
Recommended
Recommended
More Related Content
Similar to httpsdoi.org10.11771534650120954275Clinical Case Stud
Similar to httpsdoi.org10.11771534650120954275Clinical Case Stud (20)
More from PazSilviapm
More from PazSilviapm (20)
Recently uploaded
Recently uploaded (20)
httpsdoi.org10.11771534650120954275Clinical Case Stud
- 1. https://doi.org/10.1177/1534650120954275 Clinical Case Studies 2021, Vol. 20(1) 22 –38 © The Author(s) 2020 Article reuse guidelines: sagepub.com/journals-permissions DOI: 10.1177/1534650120954275 journals.sagepub.com/home/ccs Original Manuscript Schema Therapy for Chronic Depression Associated with Childhood Trauma: A Case Study Kate L. Herts1,2 and Susan Evans1,2 Abstract Chronic depression lasting longer than 2 years is often undertreated. Research suggests that maladaptive cognitive schemas mediate the association between childhood trauma and later depression. Schema Therapy (ST) is an integrative treatment approach that targets maladaptive cognitive schemas through cognitive, behavioral, interpersonal, and experiential interventions. ST has been studied in patients with chronic depression with good results. The purpose of this case study is to detail how an ST treatment was used to
- 2. treat chronic depression in a woman, “Amy,” with a childhood trauma history. Amy presented with a persistent depressive disorder that had lasted over 40 years. An ST approach was chosen in light of the chronicity of Amy’s symptoms and her childhood trauma history. Standardized measures including the Beck Depression Inventory were used to assess progress throughout treatment. We provide a comprehensive summary of the 22-session ST case conceptualization and treatment, through which Amy’s depressive symptoms evidenced a 73 percent reduction. Amy qualitatively reported reduced depressive rumination and avoidance behaviors as well as increased frequency of positive mood. Keywords depression, chronic depression, schema therapy, childhood trauma 1 Theoretical and Research Basis for Treatment Depressive disorders are a leading cause of global di sease burden (Ferrari et al., 2013). Consistent with past research, we use the term “chronic depression” to describe dysthymia, chronic major depression, double depression and recurrent major depression without instances of complete remission, because past research has failed to show systematic underlying differences in etiology (Hölzel et al., 2011). It is estimated that 20% of all depressed individuals and up to 47% of patients in outpatient mental health settings are chronically depressed, with symptoms lasting at least 2 years (Torpey & Klein, 2008).
- 3. Cognitive Behavioral Therapy (CBT) is currently the gold standard psychotherapy treatment for major depression, as well as anxiety and other disorders (David et al., 2018). However, few 1Weill Cornell Medicine, New York, NY, USA 2New York Presbyterian Hospital, New York, NY, USA Corresponding Author: Kate L. Herts, Weill Cornell Medicine, 240 E 69th St, New York, NY 10065, USA. Email: [email protected] 954275CCSXXX10.1177/1534650120954275Clinical Case StudiesHerts and Evans research-article2020 https://us.sagepub.com/en-us/journals-permissions https://journals.sagepub.com/home/ccs mailto:[email protected] http://crossmark.crossref.org/dialog/?doi=10.1177%2F15346501 20954275&domain=pdf&date_stamp=2020-09-04 Herts and Evans 23 studies have specifically examined the efficacy of psychotherapy in the treatment of chronic depression. Cuijpers and colleagues (2010) conducted a meta- analysis of 16 randomized con- trolled trials of the impact of psychotherapy on chronic depression and found that psychotherapy has only a small (though statistically significant) effect as compared to control groups. In addi- tion, combined treatment with an SSRI was more effective than
- 4. either treatment alone (Cuijpers et al., 2010). A recent systematic review found only 10 studies that examined pharmacotherapy, psychotherapy, or their combination in the treatment of chronic major depression (Spijker et al., 2013). The best evidence was found for Cognitive Behavioral Analysis Systems of Psychotherapy (CBASP), an individual cognitive behavior treatment specifically developed for the treatment of chronic depression, in combination with the antidepressant nefazadone, which together demon- strated moderate to large effects (Spijker et al., 2013). Taken together, this research suggests that psychotherapy may be less effective in treating chronic depression as compared to discrete epi- sodes of major depressive disorder. Indeed, research has shown that for many patients, chronic depression is undertreated (Kocsis et al., 2008) or not fully responsive to treatment (Torpey & Klein, 2008). Impact of Childhood Trauma Research suggests that childhood trauma is a significant predictor of depression in adulthood. Data from a longitudinal cohort in the Netherlands demonstrated that among adults with a diag- nosis of major depression, a retrospectively reported history of emotional abuse, emotional neglect and physical abuse in childhood were significant predictors of chronic depression (Hovens et al., 2012; Wiersma et al., 2009). A recent meta- analysis of studies examining child- hood trauma as a predictor of later depression found that experiencing emotional abuse or neglect in childhood carried stronger risk for depression as compared to
