On the Cusp of the Era of Immuno-Oncology in Triple-Negative Breast Cancer: Rational Strategies to Make the Most of Immunotherapies and Other Effective Treatment Modalities Throughout the Disease Continuum
•
3 likes•390 views

Professor Peter Schmid, FRCP, MD, PhD, Leisha A. Emens, MD, PhD, and Heather L. McArthur, MD, MPH, prepared useful practice aids pertaining to the role of immunotherapy in triple-negative breast cancer for this CME/MOC/CNE activity titled, "On the Cusp of the Era of Immuno-Oncology in Triple-Negative Breast Cancer: Rational Strategies to Make the Most of Immunotherapies and Other Effective Treatment Modalities Throughout the Disease Continuum." For the full presentation, monograph, complete CME/MOC/CNE information, and to apply for credit, please visit us at http://bit.ly/34aGu95. CME/MOC/CNE credit will be available until December 29, 2020.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to On the Cusp of the Era of Immuno-Oncology in Triple-Negative Breast Cancer: Rational Strategies to Make the Most of Immunotherapies and Other Effective Treatment Modalities Throughout the Disease Continuum
Similar to On the Cusp of the Era of Immuno-Oncology in Triple-Negative Breast Cancer: Rational Strategies to Make the Most of Immunotherapies and Other Effective Treatment Modalities Throughout the Disease Continuum (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
On the Cusp of the Era of Immuno-Oncology in Triple-Negative Breast Cancer: Rational Strategies to Make the Most of Immunotherapies and Other Effective Treatment Modalities Throughout the Disease Continuum
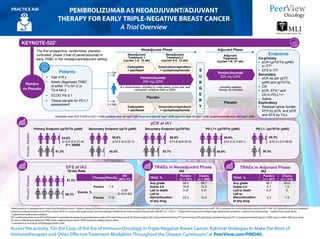
- 1. a Must consist of ≥2 separate tumor cores from the primary tumor. b Patients without pCR data for any reason or who received neoadjuvant chemotherapy not specified in the protocol were counted as non-pCR. c PD-L1 assessed at a central laboratory using the PD-L1 IHC 22C3 pharmDx assay and measured using the combined positive score (CPS); number of PD-L1+ tumor cells, lymphocytes, and macrophages divided by the total number of tumor cells x100; PD-L1+ = CPS ≥1. d 1 patient from sepsis and multiple organ dysfunction syndrome; 1 patient from pneumonitis. e 1 patient from septic shock. f 1 patient from pulmonary embolism. CPS: combined positive score; ECOG PS: Eastern Cooperative Oncology Group performance status; EFS: event-free survival; IA: interim analysis; IHC: immunohistochemistry; ITT: intent to treat; pCR: pathologic complete response; PD-L1: programmed death ligand-1; Q3W: every 3 weeks; QW: every week; TIL: tumor-infiltrating lymphocyte; TNBC: triple-negative breast cancer; TRAE: treatment-related adverse effect. 1. Schmid P et al. AnnOncol. 