Hope Is on the Horizon for Patients With ALS: Overcoming Diagnostic Difficulties and Exploring Novel Emerging Therapeutic Approaches
•
0 likes•5 views

Chair, John Ravits, MD, FAAN, prepared useful Practice Aids pertaining to amyotrophic lateral sclerosis for this CME activity titled “Hope Is on the Horizon for Patients With ALS: Overcoming Diagnostic Difficulties and Exploring Novel Emerging Therapeutic Approaches.” For the full presentation, downloadable Practice Aids, and complete CME information, and to apply for credit, please visit us at http://bit.ly/3AgpcKy. CME credit will be available until March 16, 2024.

Recommended
Recommended
More Related Content
Similar to Hope Is on the Horizon for Patients With ALS: Overcoming Diagnostic Difficulties and Exploring Novel Emerging Therapeutic Approaches
Similar to Hope Is on the Horizon for Patients With ALS: Overcoming Diagnostic Difficulties and Exploring Novel Emerging Therapeutic Approaches (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Hope Is on the Horizon for Patients With ALS: Overcoming Diagnostic Difficulties and Exploring Novel Emerging Therapeutic Approaches
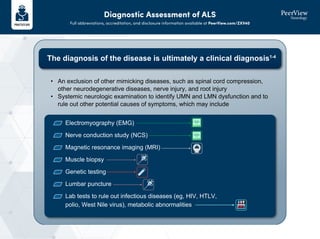
- 1. Diagnostic Assessment of ALS Full abbreviations, accreditation, and disclosure information available at PeerView.com/ZXV40 The diagnosis of the disease is ultimately a clinical diagnosis1-4 Electromyography (EMG) Nerve conduction study (NCS) Magnetic resonance imaging (MRI) Muscle biopsy Genetic testing Lumbar puncture Lab tests to rule out infectious diseases (eg, HIV, HTLV, polio, West Nile virus), metabolic abnormalities • An exclusion of other mimicking diseases, such as spinal cord compression, other neurodegenerative diseases, nerve injury, and root injury • Systemic neurologic examination to identify UMN and LMN dysfunction and to rule out other potential causes of symptoms, which may include
- 2. Diagnostic Assessment of ALS Full abbreviations, accreditation, and disclosure information available at PeerView.com/ZXV40 • Progression of symptoms over time • LMN signs by region (bulbar, cervical, thoracic, lumbosacral) – Clinical: weakness, fasciculations, atrophy – Electromyography LMN loss: fibrillations and positive sharp waves, fasciculations Reinnervation: large motor units and reduced recruitment • UMN signs by region (bulbar, cervical, thoracic, lumbosacral) – Clinical: spasticity, hyper-reflexia, pathologic reflexes, pseudobulbar affect Clinical/EMG evidence of LMN + UMN in 1 region or isolated UMN signs in 2 or more regions or LMN signs rostral to LMN signs Clinical LMN + UMN in 1 region and LMN signs in 2 regions Clinical/EMG evidence of LMN + UMN in 2 regions Some UMN signs rostral to LMN signs Clinical/EMG evidence of LMN + UMN in 3 regions Clinically possible ALS Clinically probable ALS (laboratory supported) Clinically probable ALS Clinically definite ALS Revised El Escorial and Awaji Diagnostic Criteria for ALS5 1. Hardiman O et al. Nat Rev Dis Primers. 2017;3:17071. 2. Brown RH et al. N Engl J Med. 2017;377:162-172. 3. Kiernan MC et al. Lancet. 2011;377:942-955. 4. http://webgw.alsa.org/site/PageServer?pagename=GW_12_AAM16_what_is_als#gsc.tab=0. 5. Quinn C, Elman L. Continuum (Minneap Minn). 2020;26:1323-1347.
- 3. Mechanisms of Action of Emerging Therapies in ALS1-6 Full abbreviations, accreditation, and disclosure information available at PeerView.com/ZXV40 Catalyzes oxidation of NADH to NAD+ CNM-Au8 is an oral suspension of clean-surfaced, catalytically active gold nanocrystals Driving production of ATP and restoring energy in brain cells Reduces accumulation of TDP-43 aggregates in the cytoplasm CNM-Au8 Mechanism of Action ATP TDP-43 N NH2 NH2 O O P P O O O O O O HO HO HO OH OH OH N N N N NADH N N NH2 N N N+ NH2 O O O O O P P O O OH HO OH OH OH OH O NAD+ Emerging Small-Molecule Therapies
- 4. Mechanisms of Action of Emerging Therapies in ALS1-6 Full abbreviations, accreditation, and disclosure information available at PeerView.com/ZXV40 • RIPK1 regulates a neuroinflammatory environment in the CNS that can lead to cell necroptosis and neurodegeneration • SAR443820 is a CNS-penetrant small-molecule inhibitor of RIPK1 Microglial cell Damaged mitochondrion • Demyelination • Axonal degeneration Cytokines DAMPs Neuron Damaged lysosome Oligodendrocyte Necroptosis Homeostatic suppression RIPK1 RIPK3 RIPK1 RIPK1 RIPK3 MLKL Deleterious inflammation Necroptosis SAR443820: RIPK1 Inhibitor Integrated stress response DNL343 eIF2B ON Reinitiated translation Reversible stress granules Stress response proteins and genes (eg, ATF4, CHAC1) DNL343 Treatment • DNL343 is currently being investigated in a phase 1b trial to evaluate safety, PK, and PD in patients with ALS • In ALS, chronic activation of the integrated stress response (ISR) occurs because of inactivation of eIF2B and formation of “stress granules,” precursors to TDP-43 aggregation DNL343: eIF2B Agonist Emerging Small-Molecule Therapies
- 5. Mechanisms of Action of Emerging Therapies in ALS1-6 Full abbreviations, accreditation, and disclosure information available at PeerView.com/ZXV40 1. Jiang J et al. Front Pharmacol. 2022;13:1054006. 2. Yuan J et al. Nat Rev Neurosci. 2019;20:19-33. 3. Sun L et al. 2022 International Symposium on ALS/MND. Abstract CLT-09. 4. https://clinicaltrials.gov/ct2/show/NCT05006352?term=DNL343&draw=2&rank=2. 5. Robberecht W, Philips T. Nat Rev Neurosci. 2013;14:248-264. 6. Miller T et al. N Engl J Med. 2020;383:109-119. Emerging Small-Molecule Therapies Antisense oligonucleotides • Are administered intrathecally • Are widely distributed throughout the CSF • Duration of action is between 1 to 3 months Tofersen: Antisense Oligonucleotide Targeting SOD1 ALS DNA mRNA SOD1 protein Antisense oligonucleotide Enzymatic degradation Oligomers and pre-aggregates DNA Mutant SOD1 gene Modified SOD1 protein SOD1 mRNA Aggregates SOD1 ALS Is Thought to Be GOF Mechanism Pathogenic Mechanism of Mutant SOD1-Induced Toxicity Dysfunction in the cytoplasm and toxicity