provided or unclear
Method of randomization 1 = Described
0 = Unclear
19. Outcome measure 1 = Claims data or chart review
0 = Self-reported data
Clarity of outcome 1 = Description of outcome was provided
0 = No definition of outcome provided
Clarity of time until outcome was measured 1 = Described
0 = Unclear
Information on withdrawal or dropout rate 1 = The number and
the reasons for withdrawal were stated
0 = Only the number described or not discussed
Analysis performed by intervention allocation status 1 = Yes
(i.e., intention to treat)
0 = No
Awareness of group assignments of outcome assessor 1 =
Unaware
0 = Aware
AJPH RESEARCH
e6 Systematic Review Peer Reviewed Kim et al. AJPH April
2016, Vol 106, No. 4
T
A
152. in
ue
d
AJPH RESEARCH
e8 Systematic Review Peer Reviewed Kim et al. AJPH April
2016, Vol 106, No. 4
T
A
B
L
E
2
—
Co
nt
in
ue
d
N
av
ar
ro
et
al
.3
9
(1
99
403. d
AJPH RESEARCH
e12 Systematic Review Peer Reviewed Kim et al. AJPH April
2016, Vol 106, No. 4
T
A
B
L
E
2
—
Co
nt
in
ue
d
C
a
rd
io
va
sc
u
la
r
d
is
e
469. m
u
n
it
y
ce
n
te
r,
an
d
ap
ar
tm
e
n
t)
.
AJPH RESEARCH
April 2016, Vol 106, No. 4 AJPH Kim et al. Peer Reviewed
Systematic Review e13
http://www.ajph.org
hypertension.61,65,68,71,72,74,75 Two studies
tested an intervention on other CVD-related
topics including promotion of physical ac-
tivity in women who have 1 or more CVD
risk factors60 and chronic disease screening
(e.g., annual examination).66 Three studies
470. tested CBHW interventions on cognitive
functioning82 and mental disorders (de-
pression84 and schizophrenia83). Finally, 2
studies involved CBHWs for asthma85 con-
trol and medication safety among rural elders
with chronic diseases.86
Forty-six (75%) studies employed
individual randomization and 14 (23%)
studies used cluster randomiza-
tion.29,33,34,36,39,47,48,54,55,58,62,63,68,82 The 2
most common types of comparison groups
were less-intensive intervention (n = 17;
28%),27,35,36,38,40,46,53,57,58,62,65–67,73,74,78,85
and usual care (n = 16; 26%)31,32,37,41,44,47,
51,55,60,64,71,72,76,77,83,86 or enhanced usual
care (n = 4; 7%)56,59,69,84 followed by
wait-list control (n = 7; 11%),42,45,48–50,63,77
and attention control (n = 3; 5%).39,52,82
Eight studies involved more than 1 com-
parison group (e.g., usual care and minimal
intervention).26,28–30,61,68,75,80 Study sites
commonly involved participants’ homes
(n = 31; 51%),28,29,32,33,36,38,40–44,52,55,56,
63,65,68,70,72,75,76,78,79,81,83,85,86 community
health clinics (n = 15; 25%),30,31,45,46,56,58,
60,61,63,64,66,73,79,84,86 community-based
organizations (n = 11; 18%),35,36,38,40,57,59,
67,69,73,77,82 and faith-based organizations
(n = 4; 7%).34,36,42,62 Some studies relied
solely on telephone contact for CBHW
interventions.27,37,53,74
471. Quality Ratings
Thirty-nine studies fell under the high-
quality category (i.e., quality scores of 9 or
higher with a maximum possible score of 12;
Table 1). Most studies clearly described the
research questions, study design, sample
characteristics, sample inclusion and exclusion
criteria, study setting, study outcomes, and
data collection timepoints. None of the
studies were considered to be low quality.