2019;30(suppl 5):v851-v934. Access the activity,“On the Cusp of the Era of Immuno-Oncology in Triple-Negative Breast Cancer: Rational Strategies to Make the Most of Immunotherapies and Other Effective Treatment Modalities Throughout the Disease Continuum,”at PeerView.com/PMD40. PEMBROLIZUMAB AS NEOADJUVANT/ADJUVANT THERAPY FOR EARLY TRIPLE-NEGATIVE BREAST CANCER A Trial Overview PRACTICE AID KEYNOTE-5221 The first prospective, randomized, placebo- controlled, phase 3 trial of pembrolizumab in early TNBC in the neoadjuvant/adjuvant setting • Age ≥18 y • Newly diagnosed TNBC of either T1c N1-2 or T2-4 N0-2 • ECOG PS 0-1 • Tissue sample for PD-L1 assessmenta Patients Pembrolizumab 200 mg Q3W Placebo 2:1 randomization stratified by nodal status, tumor size, and carboplatin schedule (QW vs Q3W) Neoadjuvant Phase Adjuvant Phase Neoadjuvant Treatment 1 (cycles 1-4; 12 wk) Neoadjuvant Treatment 2 (cycles 5-8; 12 wk) Adjuvant Treatment (cycles 1-9; 27 wk) Carboplatin + paclitaxel Carboplatin dose: AUC 5 Q3W or AUC 1.5 QW; paclitaxel dose: 80 mg/m2 QW; doxorubicin dose:60 mg/m2 Q3W; epirubicin dose: 90 mg/m2 Q3W; cyclophosphamide dose: 600 mg/m2 Q3W Doxorubicin/epirubicin + cyclophosphamide Carboplatin + paclitaxel Doxorubicin/epirubicin + cyclophosphamide S U R G E R Y Pembrolizumab 200 mg Q3W Placebo Including radiation therapy as indicated Pembro vs Placebo Endpoints Co-primary • pCR (ypT0/Tis ypN0) in ITTb • EFS in ITT Secondary • pCR as per ypT0 ypN0 and ypT0/Tis • OS • pCR, EFS,b and OS in PD-L1+c • Safety Exploratory • Residual cancer burden, EFS by pCR, and pCR and EFS by TILs pCR at IA1 Primary Endpoint (ypT0/Tis ypN0) Secondary Endpoint (ypT0 ypN0) Secondary Endpoint (ypT0/Tis) PD-L1+ (ypT0/Tis ypN0) PD-L1- (ypT0/Tis ypN0) 64.8% 51.2% 13.6 (5.4-21.8) P = .00055 59.9% 45.3% 14.5 (6.2-22.7) 68.6% 53.7% 14.8 (6.8-23.0) 68.9% 54.9% 45.3% 30.3% 14.2 (5.3-23.1) 18.3 (-3.3-36.8) PembroPlacebo EFS at IA2 18-mo Rate 91.3% 85.3% PembroPlacebo Therapy Results HR (95% CI) Events, % Pembro 7.4 0.63 (0.43-0.93) Placebo 11.8 TRAE, % Pembro (n = 781) Chemo (n = 389) Any grade 99.0 99.7 Grade 3-5 76.8 72.2 Led to death 0.3d 0.3e Led to discontinuation of any drug 23.3 12.3 n = 784 n = 390 TRAEs in Neoadjuvant Phase IA2 TRAEs in Adjuvant Phase IA2 TRAE, % Pembro (n = 547) Chemo (n = 314) Any grade 48.1 43.0 Grade 3-5 5.7 1.9 Led to death 0.2f 0 Led to discontinuation of any drug 3.3 1.3
- 2. a Centrally evaluated per VENTANA PD-L1 (SP142) IHC assay (double blinded for PD-L1 status); positive = ≥1%; negative = <1%. b Radiological endpoints were investigator assessed per RECIST v1.1. c Treatment-related deaths: autoimmune hepatitis, mucosal inflammation/death, and septic shock. AE: adverse effect; DOR: duration of response; ECOG PS: Eastern Cooperative Oncology Group performance status; IC: tumor-infiltrating immune cell; IHC: immunohistochemistry; ITT: intent to treat; mTNBC: metastatic triple-negative breast cancer; nab-P: nab-paclitaxel; ORR: objective response rate; PBO: placebo; PD: progressive disease; PD-L1: programmed death ligand-1; RECIST: Response Evaluation Criteria in Solid Tumors; TFI: treatment-free interval; TNBC: triple-negative breast cancer; TRAE: treatment-related adverse effect. 1. Schmid P et al. 43rd European Society for Medical Oncology Congress (ESMO 2018). Abstract LBA1_PR. 2. Schmid P et al. NEnglJMed. 