ASCO-GI; Performance of 18-FDG-PET in the management of non-metastatic HIV+ anal squamous cell carcinoma (ASCC)

Presented at the 2017 American Society for Clinical Oncology Gastroenterology in San Francisco - January 21st 2017 Background: ASCC remains rare, but the incidence has been increasing over the last decade, especially in patients with HIV infection (HIV+). A recent meta-analysis demonstrated the usefulness of 18FDG-PET in initial staging and response assessment in ASCC. HIV+ patients may develop opportunistic infections which can cause false positives lymph nodes on Pet scanning and, therefore, our objective was to evaluate performance of 18FDG-PET in HIV+ patients. Patients and Methods: Retrospective analysis of consecutive patients with non-metastatic ASCC, treated in our institution during six years. HIV+ patients were analyzed separately in two groups, group 1 (Gr1): N0, group 2 (Gr2): N1,N2,N3. Results: A total of 87 patients with ASCC were analyzed, including 24 HIV+ patients (21 males, median age was 53 for male and 50 for women). There were 15 patients in Gr1 and 9 in Gr2. All patients performed conventional imaging (MRI and CT-scan). In Gr1, 12/15 patients had FDG-PET, it resulted in upstaging nodal disease in 2 patients. In Gr 2, 6/9 patients had FDG-PET, it resulted in upstaging nodal disease in 1 patient and down staging nodal disease in 2 patients. Both of sensibility and specificity of FDG-PET were 83% in our HIV+ population. All patients underwent Mitomycine C/5FU based chemoradiation or exclusive radiation therapy. Mean radiation dose received was 63.3Gy in G1 and 63.9Gy in G2. 18FDG-PET drive a modification in treatment strategy in only 1 patient in both of groups. Post-treatment PET scan was performed 4 months after treatment completion. Among patients who had post-treatment 18FDG-PET, a metabolic complete response was observed in 6/11 patients in Gr 1 and 3/5 patients in Gr 2. Survival at 5 years was 89% and 75% in Gr1 and Gr2, respectively. Conclusion: Based on our experience, 18FDG-PET nether drives substantial changes in staging nor in therapeutic strategy for ASCC HIV+ patients.
Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (11)
Similar to ASCO-GI; Performance of 18-FDG-PET in the management of non-metastatic HIV+ anal squamous cell carcinoma (ASCC)
Similar to ASCO-GI; Performance of 18-FDG-PET in the management of non-metastatic HIV+ anal squamous cell carcinoma (ASCC) (20)
More from Prof. Eric Raymond Oncologie Medicale
More from Prof. Eric Raymond Oncologie Medicale (20)
Recently uploaded
Recently uploaded (20)
ASCO-GI; Performance of 18-FDG-PET in the management of non-metastatic HIV+ anal squamous cell carcinoma (ASCC)
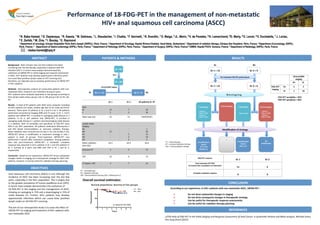
- 1. Performance of 18-‐FDG-‐PET in the management of non-‐metasta8c HIV+ anal squamous cell carcinoma (ASCC) 1 N. Baba Hamed, 2 G. Deplanque, 1 R. Kassis, 1 M. Gatineau, 1 L. Staudacher, 1 I. Chaiba, 1 F. Savinelli, 1 R. Sverdlin, 1 O. Maiga, 3 JL. Marin, 4 V. de Parades, 4 N. Lemarchand, 5O. Marty, 5 D. Levoir, 6 V. Duchatelle, 7 J. Loriau, 8 E. Zerbib, 9 M. Zins, 9 I. Boulay, 1 E. Raymond 1 Department of oncology, Groupe Hospitalier Paris Saint Joseph (GHPSJ), Paris, France; 2 Department of Oncology, Hopital Riviera-Chablais, Vaud-Valais, Switzerland; 3 Department of radiation therapy, Clinique Des Peupliers, Paris, France; 4 Department of proctology, GHPSJ, Paris, France; 5 Department of Gastro-enterology GHPSJ, Paris, France; 6 Department of Pathology GHPSJ, Paris, France; 7 Department of Surgery, GHPSJ, Paris, France;8 CIMEN, Hopital FOCH, Suresne, France, 9 Department of Radiology, GHPSJ, Paris, France : nbaba-hamed@hpsj.fr N = 87 N = 24 Gr 2 = 9 Gr 1 = 15 HIV + Clinical/MRI staging Gr 1 Gr 2 All pa8ents N= 87 Sexe M F 14 1 7 2 34 53 Mean age (yo) 56 53 54(M)/65(F) Lymph nodes staging Nx N0 N1 N2 N3 -‐ 15 -‐ -‐ -‐ -‐ -‐ 5 2 2 1 56 15 10 5 Mean radia<on dose (Gy) 63.3 63.9 63.6 Exclusive RT 5 0 15 CRT 10 9 72 CT before CRT 3 7 21 Gr 2 = 9 Gr 1 = 15 Gr 2 = 6 Gr 1 = 12 Pre treatment FDG-‐PET performance 