- 5. other traumatic events (e.g., sexual abuse; Mandelli et al., 2015). Beck and colleague’s (1979) cognitive model of depression posits that patients with depres- sion have maladaptive core beliefs, or schema, through which they view themselves, their experiences and the future. Research demonstrates that maladaptive cognitive schemas in the Disconnection and Rejection domain mediate the relationship between childhood trauma and later depression in college students (e.g., Rezaei et al., 2016). This domain encompasses sche- mas characterized by abandonment, defectiveness and shame, emotional deprivation, mistrust and abuse, social introversion and isolation/withdrawal. Treatment that specifically targets maladaptive schemas in the Disconnectio n and Rejection domain may thus be particularly helpful for depressed patients with a childhood trauma history. Post-traumatic stress disorder (PTSD) is often comorbid with depression in the aftermath of trauma. In a study of over 350 trauma-exposed adults, Contractor and colleagues (2018) found that the negative alterations in cognitions and mood present in PTSD accounted for significant variance between PTSD and non-somatic depression, though it is notable that other research (e.g., Byllesby et al., 2017) suggests that a general distress factor provides a better explanation for the comorbidity between these disorders. Gurak and colleagues (2016) describe the treat- ment of a young adult woman with comorbid PTSD and recurrent MDD, as well as a childhood trauma history. The patient benefited from cognitive processing
- 6. therapy interventions, which helped her restructure maladaptive trauma-related core beliefs that were contributing to feel- ings of guilt (Gurak et al., 2016). The patient ultimately saw a significant reduction in depres- sive symptoms over the course of integrative trauma treatment (Gurak et al., 2016). Taken together, these findings suggest that treating maladaptive trauma-related cognitions as well as general, non-trauma specific distress as in ST can be impactful for trauma-exposed patients with depression. 24 Clinical Case Studies 20(1) Schema Therapy for Chronic Depression Schema Therapy (ST), developed by Jeffrey Young (1999) and colleagues, is an integrative approach that expands beyond traditional cognitive behavioral therapy (CBT) and combines interpersonal and experiential strategies to address a variety of chronic psychological disorders. ST is grounded in attachment theory and uses Gestalt theory and practice such as imagery to access emotion. The therapy therefore combines cognitive, behavioral, interpersonal and experi- ential techniques to address current negative life patterns (i.e., attachment to unavailable part- ners) by connecting them to schemas that were formed in childhood and adolescence. Schemas may be defined as self-defeating emotional and cognitive patterns that begin early in develop- ment and continue throughout life. ST differs from Beck’s
- 7. original therapy for depression (Beck et al., 1979) in that there is a greater emphasis on the therapeutic relationship (includes limited reparenting), on affect and the understanding of childhood origins. Since its development there is some empirical evidence of the effectiveness of ST for treating personality disorders (PD), particularly in Europe where ST is the first treatment of choice for PD. While the effectiveness of CBT is well documented for the treatment of depression, there continues to be a percentage of patients who do not respond, may be partial remitters, or patients who relapse. ST is a promising alternative treatment for depression, particularly for patients with comorbid personality disorders. For example, Seavey and Moore (2012) describe a case of an 18-year-old man with first episode Major Depressive Disorder and personality disorder not oth- erwise specified who went into full remission from depression after ST. In addition, patients with trauma-related depression have benefited from Acceptance and Commitment Therapy (e.g., Hiraoka et al., 2016), which similarly to ST, diverges from CBT in its central reliance on experi- ential exercises. In recent years, ST has been applied and studied in patients with chronic forms of depression with good results. Malogiannis et al. (2014) for example, studied 12 chronically depressed patients who received ST over 60 sessions. The authors found that five patients showed reduced symptoms at end of treatment and at the 6 month follow up period and only one relapsed, while