2018;379:2108-2121. Access the activity,“On the Cusp of the Era of Immuno-Oncology in Triple-Negative Breast Cancer: Rational Strategies to Make the Most of Immunotherapies and Other Effective Treatment Modalities Throughout the Disease Continuum,”at PeerView.com/PMD40. ATEZOLIZUMAB PLUS NAB-PACLITAXEL IN LOCALLY ADVANCED/METASTATIC TRIPLE-NEGATIVE BREAST CANCER A Trial Overview PRACTICE AID Primary PFS Analysis Median PFS: ITT Median PFS: PD-L1+ 7.2 mo 5.5 mo Stratified HR = 0.80 (95% CI, 0.69-0.92) P = .0025 7.5 mo 5.0 mo 21.3 mo 17.6 mo 25.0 mo 15.5 mo Atezo +nab-P Placebo +nab-P ORR 56% 46% Safety Summary Interim OS Analysis Median OS: ITT Median OS: PD-L1+ Atezo +nab-P Placebo +nab-P Atezo +nab-P Placebo +nab-P Stratified HR = 0.62 (95% CI, 0.49-0.78) P < .0001 Stratified HR = 0.84 (95% CI, 0.69-1.02) P = .0840 Stratified HR = 0.62 (95% CI, 0.45-0.86) ITT PD-L1+ 59% 43% DOR 7.4 mo DOR 5.6 mo DOR 8.5 mo DOR 5.5 mo TRAE, % Atezo + nab-P (n = 452) Placebo + nab-P (n = 438) Any grade 96 94 Grade 3/4 40 30 Grade 5c 1 <1 All-Cause AEs, % Atezo + nab-P (n = 452) Placebo + nab-P (n = 438) Any grade 99 98 Grade 3/4 49 42 Grade 5 1 1 Any-Grade Serious AEs, % Atezo + nab-P (n = 452) Placebo + nab-P (n = 438) Regardless of attribution 23 18 TRAEs 12 7 Safety-Evaluable Population Until RECIST v1.1 PD or toxicity IMpassion1301,2 The first prospective, randomized, placebo-controlled, phase 3 trial to demonstrate a benefit with first-line immunotherapy in mTNBC • Metastatic or inoperable locally advanced TNBC • No prior therapy for advanced TNBC (prior chemo in the curative setting, including taxanes, allowed if TFI ≥12 mo) • ECOG PS 0-1 Patients Atezolizumab 840 mg on d 1 and 15 of 28-d cycle + nab-paclitaxel 100 mg/m2 IV on d 1, 8, and 15 of 28-d cycle Placebo IV on d 1 and 15 of 28-d cycle + nab-paclitaxel 100 mg/m2 on d 1, 8, and 15 of 28-d cycle 1:1 randomization stratified by prior taxane use, liver metastases, and PD-L1 status on IC (≥1% vs <1%)a Double-blind; no crossover permitted Atezo + nab-P vs PBO + nab- Endpoints Co-primary • PFS and OS in the ITT and PD-L1+ populationsb Key Secondary • ORR, DOR, and safety n = 451 n = 451
- 3. IMMUNO-ONCOLOGY 101 Harnessing the Immune System in the Treatment of Triple-Negative Breast Cancer PRACTICE AID Access the activity,“On the Cusp of the Era of Immuno-Oncology in Triple-Negative Breast Cancer: Rational Strategies to Make the Most of Immunotherapies and Other Effective Treatment Modalities Throughout the Disease Continuum,”at PeerView.com/PMD40. Without Immunotherapy With Immunotherapy MHC Antigen TCR PD-1 PD-L1 Anti– PD-L1 Anti– PD-1 Tumor cell Tumor escape Inactivation of T Cell Activation of T Cell Elimination of tumor cells Without Immunotherapy With Immunotherapy MHC CD80/86 CTLA-4 Anti– CTLA-4 antibody APC Antigen TCR Inactivation of T Cell Activation of T Cell Tumor escape Elimination of tumor cells Immune Checkpoint Inhibition in the Treatment of Cancer1 Immune checkpoints Proteins on T cells or cancer cells that need to be activated/inactivated to start/stop an immune response Examples include PD-1, PD-L1, CTLA-4 Serve as “brakes” that help keep immune responses in check; can prevent T-cell response against cancer cells Can be blocked by immune checkpoint inhibitors The “brakes” on the immune system are released and T cells are able to attack and kill cancer cells PD-1/PD-L1 Checkpoint Inhibition2 CTLA-4 Checkpoint Inhibition2 CTLA-4 is a negative regulator of costimulation required for activation