2 Downstaging : -‐ Pa8ent 1 : T3N1 à T3N0 -‐ Pa8ent 2 : T3N3 à T3N2 Clinical/MRI staging N+ N-‐ FDG-‐PET staging N+ 5 2 N-‐ 1 10 FDG-‐PET sensibility = 83% FDG-‐PET specificity = 83% Survival proportions: Survival of Two groups 0 1 2 3 4 5 6 7 0 50 100 Years Percentsurvival VIH+ VIH- p-value=0.44 (NS) 1 Upstaging : T3N1 à T3N3 0 Downstaging 2 Upstaging : -‐ Pa8ent 1 : T2N0 à T2N2 -‐ Pa8ent 2 : T2N0 to T2N1 R e s t a g i n g No modifica8on 1 modifica8on : Switch CRT to CT _ 1 modifica8on : Switch RT to CRT (Pa8ent 1) Modifica8on of strategy CT = chemotherapy RT = exclusive Radia<on therapy CRT = Chemoradia<on therapy N+ N-‐ N-‐ N+ (1)The Role of FDG-‐PET in the Ini<al Staging and Response Assessment of Anal Cancer: A Systema<c Review and Meta-‐analysis. Michael Jones; Ann Surg Oncol (2015) FDG-‐PET response Gr 1 Gr 2 Post treatment PET-‐FDG (4 months aZer comple8on of treatment) 11 5 Complete metabolic response 6 3 CT = chemotherapy RT = Radia<on therapy CRT : Chemoradia<on therapy (5FU + Mitomycine C) Anal squamous cell carcinoma (ASCC) is rare although the incidence of ASCC has been increasing over the last few years, especially in the HIV+ populaPon. This is largely due to the greater prevalence of human papilloma virus (HPV). A recent meta analysis demonstrates the usefulness of 18 FDG-‐PET in the staging and the management of ASCC, showing an upstaging in 15% and a downstaging in 15% of nodal diseases (1). Further, HIV+ paPents may develop opportunisPc infecPons which can cause false posiPves lymph nodes on 18 FDG-‐PET scanning. The aim of our retrospecPve study is to asses the effect of 18FDG-‐PET on staging and treatment of HIV+ paPents with non metastaPc ASCC Overall survival es8mates: ABSTRACT Background : ASCC remains rare, but the incidence has been increasing over the last decade, especially in paPents with HIV infecPon (HIV+). A recent meta-‐analysis demonstrated the usefulness of 18FDG-‐PET in iniPal staging and response assessment in ASCC. HIV+ paPents may develop opportunisPc infecPons which can cause false posiPves lymph nodes on PET scanning and, therefore, our objecPve was to evaluate performance of 18FDG-‐PET in HIV+ paPents. Methods : RetrospecPve analysis of consecuPve paPents with non-‐ metastaPc ASCC, treated in our insPtuPon during six years. HIV+ paPents were analyzed separately in two groups according to their lymph nodes status, group 1 (Gr 1): N0, group 2 (Gr 2): N1, N2, N3. Results : A total of 87 paPents with ASCC were analyzed, including 24 HIV+ paPents (21 males, median age was 53 for male and 50 for women). There were 15 paPents in Gr 1 and 9 in Gr 2. All paPents performed convenPonal imaging (MRI and CT-‐scan). In Gr 1, 12/15 paPents had 18FDG-‐PET, it resulted in upstaging nodal disease in 2 paPents. In Gr 2, 6/9 paPents had 18FDG-‐PET, it resulted in upstaging nodal disease in 1 paPent and downstaging nodal disease in 2 paPents. Both of sensibility and specificity of FDG-‐PET were 83% in our HIV+ populaPon. All paPents underwent Mitomycine C and 5FU based chemoradiaPon or exclusive radiaPon therapy. Mean radiaPon dose received was 63.3Gy in G1 and 63.9Gy in G2. 18FDG-‐PET drives a modificaPon in treatment strategy in only 1 paPent in both of groups. Post-‐treatment 18FDG-‐PET was performed 4 months aber treatment complePon. Among paPents who had post-‐treatment 18FDG-‐PET, a metabolic complete response was observed in 6/11 paPents in Gr 1 and 3/5 paPents in Gr 2. Survival at 5 years was 89% and 75% in Gr 1 and Gr 2, respecPvely. Conclusion : Based on our experience, 18FDG-‐PET drives substanPal changes neither in staging nor in therapeuPc strategy for ASCC HIV+ paPents, however, it may be useful for radiaPon therapy planning. RESULTS PATIENTS & METHODS REFERENCES CONCLUSION According to our experience, in HIV+ pa8ents with non metasta8c ASCC, 18FDG-‐PET : Ø Do not drive substan8al changes in staging Ø Do not drive consequent changes in therapeu8c strategy Ø Can be useful for therapeu8c response assessments Ø Can be useful for radia8on therapy planning OBJECTIVES