However, there were several notable meth-
odological limitations. For example, only
about half of the studies (n = 34) discussed
using a theoretical framework to develop the
intervention or from which to select study
outcomes.26–29,31–35,39,41–44,46,49,53–55,62–
65,73–80,84,85 In addition, less than one third of
the selected studies discussed conducting
a power analysis a priori (n = 21),26,29,40,42–
47,49,56,63,68,71,73,77,78,81,83–85 and about half
of the studies (n = 34)26,28,29,30,32,34,37,40–
44,46–48,51-54,56,57,59,63,65,68,69,71,74,76–
78,81,83,84 clearly described how they
randomized study participants. Similarly,
less than 1 in 4 studies discussed any
type of blinding (i.e., the outcome
assessor was aware of the status of
the participant’s group assignment;
n = 15).33,37,43,45,48,49,51,52,54,63,65,69,76,81,83
In the context of cancer screening, half of
the studies measured primary cancer screen-
ing behavior through self-report only29,34–
472. 36,38–41,48–50,53–55 as opposed to objective
chart review. Of the 7 cancer screening
studies that verified self-reported screening
behavior with chart review, discrepancies
were noted in all studies (sensitivities from
59%52 to 83%33,42 and specificities from
81%33 to 100%28). Finally, less than one third
of the studies (n = 21) described how they
maintained and monitored CBHW in-
tervention fidelity.28,32–34,37,42–44,46,47,49,51–
56,60,67,70,78
Roles and Tasks of CBHWs in
Intervention Studies
The CBHWs delivered a wide range of
interventions including education, counsel-
ing, navigation assistance, case management,
social services, and social support. These in-
terventions were often delivered in addition
to traditional outreach responsibilities of
CBHWs, which included participant re-
cruitment and data collection. The CBHW
interventions were performed in collabora-
tion with health care professionals. The
CBHWs were supervised by research staff,
clinic staff, and study psychologists (Table 2).
Fifty out of 61 interventions involved
CBHWs alone or the effect of the work of
CBHWs was tested separately, whereas in
11 studies, CBHWs partnered with other
professionals such as primary care pro-
viders,26,27,48,56,84,93 nurse case managers,63
dietitians,69,73 and social workers85 to deliver
the study intervention.
473. In 48 articles, CBHWs fulfilled the role of
an educator. The CBHWs provided educa-
tion via individual sessions or group education
sessions34–36,38–42,48,52,57,58,62,67,69,73,77,79,81
of varying sizes, from 338,41 to 2057partici-
pants (median = 3.5–11), with a duration of
intervention up to 30 months72 and each
session lasting from 5 to 10 minutes75 to
3 hours (average = 93 minutes).42,52,67 Edu-
cation sessions took place at participating
clinics, community locations, or participant’s
home or work. Varying educational mate-
rials were used, including standardized
PowerPoint presentations,34 videos,28,50,52
print education materials,50,52 and monthly
newsletters.61 In addition, role playing was
also adopted for interactive education
sessions.62
Some studies provided different types of
CBHW-led education based on the in-
dividual’s risk profile after baseline assessment.
In a study delivering a nurse–CBHW team
intervention to support diabetes self-
management in American Samoa, partici-
pants assigned to a higher-risk group attended
weekly group sessions whereas participants
assigned to moderate- or lower-risk group
were seen individually by CBHWs monthly
or at a lower frequency.63 Only 1 study re-
ported initial testing and validation of the
educational materials.28 In a study promoting
cervical cancer screening among Mexican
474. American women, Byrd et al.28 validated the
educational materials and lesson plans at 2
half-day workshops with bilingual or bi-
cultural CBHWs who had experiences
working with Mexican American women.
The CBHWs reported that the materials were
easy to use and successfully demonstrated
their ability to use lesson plans.28
In 36 articles, CBHWs delivered coun-
seling sessions to address barriers in adopting
target behaviors and to reinforce benefits of
behavior change.26,27,30–32,37,43–46,49,51–55,57–
64,66,67,72,75–77,79,81,83,85,86 The CBHWs
communicated with participants via tele-
phone calls, home visits, or regular meetings
to assess and problem-solve personal and
environmental barriers throughout the in-
tervention. In 1 study,36 CBHWs provided
theory-based scripted messages for each
barrier, including personal belief, fear, health
care provider, personal need, and manage-
ment barriers.46 In another study,65 CBHWs
delivered weekly 5 to 10 minutes of
counseling to reinforce patient lifestyle,
medication-taking, and appointment-
keeping behaviors.75
AJPH RESEARCH
e14 Systematic Review Peer Reviewed Kim et al. AJPH April
2016, Vol 106, No. 4
In 21 articles, CBHWs provided
475. navigation assistance for their study
participants in obtaining preventive care
services and managing chronic dis-
eases.27,31,33,37,38,40,41,43,45,46,49,51,62,63,70–
72,77,79,81 As navigators, CBHWs provided
information on how to access medical services
and helped with scheduling appointments at
health centers. Information on access to
medical services included availability of low-
cost or free medical services in the community,
local providers, and health insurance. In addi-
tion to appointment scheduling, CBHWs
facilitated participants’ attendance at scheduled
health services by arranging transportation and
accompanying participants to appointments.
