Call Girls In {{Connaught Place Delhi}}96679@38988 Indian Russian High Profil...
Leishmaniasis (2).ppt
1.
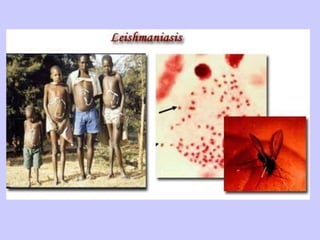
2. Leishmaniasis is a parasitic disease caused by the
protozoa belonging to the genus, Leishmania .
Human leishmaniasis is not a disease, but a group of diseases.
While several ways to classify leishmaniasis (eg, by
geography or taxonomy) are available, clinically, it can present
itself in various ways, and is more easily classified as
cutaneous, mucocutaneous, and visceral leishmaniasis.
4. Species, Reservoirs, and Clinical Diseases
Clinical Disease Leishmaniasis Species (Possible
reservoir)
Geographic Location
Cutaneous
leishmaniasis
L. tropica complex
L. tropica (dog)
L. aethiopica (rock hyrax)
L. major (gerbils & rodents)
Old World
L. mexicana complex
L. mexicana (woodrats, cat, and
others)
L. pifanoi
L. amazonensis (small forest
mammals, rodents, marsupials, and
foxes)
L. garnhami
L. venezuelensis
New World
L. braziliensis complex
L. peruviana (domestic dog and
probably a wild rodent)
L. guyanensis (arboreal sloths and
anteaters)
L. panamensis (sloths, rodents,
monkeys, procyonids)
L. lainsoni (agouti)
L. colombiensis (sloth)
New World
5. Cutaneous
leishmaniasis
L. infantum Old World
L. chagasi New World
Mucocutaneous
leishmaniasis
L. braziliensis complex
L. braziliensis
L. guyanensis
L. panamensis
New World
L. mexicana New World
L. tropica Old World
L. major Old World
Species, Reservoirs, and Clinical Diseases
6. Species, Reservoirs, and Clinical Diseases
Visceral leishmaniasis L. donovani complex
L. donovani (no
reservoir in Indian or
Kenyan area, various
rodents in Sudan , dogs
in China )
L. infantum (human is
accidental host, natural
infection in dogs, other
Canidae, and
porcupines)
Old World
Old World
L. chagasi (domestic
dogs and cats, foxes)
New World
L. tropica Old World
L. amazonensis New World
7. • During blood meal, infected sandflies inject the infective stage,
the so-called promastigote parasite, into the human host.
• Injected promastigotes are first phagocytized by macrophages
and transform into so-called amastigote parasites.
• These multiply in the infected cells and also affect different
tissues, depending on the Leishmania species, which causes
the corresponding clinical manifestation of the disease.
8. • When sandflies take blood meals from an infected host,
they take up parasitized macrophages.
• In the vector fly's midgut, these parasites differentiate
into the so-called promastigote form, which multiplies
and finally migrates to the fly's proboscis.
11. Epidemiology
• The species of visceral
leishmaniasis are endemic in
areas of India, China, Central
and South America, East and
West Africa, and the countries
surrounding the Mediterranean.
• In India, no extrahuman
reservoirs are known, but in
other regions, infection may
involve several mammalian
species, including dogs, foxes,
and wild rodents.
• Sandflies of the genus
Phlebotomus are the insect
vectors that spread L.
donovani.
12. Pathogenesis
• The flagellated promastigotes of L. donovani are
introduced by an insect bite.
• After entering macrophages of the
reticuloendothelial system, these forms change
into amastigotes, which multiply in phagocytic
cells.
• Released amastigotes disseminate
hematogenously and invade reticuloendothelial
cells in the spleen, liver, lymph nodes, bone
marrow, and skin.
13. Incubation and Clinical Symptoms
• Incubation period is 6-8 months.
Symptoms:
• weakness, dizziness, weight
loss, diarrhea, and
constipation.
• Fever, may spike twice daily;
• chills and sweating.
• hepatosplenomegaly
• anemia and leukopenia.
• bleeding from the gingivae,
nose, or GI tract,
• ecchymoses and petechiae on
the skin.
14.
15. Cutaneous and Mucocutaneous Leishmaniasis
Etiology and Epidemiology
Old World cutaneous leishmaniasis is
caused by three species of Leishmania
that belong to the L. tropica complex:
L. tropica is present in the Middle East
and the Mediterranean littoral;
L. major is found in the Middle East,
Arabia, India, and sub-Saharan Africa;
L. aethiopica is found principally in
Ethiopia and Kenya.
Phlebotomus sandflies are the
principal vectors.
• Infections that are caused by
Leishmania can be acquired by
travelers, as well as by military and other
personnel residing in endemic areas.
• Military personnel in the Middle East
have acquired cutaneous leishmaniasis
with L. major and viscerotropic
infections with L. tropica.
