Current and Emerging Therapies for Endometriosis and Uterine Fibroids: What Do You Need to Know?
•
0 likes•95 views

Georgine Lamvu, MD, MPH prepared useful Practice Aids pertaining to the diagnosis and management of endometriosis and uterine fibroids for this CME activity titled "Current and Emerging Therapies for Endometriosis and Uterine Fibroids: What Do You Need to Know?" For the full presentation, monograph, complete CME information, and to apply for credit, please visit us at https://bit.ly/3cH0J2A. CME credit will be available until August 2, 2021.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Current and Emerging Therapies for Endometriosis and Uterine Fibroids: What Do You Need to Know?
Similar to Current and Emerging Therapies for Endometriosis and Uterine Fibroids: What Do You Need to Know? (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Current and Emerging Therapies for Endometriosis and Uterine Fibroids: What Do You Need to Know?
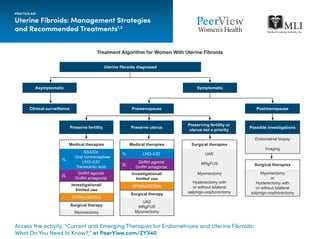
- 1. Uterine Fibroids: Management Strategies and Recommended Treatments1,2 PRACTICE AID Access the activity, “Current and Emerging Therapies for Endometriosis and Uterine Fibroids: What Do You Need to Know?,” at PeerView.com/ZYV40 Treatment Algorithm for Women With Uterine Fibroids Uterine fibroids diagnosed Asymptomatic Clinical surveillance Premenopause Preserving fertility or uterus not a priority Preserve uterusPreserve fertility Symptomatic Postmenopause Possible investigations Endometrial biopsy Imaging Surgical therapies Myomectomy or Hysterectomy with or without bilateral salpingo-oophorectomy Surgical therapies UAE MRgFUS Myomectomy Hysterectomy with or without bilateral salpingo-oophorectomy Medical therapies 1L NSAIDs Oral contraceptives LNG-IUD Tranexamic acid 2L GnRH agonist GnRH antagonist Investigational/ limited use SPRMs/SERMs Surgical therapy Myomectomy Medical therapies 1L LNG-IUD 2L GnRH agonist GnRH antagonist Investigational/ limited use SPRMs/SERMs Surgical therapy UAE MRgFUS Myomectomy
- 2. Uterine Fibroids: Management Strategies and Recommended Treatments1,2 PRACTICE AID Access the activity, “Current and Emerging Therapies for Endometriosis and Uterine Fibroids: What Do You Need to Know?,” at PeerView.com/ZYV40 1L Medical Therapy Description Advantages Disadvantages Fertility Preserved? NSAIDs • Anti-inflammatories and prostaglandin inhibitors • Reduce pain and blood loss from fibroids • Do not decrease fibroid volume • Gastrointestinal AEs Yes Oral contraceptives • Treats abnormal uterine bleeding likely by stabilization of endometrium • Reduces blood loss from fibroids • Ease of conversion to alternative therapy • Do not decrease fibroid volume Yes, if discontinued after resolution of symptoms LNG-IUD • Treats abnormal uterine bleeding likely by stabilization of endometrium • Most effective for reducing blood loss • Decreases fibroid volume • Irregular uterine bleeding • Increased risk of device expulsion Yes, if discontinued after resolution of symptoms Tranexamic acid • Antifibrinolytic therapy • Reduces blood loss from fibroids • Ease of conversion to alternate therapy • Does not decrease fibroid volume • Medical contraindications Yes 2L Medical Therapy Description Advantages Disadvantages Fertility Preserved? GnRH agonists • Preoperative treatment to decrease tumor size or in women approaching menopause • Decreases blood loss, operative time, and recovery time • Long-term treatment associated with higher cost, menopausal symptoms, and bone loss • Increased recurrence risk with myomectomy Depends on subsequent procedure GnRH antagonists3,4,a • Binds competitively to progesterone receptor • Reduce blood loss, dysmenorrhea, and fibroid size • Initial increase in bleeding • Vasomotor symptoms • Bone density loss Depends on subsequent procedure Investigational/ Limited Use Description Advantages Disadvantages Fertility Preserved? SPRMs • Preoperative treatment to decrease tumor size or in women approaching menopause • Decreases blood loss, operative time, and recovery time • Not associated with hypoestrogenic AEs • Headache, breast tenderness, PAEC • Increased recurrence risk with myomectomy Depends on subsequent procedure Current and Investigational Management Strategies for Women With Uterine Fibroids