In a study addressing cervical cancer screening
among Chinese women, CBHWs provided
transportationassistancethroughtaxicabsorbus
passes and medical interpreter services during
clinic visits for Papanicolaou (Pap) testing.51
In 4 studies, CBHWs were involved in case
management by planning and coordinating
appropriate health care services.74,77,79,83
Studies in which CBHWs provided case
management services usually addressed
chronic conditions often involving care from
multiple health professionals. In a study de-
livering a diabetes education and manage-
ment program for uninsured Mexican
Americans,77 CBHWs facilitated immediate
physician contact to address acute problems,
assisted with pharmacy refills, and arranged
specialty visits, such as dental care and dilated
retinal exam. These CBHWs were state-
476. certified health workers and they delivered
management services in the setting of an
urban community health services clinic.
In 7 articles, CBHWs assisted participants
in assessing social services in addition to
medical services.56,65,71,72,76,83,84 In these
studies, investigators attempted to address
systematic barriers preventing study partici-
pants from adopting target behaviors by
connecting them to existing social services.
The social services provided included referrals
to community transportation,71 child care,71
housing,65,76,84 legal benefits,83 and em-
ployment opportunities.65,83,84
Eighteen studies assigned CBHWs
to provide social support to promote
targeted health behaviors.27,29,
31,36,48,49,51,52,55,58,60,63,72,80,81,86 The
CBHWs directly provided support for be-
havior change by encouraging the study
participants through multiple conversations
and offering emotional support. Social support
was also offered indirectly by educating family
and friends on how to be supportive. For
example, in a study delivering an intervention
to decrease blood pressure in an urban African
American population,72 CBHWs taught family
members or friends how to provide daily
support to the patient, and also to assist with
appointment keeping or with behaviors related
to blood pressure control.
477. Effects of CBHW Interventions
The effects of CBHW interventions
reviewed are summarized in Table 2. The
findings presented in this section highlight the
effects of CBHWs as an intervention com-
ponent as long as the effect was measured
separately. Because of the heterogeneity of
settings, sample characteristics, and types of
interventions, it was not possible to conduct
a quantitative meta-analysis. Overall, most
studies reviewed reported positive outcomes
for the targeted health behavior. Eight pub-
lications including 6 companion articles also
demonstrated that the use of trained, cul-
turally competent CBHWs resulted in cost
savings.36,43,87–92
Cancer prevention. Of the 30 studies that
tested the effect of a CBHW-led intervention
on cancer control, 21 studies (70%) found
improvements in cancer screening behav-
iors.26,28,30–33,35,37,38,40–51 Positive changes in
mammogram uptake (6% to 33% increase)26,
31,37,40,41,43,46,48,50 were noted in 9 of the
16 studies that focused on breast cancer. The
trial with the largest increase in mammogram
screening (33%) employed a multifaceted
intervention designed for African American
women that included 4 monthly CBHW-led,
culturally tailored counseling sessions and
mailing of a postcard message tailored to the
participant’s barriers.46 Similarly, significant
improvements in Pap tests, ranging from 7%
to 29%,28,32,35,37,38,42,49,50,52 were reported
in 9 of the 16 studies that targeted cervical
478. cancer. Of the 3 studies focused on colorectal
cancer, only 1 yielded a significant increase in
colorectal cancer screening in the CBHW-led
education group compared with usual care
(27% vs 12%; P < .001).45
The studies without significant changes in
mammogram,27,36,53,55 Pap test,27,30,32,34 or
colorectal cancer screening21,27 tended to
compare one type of CBHW intervention to
another (e.g., education vs social support
group)27 or to a less-intensive intervention (as
opposed to no intervention).27,53 In addition,
some of these studies included a high pro-
portion of participants who were up to date
for screening41 or had significantly different
demographic characteristics between the 2
groups at baseline.55 One study44 reported
significant improvement in self-reported Pap
test use among Appalachian women (n = 286;
71% vs 54%; P = .008); however, the result
ceased to be significant when chart review
was used to ascertain the outcome (51% vs
42%; P = .135). Holt et al.34 found a sig-
nificant negative effect of spiritually based
CBHW-led intervention on fecal occult
blood testing among African Americans
compared with the nonspiritual group (2%
decrease vs 9% increase, respectively;
P = .03).