of an antitumor T cell in a lymph node upon recognition of tumor antigen PD-1 pathway inhibits signaling downstream of TCR: TCR triggered by antigen presented by tumor cell à negative regulatory receptor PD-1 expressed à PD-L1 reactively expressed à PD-L1 binds to PD-1 Tumor microenvironment Lymphoid tissue Anti–PD-1 or anti–PD-L1 monoclonal antibodies block the interaction and negative regulation Anti–CTLA-4 monoclonal antibodies block negative regulation by CTLA-4 T cell inactivated Tumor escape T cell activated Tumor attack T cell inactivated Tumor escape T cell activated Tumor attack STOP GO STOP GO
- 4. IMMUNO-ONCOLOGY 101 Harnessing the Immune System in the Treatment of Triple-Negative Breast Cancer PRACTICE AID APC: antigen-presenting cell; CD: cluster of differentiation; CTLA-4: cytotoxic T-lymphocyte–associated protein 4; MHC: major histocompatibility complex; PD-1: programmed cell death protein 1; PD-L1: programmed death ligand 1; TCR: T-cell receptor; TIL: tumor-infiltrating lymphocyte; TNBC: triple-negative breast cancer. 1. Ribas A, Wolchock JD. Science. 2018;359:1350-1355. 2. Adapted from: Soularue E et al. Gut. 2018;67:2056-2067. 3. de la Cruz-Merino et al. Clin Trans Oncol. 2019;21:117-125. 4. Vikas P et al. Cancer Manag Res. 2018;10:6823-6833. 5. Tecentriq (atezolizumab) Prescribing Information. https://www.gene.com/download/pdf/tecentriq_prescribing.pdf. Accessed November 19, 2019. 6. https://www.fda.gov/Drugs/ InformationOnDrugs/ApprovedDrugs/ucm633065.htm. Accessed November 19, 2019. Access the activity,“On the Cusp of the Era of Immuno-Oncology in Triple-Negative Breast Cancer: Rational Strategies to Make the Most of Immunotherapies and Other Effective Treatment Modalities Throughout the Disease Continuum,”at PeerView.com/PMD40. Rationale for Immunotherapy in TNBC3,4 FDA Approval of Immunotherapy in TNBC5,6 First approval in breast cancer FDA granted accelerated approval to atezolizumab in combination with nab-paclitaxel for adult patients with unresectable locally advanced or metastatic TNBC whose tumors express PD-L1 (PD-L1–stained, tumor-infiltrating immune cells of any intensity covering ≥1% of the tumor area), as determined by an FDA-approved test More to come! Immune Checkpoint Inhibitors Under Investigation in TNBC Anti–PD-1 inhibitors: Pembrolizumab Nivolumab Anti–PD-L1 inhibitors: Atezolizumab Durvalumab Avelumab Anti–CTLA-4 inhibitors: Ipilimumab Tremelimumab TNBC tumors with a highly invasive characteristic express a large amount of PD-L1 and a high degree of TILs compared with other subtypes of breast cancer Implicates immunogenic nature of TNBC Rationale for testing/use of immunotherapies in TNBC More aggressive forms of breast cancer have some degree of host immunity, but it appears to decrease as the tumors progress and become more resistant (eg, advanced, heavily pretreated TNBC) Reduction in body’s immune response to the cancer Immunotherapy may be more effective in earlier stages of TNBC Rationale for testing/use of immunotherapies in neoadjuvant or adjuvant settings Multimodal therapy may enhance the activity of immunotherapies in TNBC and other subtypes of breast cancer Combination or sequential strategies with chemotherapies, targeted therapies, other immunotherapies with nonredundant mechanisms of action, vaccines, surgery, radiation, and cryotherapy are being explored