- 3. Uterine Fibroids: Management Strategies and Recommended Treatments1,2 a FDA approved in combination with estradiol and norethindrone acetate for management of heavy menstrual bleeding associated with uterine fibroids in premenopausal women (up to 24 months). 1L: first line; 2L: second line; AEs: adverse events; GnRH: gonadotropin-releasing hormone; LNG-IUD: levonorgestrel-releasing intrauterine device; MRgFUS: magnetic resonance–guided focused ultrasound surgery; NSAIDs: nonsteroidal anti-inflammatory drugs; PAEC: progesterone receptor modulator–associated endometrial changes; SPRMs: selective progesterone receptor modulators; UAE: uterine artery embolization. 1. Vilos GA et al. J Obstet Gynaecol Can. 2015;37:157-178. 2. De La Cruz MSD, Buchanan EM. Am Fam Physician. 2017;95:100-107. 3. Schlaff WD et al. N Engl J Med. 2020;382:328-340. 4. Singh SS et al. Am J Obstet Gynecol. 2018;218:563-572.e1. PRACTICE AID Access the activity, “Current and Emerging Therapies for Endometriosis and Uterine Fibroids: What Do You Need to Know?,” at PeerView.com/ZYV40 Surgical Therapy Description Advantages Disadvantages Fertility Preserved? Hysterectomy • Surgical removal of uterus (transabdominally, transvaginally, or laparoscopically) • Definitive treatment for when preserving fertility not a priority • Transvaginal and laparoscopic approach associated with decreased pain, blood loss, and recovery time compared with transabdominal surgery • Transabdominal surgery risks (infection, pain, fever, increased blood loss, and recovery time) • Morcellation with laparoscopic approach increases risk of iatrogenic dissemination of tissue No MRgFUS • In situ destruction using high-intensity ultrasound waves • Noninvasive approach • Shorter recovery time with modest symptom improvement • Heavy menses • Pain from sciatic nerve irritation • Higher reintervention rate Unknown Myomectomy • Surgical or endoscopic excision of tumors • Resolution of symptoms with preservation of fertility • Recurrence rate of 15%-30% at 5 years, depending on size and extent of tumors Yes UAE • Interventional radiologic procedure to occlude uterine arteries • Minimally invasive • Avoids surgery • Short hospitalization • Recurrence rate 17% at 30 months • Postembolization syndrome Unknown Current and Investigational Management Strategies for Women With Uterine Fibroids (Cont'd)
- 4. Clinical Diagnosis of Endometriosis1 a Alternative diagnosis indicated by symptoms on the right side of the figure may coexist with endometriosis and does not rule out endometriosis. IBS: irritable bowel syndrome; NSAIDs: nonsteroidal anti-inflammatory drugs. 1. Agarwal SK et al. Am J Obstet Gynecol. 2019;220:354.e1-354.e12. PRACTICE AID Access the activity, “Current and Emerging Therapies for Endometriosis and Uterine Fibroids: What Do You Need to Know?,” at PeerView.com/ZYV40 ConsistentWithEndometriosis ConsiderOtherDiagnosisinAdditiontoEndometriosisa Step 1: Evaluate Presence of Symptoms Step 2: Review Patient History Step 3: Perform a Physical Examination Step 4: Perform/Order Imaging • Persistent and/or worsening cyclic or constant pelvic pain • Dysmenorrhea • Deep dyspareunia • Cyclic dyschezia • Cyclic dysuria • Cyclic catamenial symptoms located in other systems (eg, lung, skin) • Infertility • Dysmenorrhea in adolescence; current chronic pelvic pain • Previous laparoscopy with diagnosis • Dysmenorrhea unresponsive to NSAIDs • Positive family history • Nodules in cul-de-sac • Retroverted uterus • Mass consistent with endometriosis • Obvious endometrioma that is external (seen on speculum or on skin) • Endometrioma on ultrasound • Presence of soft markers (eg, sliding sign) • Nodules and masses • Severe pain, amenorrhea, or cramping without menstruation in adolescent could indicate a reproductive tract anomaly • Severe noncyclic constipation and diarrhea suggest IBS • Painful voiding or flank pain could suggest urinary tract stones • Urinary symptoms (eg, hematuria, frequent urination) could indicate interstitial cystitis/painful bladder symptoms • Absence of menses or other obstructive conditions in adolescence • History of pain directly associated with surgery (eg, postoperative nerve entrapment or injury, bowel adhesions) • Pelvic floor spasms • Severe allodynia along pelvic floor/vulva or elsewhere • Masses not consistent with endometriosis (eg, fibroids) • Adenomyosis and fibroids (although these may be present with endometriosis)