Cardiovascular disease risk reduction. Sixteen
studies (62%) included in the review found
a significant effect of CBHW intervention on
CVD risk reduction.56,58–60,62–65,68–72,77–79
479. Of the 9 studies that tested the effect of
CBHW-led intervention on global CVD
prevention, 5 (56%) studies found signifi-
cantly greater improvements in lipid profile
(total cholesterol, low-density lipopro-
tein, high-density lipoprotein, or tri-
glycerides),56,59,62 blood pressure,56,58,62,64
hemoglobin A1C (HbA1C),56 and global
CVD risk59 for the CBHW intervention
group compared with the comparison group.
Mixed or nonsignificant results were noted in
the 3 remaining studies, which might have
been attributable to a small sample size
(48–61),67,73 low statistical power,80 low
follow-up rates (67% to 73%),67,80 or
variability in fidelity of intervention
implementation.80
Of the 2 studies that focused on other
CVD-related topics,60,66 only 1 study60
found a significant improvement in self-
reported moderate (71% to 84%; P < .001)
and vigorous (13% to 33%; P < .001) physical
activity from baseline to 6-month follow-up
in the intervention group. No significant
increase was noted in the comparison group.
Of the 8 studies63,69,70,76–79,81 that ex-
clusively focused on HbA1C or fasting glu-
cose as a primary outcome, all but 276,81 found
significant improvements in diabetes control.
Tang et al.81 compared the effect of peer
480. AJPH RESEARCH
April 2016, Vol 106, No. 4 AJPH Kim et al. Peer Reviewed
Systematic Review e15
leaders (bilingual residents in the target
community with diabetes and aged ‡ 21
years) versus CBHWs on diabetes manage-
ment. In the study,81 the peer leader group
had a significant reduction in HbA1C at
18-month follow-up (–0.6% from baseline;
P = .009). By contrast, the CBHW group
failed to maintain an HbA1C reduction
(–0.3% from baseline; P = .234).
Eight studies examined CBHW in-
terventions for better blood pressure control.
Significant improvements in blood pressure
control were seen in 4 studies.65,68,71,72 Of the
4 studies that found nonsignificant re-
sults,57,61,74,75 2 lacked statistical power.57,61
Mental disorders, asthma control, and med-
ication safety. Three studies involved CBHWs
to address issues related to cognitive func-
tioning and mental disorders, such as de-
pression and schizophrenia82–84; the study
results were mixed. With data collected from
a cluster randomized trial94 designed to test
the effect of a weight-loss intervention for
obese older adults (‡ 60 years) whowere using
cognitive training as an attention control,
Beck et al.82 compared a cognitive training
intervention to a weight-loss intervention.
481. Participants in the intervention group had
about 3 times higher odds of achieving better
cognitive functioning compared with those in
the attention control (weight-loss) group
(odds ratio = 2.7; 95% confidence inter-
val = 1.3, 5.6; P = .011).82 Two studies that
focused on mental disorders yielded partially
significant83 or nonsignificant findings.84
Chatterjee et al.83 found a significant decrease
in disability from schizophrenia (P = .01) but
not in symptom severity. In the study84 that
tested a CBHW intervention on depression,
the authors argued that nonsignificant find-
ings might have been associated with fidelity
issues, instead of an ineffective intervention.
One study tested the effect of CBHW
intervention on asthma control and found
that the intervention was effective in pro-
moting self-efficacy; however, there was no
significant difference in clinical outcomes
(e.g., symptomatic days and nights over the
past 14 days) between groups.85 However,
the authors reported that this study was un-
derpowered to detect self-management in
asthma control and clinical outcomes. In
a study86 that tested the effect of a volun-
teer coaching on medication safety in
community-dwelling elders with 2 or more
chronic illnesses, the volunteer coaching
program was effective in promoting medi-
cation safety knowledge as well as 3 (out of 6)
medication safety behaviors, compared with
the usual care.