- 5. Access the activity,“On the Cusp of the Era of Immuno-Oncology in Triple-Negative Breast Cancer: Rational Strategies to Make the Most of Immunotherapies and Other Effective Treatment Modalities Throughout the Disease Continuum,”at PeerView.com/PMD40. SELECTION OF KEY IMMUNO-ONCOLOGY CLINICAL TRIALS IN TRIPLE-NEGATIVE BREAST CANCER1 PRACTICE AID Atezolizumab + nab-paclitaxel atezolizumab + AC surgery atezolizumab vs placebo + nab-paclitaxel placebo + AC surgery NCT03197935 IMpassion031 Phase 3 Anti–PD-L1 Atezolizumab + paclitaxel + carboplatin atezolizumab + (AC or EC) surgery atezolizumab vs placebo + paclitaxel + carboplatin placebo + (AC or EC) surgery placebo NCT03281954 GBG 96-GeparDouze Phase 3 Anti–PD-L1 Atezolizumab + nab-paclitaxel + carboplatin surgery AC or EC or FEC vs nab-paclitaxel + carboplatin surgery AC or EC or FEC NCT02620280 NeoTRIPaPDL1 Phase 3 Anti–PD-L1 NCT03036488a KEYNOTE-522 Phase 3 Anti–PD-1 Durvalumab durvalumab + nab-paclitaxel durvalumab + EC surgery vs placebo placebo + nab-paclitaxel placebo + EC surgery NCT02685059 GeparNuevo Phase 2 Anti–PD-L1 Pembrolizumab + nab-paclitaxel pembrolizumab + EC surgery NCT03289819 NIB Phase 2 Anti–PD-1 Olaparib durvalumab + olaparib surgery NCT03594396 Phase 1/2 Anti–PD-L1 Pembrolizumab + radiotherapy boost surgery NCT03366844 Anti–PD-1 Phase 1/2 Nivolumab surgery vs nivolumab + doxorubicin surgery NCT03815890 BELLINI Phase 2 Anti–PD-1 Nivolumab + ipilimumab core biopsy/cryoablation surgery nivolumab vs surgery NCT03546686 Phase 2 Anti–PD-1 + anti–CTLA-4 Neoadjuvant Setting Pembrolizumab + paclitaxel + carboplatin pembrolizumab + (AC or EC) surgery pembrolizumab vs placebo + paclitaxel + carboplatin placebo + (AC or EC) surgery placebo
- 6. Access the activity,“On the Cusp of the Era of Immuno-Oncology in Triple-Negative Breast Cancer: Rational Strategies to Make the Most of Immunotherapies and Other Effective Treatment Modalities Throughout the Disease Continuum,”at PeerView.com/PMD40. SELECTION OF KEY IMMUNO-ONCOLOGY CLINICAL TRIALS IN TRIPLE-NEGATIVE BREAST CANCER1 PRACTICE AID Pembrolizumab + radiotherapy vs observation + radiotherapy (for residual disease after neoadjuvant chemo and surgery) NCT02954874 SWOG-S1418 Phase 3 Anti–PD-1 Avelumab vs observation (after surgery, neo- or adjuvant chemo, and radiotherapy if indicated) NCT02926196 A-Brave Phase 3 Anti–PD-L1 Atezolizumab + paclitaxel → atezolizumab + (AC or EC) → atezolizumab vs paclitaxel → AC or EC NCT03498716 IMpassion030 Phase 3 Anti–PD-L1 Nivolumab vs capecitabine vs nivolumab + capecitabine (for residual disease after neoadjuvant chemo and surgery) NCT03487666 OXEL Phase 2 Anti–PD-1 Adjuvant Setting Nivolumab + ipilimumab + radiotherapy vs capecitabine + radiotherapy (for residual disease after neoadjuvant chemo and surgery) NCT03818685 BreastImmune03 Phase 2 Anti–PD-1 + anti–CTLA-4 Atezolizumab + capecitabine vs capecitabine (for residual disease after neoadjuvant chemo and surgery) NCT03756298 Phase 2 Anti–PD-1
