
Recommended
More Related Content
Similar to UVA GI Cynthia Philip.pptx
Similar to UVA GI Cynthia Philip.pptx (20)
Recently uploaded
Recently uploaded (20)
UVA GI Cynthia Philip.pptx
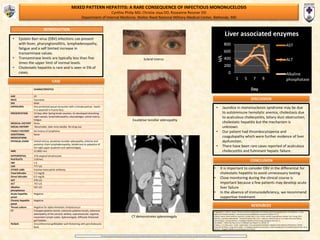
- 1. MIXED PATTERN HEPATITIS: A RARE CONSEQUENCE OF INFECTIOUS MONONUCELOSIS Cynthia Philip MD, Christie Joya DO, Roseanne Ressner DO Department of Internal Medicine; Walter Reed National Military Medical Center, Bethesda, MD INTRODUCTION RESOURCES CONCLUSION DISCUSSION “The views expressedin this presentationare thoseof the authorsand do notreflectthe official policy or position of the Departmentof the Army, the Departmentof the Navy, the Departmentof Defense, nor the USGovernment.” 1) Agergaard, J., and C.s. Larsen. "Acute Acalculous Cholecystitis in a Patient with PrimaryEpstein-Barr Virus Infection: A Case Report and Literature Review." International Journal ofInfectious Diseases 35 (2015): 67-72. 2) Busch, Daniel, Sarah Hilswicht, Dominik S. Schöb, Klaus T Von Trotha, Karsten Junge,Nikolaus Gassler, Son Truong, Ulf P. Neumann, and Marcel Binnebösel. "Fulminant Epstein-Barr Virus - Infectious Mononucleosis in an Adult with Liver Failure, SplenicRupture, and Spontaneous Esophageal Bleeding with Ensuing Esophageal Necrosis: A Case Report." J Med Case Rep Journal of Medical Case Reports 8.1 (2014): 35. 3) Salva, I., I. V. Silva, and F. Cunha. "Epstein-Barr Virus-associated Cholestatic Hepatitis."Case Reports 2013.Dec16 1 (2013). 4) Tan, Zh, Kb Phua, C. Ong, and A. Kader. "Prolonged Hepatitis and Jaundice: A Rare Complication of Paediatric Epstein-Barr Virus Infection." Singapore Medical Journal Smedj 56.07 (2015). • It is important to consider EBV in the differential for cholestatic hepatitis to avoid unnecessary testing • Close monitoring during the clinical course is important because a few patients may develop acute liver failure • In the absence of immunodeficiency, we recommend supportive treatment. CASE 0 200 400 600 800 1 5 7 9 U/L Day Liver associated enzymes AST ALT Alkaline phosphatase • Epstein Barr virus (EBV) infections can present with fever, pharyngtonsillitis, lymphadenopathy, fatigue and a self limited increase in transaminase values. • Transaminase levels are typically less than five times the upper limit of normal levels. • Cholestatic hepatitis is rare and is seen in 5% of cases. • Jaundice in mononucleosis syndrome may be due to autoimmune hemolytic anemia, cholestasis due to acalculous cholecystitis, biliary duct obstruction, cholestatic hepatitis but the mechanism is unknown. • Our patient had thrombocytopenia and coagulopathy which were further evidence of liver dysfunction. • There have been rare cases reported of acalculous cholecystitis and fulminant hepatic failure. CHARACTERISTICS AGE 20 RACE Caucasian SEX Male EXPOSURES One protected sexual encounter with a female partner. Swam in a waterfall in Puerto Rico. PRESENTATION 10 days after Spring break vacation, he developed drenching night sweats, lymphadenopathy, odynophagia, scleral icterus, fatigue. MEDICAL HISTORY None SOCIAL HISTORY Nonsmoker, beer once weekly. No drug use. FAMILY HISTORY No history of lymphoma ADDITIONAL MEDICATIONS None PHYSICAL EXAM Scleral icterus, exudative tonsillar adenopathy, anterior and posterior chain lymphadenopathy, tenderness to palpation of the right upper quadrant and splenomegaly. WBC 21,000/ mcL DIFFERENTIAL 21% atypical lymphocytes PLATELETS 119/mcL INR 1.6 LDH 777 U/L OTHER LABS Positive heterophile antibody Total bilirubin 7.2 mg/dL Direct bilirubin 6.5 mg/dL AST 478 U/L ALT 755 U/L Alkaline phosphatase 501 U/L Acute hepatitis panel Negative Chronic hepatitis panel Negative Throat culture Negative for alpha hemolytic streptococcus CT Enlarged palatine tonsils, extensive palatine tonsils, extensive adenopathy of the cervical, axillary, supraclavicular, inguinal, mesenteric lymph nodes. Splenomegaly. Diffusely thickened gall bladder. RUQUS Circumferential gallbladder wall thickening with pericholecystic fluid. Scleral icterus Exudative tonsillar adenopathy CT demonstrates splenomegaly