482. Cost outcomes. Eight out of 61 studies
(13%) included cost analyses. Of the 8 articles
with cost analyses, 3 studies focused on di-
abetes control,88 high blood pressure con-
trol,91 and cardiovascular risk reduction.87
Lawlor et al.88 found that a lifestyle in-
tervention delivered by a registered dietitian–
CBHW group could be cost-effective. In the
study, estimated direct medical costs per
capita were $850 and $142 for the registered
dietitian–CBHW and the registered dietitian
groups, respectively. When total costs were
calculated, however, it was higher for the
registered dietitian–only group than for the
registered dietitian–CBHW group ($7596 vs
$6027, respectively). In a study tolower blood
pressure in 12 randomly selected communi-
ties in Pakistan,91 Jafar et al. found that
a “home health education by CBHWs plus
trained general practitioner” intervention was
the most cost-effective intervention com-
pared with “home health education only,”
“general practitioner only,” and “usual care”
interventions. The combined intervention
resulted in an incremental cost-effectiveness
ratio (ICER) of $23 (95% confidence
interval = 6%, 99%) per millimeter of
mercury (mm Hg) systolic blood pressure
reduction compared with the usual-care
group.91 In a CVD risk reduction program
delivered by nurse practitioner (NP)–CBHW
teams in urban community health centers,87
Allen et al. also reported estimated savings of
483. $157 and $190 per 1% reduction in systolic
and diastolic blood pressure, respectively.
They also reported an ICER of $149 for
1% reduction in HbA1C and $40 for 1%
reduction in low-density lipoprotein
cholesterol.
Five studies assessed cost-effectiveness of
CBHW intervention in the context of cancer
screening. A CBHW intervention designed
to promote cervical cancer screening among
Vietnamese American women resulted in an
ICER of $30 015 per quality-adjusted life
year.89 In a study that tested the effect of
a CBHW-facilitated AMIGAS (Ayudando
a Las Mujeres con Información, Guía y Amor para
su Salud: Helping Women with Information,
Guidance, and Love for Their Health, in
English) program (video, flipchart, or both)
among nonadherent Mexican-origin women
aged 21 years and older, Lairson et al.92 re-
ported an ICER of $980 per additional
women screened compared with a video-only
intervention and wait-list control. Wagner
et al.90 conducted a CBHW outreach program
for low-income women with abnormal Pap
test results in Alameda, California, and ob-
tained an ICER of $959 per follow-up for the
intervention compared with usual care. Al-
though Larkey et al.36 found no difference in
cancer screening outcomes between in-
terventionandcomparison groups,thecostper
participant screenedwas approximately3 times
greaterintheindividuallydeliveredgroupthan
in the social support group ($1716.22 vs
484. $516.53, respectively). Paskett et al.43 esti-
mated a cost associated with CBHW in-
tervention to promote mammography
screening among low-income, ethnically di-
verse female patients aged 40 years or older,
which equated to a cost savings of $4986 per
each mammogram in the CBHW group.
Qualifications and Characteristics
of CBHWs
Identification and selection of community-
based health workers. The characteristics,
training, and roles of CBHWs are summarized
in Table 3. Studies widely varied in their
approaches to identifying CBHWs. Ap-
proaches included identification by com-
munity leaders,29,34,86 use of existing
CBHWs in the community,30,45 use of par-
ticipating churches49 or a community self-
help organization,50 or community members
who demonstrated the positive behavior
targeted within the study population.26
Studies also used different selection cri-
teria. Twenty-five studies used living in
the same residential area with the study
participants as a CBHW selection crite-
rion.27,31,35,40,44,47–50,53–55,60,62,64,66,69,70,77–
81,84,86
All studies targeting racial/ethnic
minorities included bilingual CBHWs.28,
36,45,52,60,64,66,67,77,78,81,84 Three studies
selected CBHWs on the basis of their similar
background to the study population in
485. terms of marital status, age, socioeconomic
status, occupation, or having children.35,49,52
Some studies selected CBHWs on the basis of
their educational level31,45,47,60 or having
previous experiences working with the
AJPH RESEARCH
e16 Systematic Review Peer Reviewed Kim et al. AJPH April
2016, Vol 106, No. 4
T
A
B
L
E
3
—
C
h
ar
a
ct
e
ri
st
ic
s,
T
ra
in