16. Cutaneous and Mucocutaneous Leishmaniasis
• New World cutaneous leishmaniasis arises from infection with
parasites belonging to the L. mexicana group or the L.
braziliensis (Viannia subgenus) group.
• The patterns of illness vary with the nature of the infecting
leishmanial organisms, which are found in different regions of
North, Central, and South America.
• Infections with strains of L. viannia, which are endemic in
various areas of South America, cause cutaneous
leishmaniasis and, in a small percentage of those infected,
result in the later development of mucocutaneous
leishmaniasis. Such mucocutaneous disease (espundia)
involves the nasal or oropharyngeal mucosa, or both, and may
prove fatal.
• All of these New World leishmanial parasites are transmitted
principally by sandfly vectors, although direct human contact
may also bring about infection.
• Various mammals are naturally infected reservoirs of the
organisms.
17. Pathogenesis
• Both Old World and New World forms of
leishmaniasis are initiated when the bite of an
infected sandfly injects promastigotes into the
human host.
• The organisms enter tissue macrophages and
capillary endothelial cells, become amastigotes,
and multiply.
• A granulomatous inflammatory response
develops at the bite site.
• With local ischemia, the lesion ulcerates; a
bacterial infection of the necrotic area may
extend the ulceration.
18. Incubation and Clinical Symptoms
Incubation period is from 2-8
months to 1,5 years and more.
In Old World symptoms of
cutaneous leishmaniasis:
• a papule (at the inoculation
site).
• papule ulcerates and a shallow
circular lesion appears that is
several centimeters in diameter
and has a raised margin.
• lymphadenopathy.
• Healing of the lesions is slow,
sometimes requiring more than
a year.
19. Clinical Symptoms of New World
leishmaniasis
L. mexicana
• single lesion or a few lesions on
exposed surfaces of the body such
as the face and ear, which heals
spontaneously over 6 months.
• extensive destruction of the pinna.
L. viannia
• lesions on the skin or mucous
membranes.
• progressive ulcerations of
lymphatic nodes and mucous
membranes.
• the infection metastasizes to
the nasal or oral mucosa.
• Metastatic lesions can erode
the nasal septum or the hard
palate or soft palate.
• Some patients die of
malnutrition or bacterial
infection.
Incubation period is 2-3 weeks to 1-3 mounths.
20.
21.
22. Immunity
• In visceral leishmaniasis (Kala-Azar) cellular
immunity is responsible for resolving mild
disease. High levels of antibodies are found.
• In cutaneous and mucocutaneous leishmaniasis
host defense relies on cell-mediated immunity;
antibody titers are low. The response ranges
from a local granuloma with few parasites to a
histiocytoma with many parasites.
23. Laboratory Diagnostics of visceral
leishmaniasis
• Demonstration of the organism in host tissues cultured
on a Novy-MacNeal-Nicolle (NNN) or other medium or
detection of Leishman-Donovan bodies (amastigotes) in
stained tissue samples.
• PCR can be performed using genus- or species-specific
oligonucleotides.
• Established by examining bone marrow aspirates.
• Splenic aspirates have the highest yields but may be
risky.
• Liver biopsy or aspiration of enlarged lymph nodes can
also provide diagnostic material.
24. Laboratory Diagnostics of cutaneous and
mucocutaneous leishmaniasis
• Demonstrating amastigotes on
stained smears of a biopsy or of
scrapings from the border of an
ulcer.
• Culturing amastigotes on NNN
medium inoculated with lesion
material.
• PCR targeting parasite kinetoplast
DNA has allowed detection of
organisms that might be missed
on histologic section or culturing.
25. Laboratory Diagnostics of cutaneous and
mucocutaneous leishmaniasis
• Except in diffuse cutaneous
leishmaniasis, the
leishmanin skin test is
usually positive.
26. Treatment
• There are two common therapies containing antimony,
meglumine antimoniate (Glucantim®) and sodium
stibogluconate (Pentostam®). Unfortunately, in many
parts of the world, the parasite has become resistant to
antimony and for visceral or mucocutaneous
leishmaniasis, amphotericin is now the treatment of
choice.
• Miltefosine (Impavido®), is a new drug for visceral,
mucocutaneous and cutaneous leishmaniasis.
• Drug-resistant leishmaniasis may respond to
immunotherapy (inoculation with parasite antigens plus
an adjuvant) which aims to stimulate the body's own
immune system to kill the parasite.
27. Prevention:
• Preventing sandfly bites is the
most immediate form of
protection. Insect repellent,
appropriate clothing, screening
of windows, and fine mesh
netting around the bed (in
endemic areas) will reduce
exposure.
• Public health measures to
reduce the sandfly population
and animal reservoirs are
important. There are no
preventive vaccines or drugs for
leishmaniasis.