- 7. Access the activity,“On the Cusp of the Era of Immuno-Oncology in Triple-Negative Breast Cancer: Rational Strategies to Make the Most of Immunotherapies and Other Effective Treatment Modalities Throughout the Disease Continuum,”at PeerView.com/PMD40. SELECTION OF KEY IMMUNO-ONCOLOGY CLINICAL TRIALS IN TRIPLE-NEGATIVE BREAST CANCER1 PRACTICE AID Atezolizumab + nab-paclitaxel vs placebo + nab-paclitaxel NCT02425891 IMpassion130 Phase 3 Anti–PD-L1 Atezolizumab + paclitaxel vs placebo + paclitaxel NCT03125902 IMpassion131 Phase 3 Anti–PD-L1 Pembrolizumab + [nab-paclitaxel or paclitaxel or (gemcitabine + carboplatin)] vs placebo + [nab-paclitaxel or paclitaxel or (gemcitabine + carboplatin)] NCT02819518 KEYNOTE-355 Phase 3 Anti–PD-1 Metastatic/Advanced Setting Pembrolizumab NCT02447003 KEYNOTE-086 Phase 2 Anti–PD-1 1st line 1st line 1st line Durvalumab + tremelimumab → durvalumab NCT02536794 Phase 2 Anti–PD-L1 + anti–CTLA-4 1st line 1st line Atezolizumab + [(gemcitabine + carboplatin) or capecitabine] vs placebo + [(gemcitabine + carboplatin) or capecitabine] NCT03371017 IMpassion132 Phase 3 Anti–PD-L1 1st line Pembrolizumab vs capecitabine or eribulin or gemcitabine or vinorelbine NCT02555657 KEYNOTE-119 Phase 3 Anti–PD-1 ≥2nd line Pembrolizumab + doxorubicin → pembrolizumab NCT02648477 Phase 2 Anti–PD-1 Pembrolizumab + nab-paclitaxel NCT02752685 Phase 2 Anti–PD-1 1st line 1st line Pembrolizumab + carboplatin + gemcitabine vs carboplatin + gemcitabine NCT02755272 Phase 2 Anti–PD-1 Pembrolizumab + cyclophosphamide NCT02768701 Phase 2 Anti–PD-1 1st line 1st line
- 8. a Continued in adjuvant setting. 1. https://clinicaltrials.gov. November 26, 2019. AC: doxorubicin + cyclophosphamide; chemo: chemotherapy; CTLA-4: cytotoxic T-lymphocyte–associated protein 4; EC: epirubicin + cyclophosphamide; FEC: fluorouracil + epirubicin + cyclophosphamide; PD-1: programmed cell death protein 1; PD-L1: programmed death ligand 1. Access the activity,“On the Cusp of the Era of Immuno-Oncology in Triple-Negative Breast Cancer: Rational Strategies to Make the Most of Immunotherapies and Other Effective Treatment Modalities Throughout the Disease Continuum,”at PeerView.com/PMD40. SELECTION OF KEY IMMUNO-ONCOLOGY CLINICAL TRIALS IN TRIPLE-NEGATIVE BREAST CANCER1 PRACTICE AID Olaparib → durvalumab + olaparib NCT03801369 Phase 2 Anti–PD-1 Pembrolizumab + carboplatin + nab-paclitaxel NCT03121352 Phase 2 Anti–PD-1 Pembrolizumab + radiotherapy NCT02730130 Phase 2 Anti–PD-1 Metastatic/Advanced Setting (Cont’d) Nivolumab + romidepsin + cisplatin NCT02393794 Phase 1/2 Anti–PD-1 1st/2nd line 1st-3rd line ≥2nd line Pembrolizumab + eribulin mesylate NCT02513472 ENHANCE-1 Anti–PD-L1 ≥1st line 1st-3rd line Atezolizumab + cobimetinib + paclitaxel vs atezolizumab + cobimetinib + nab-paclitaxel vs cobimetinib + paclitaxel vs placebo + paclitaxel NCT02322814 Phase 2 Anti–PD-L1 1st line Pembrolizumab + lenvatinib NCT03797326 LEAP-005 Phase 2 Anti–PD-1 ≥2nd line Durvalumab + paclitaxel → durvalumab NCT02628132 Anti–PD-1 ≥2nd line Radiotherapy → nivolumab vs doxorubicin → nivolumab vs cisplatin → nivolumab vs cyclophosphamide → nivolumab vs nivolumab NCT02499367 TONIC Phase 2 Anti–PD-1 2nd-4th line Phase 1/2 Phase 1/2