- 8. two who had initially only partially improved ultimately recovered fully. In a more recent study by Renner et al. (2016), 25 patients with chronic depression who underwent a course of ST expe- rienced a significant reduction in symptoms as compared with a wait-list control group. The authors concluded that their findings provide evidence that ST may be an effective treatment for patients with chronic depression. Objective The purpose of the current case report is to provide an example of how ST interventions can be used to enhance cognitive behavioral treatment of chronic depression. We achieve this aim by detailing the case of a patient, with a history of childhood trauma and chronic depression, who partially responded to CBT and went on to achieve full remission through ST. We examine likely schemas underlying the patient’s persistent symptoms and through restructuring them incite changes in the patient’s maladaptive cognitive and behavioral life patterns. Finally, we provide clinical practice recommendations for providers caring for patients who may benefit from ST. 2 Case Introduction Cornell Cognitive Therapy Clinic The Cornell Cognitive Therapy Clinic (CTC) located in Manhattan, NY, is an outpatient clinic in a large academic medical center and serves a diversity of patients. While the CTC sees primarily
- 9. Herts and Evans 25 patients diagnosed with depressive and anxiety disorders, the program accepts a range of patients with DSM-V disorders. Patients are often referred to the CTC from other practitioners both within the medical center and from neighboring practices and institutions in the area. The CTC is one of the few insurance-based therapy programs in the metropolitan areas and accepts most major insurance plans as well as Medicaid, which opens the clinic services to lower-income patients. Therapists in the CTC include four predoctoral psychology interns who are completing their last year of PhD graduate training in clinical psychology and one postdoctoral psychology fellow who has completed the full requirements for a PhD. Supervisors in the program are licensed clinical psychologists who have advanced training in CBT and have clinical practices of their own. Case Description “Amy” is a married, Caucasian female in her 60s, domiciled with her husband and teenaged daughter, working for a Jewish religious organization, who initially presented to the CTC in fall 2017 seeking treatment for chronic depression and anxiety. She had a history of over ten years of psychodynamic treatment. At the CTC, Amy was initially treated with 20 sessions of weekly CBT with a psychology intern. Treatment focused on cognitive restructuring and behavioral cop-
- 10. ing skills, for example, mindfulness, to help Amy manage anxiety about her daughter’s health and wellbeing. At the time of transfer to psychotherapy with the first author, then a postdoctoral fellow, Amy reported improvements in the severity of her anxiety and depressive symptoms over the course of CBT treatment (see details below). However, she continued to experience some anxiety and depressive symptoms, including low mood for much of the day on more days than not. In collaboration with Amy and the second author, the supervisor on the case, a course of ST was pursued in light of the chronic nature of Amy’s symptoms and her childhood trauma history. The goal of treatment was to help Amy identify and mitigate the impact of lifelong schemas and related maladaptive behaviors on her current functioning, in the service of inciting complete remission from mood and anxiety symptoms. 3 Presenting Complaints At the initial intake to the Cognitive Therapy Clinic, prior to beginning CBT treatment, Amy met full diagnostic criteria for generalized anxiety disorder, a major depressive episode and persistent depressive disorder. Amy’s anxiety consisted primarily of obsessive worry about the health and wellbeing of herself, her husband and her daughter. She reported little to no ability to control this worry. Amy also endorsed avoidance of situations that she perceived as dangerous to her family, such as allowing her daughter to fly to Israel. When she was presented with such situations, she experienced panic symptoms including shortness of breath and fear of going crazy/losing con-
- 11. trol, though her symptoms did not meet full diagnostic criteria for a panic attack. Her avoidance negatively impacted her relationship with her daughter, with whom she desperately desired closeness and further served to prevent her daughter from gaining developmentally appropriate independence. In addition, Amy’s primary mode for coping with worry was to play out the worst- case scenario in her mind, so that she would be prepared for it. This served to increase her anxiety and depressive symptoms, as well as to increase her desire to closely watch over her daughter. Amy’s score on the Beck Anxiety Inventory (described below) was a 15, on the borderline of minimal and mild anxiety symptoms (the cutoff is 16 for mild anxiety symptoms). Amy reported that her anxiety had increased over the past decade as she got older and closer to the “age where people die.” At that initial intake, Amy was also experiencing depressive symptoms including low mood more days than not since the age of 14, frequent tearfulness both with and without a trigger, 26 Clinical Case Studies 20(1) hopelessness, low self-esteem, sleep difficulties, difficulty concentrating and passive suicidality. Amy’s passive suicidal ideation occurred approximately once per week and consisted of thoughts such as “I can’t live like this anymore. I’m too emotionally exhausted.” When she felt depressed, she engaged in ruminative thinking about past losses, such as
- 12. her father’s death, which served to reinforce her depressive cognitions. Amy’s pessimism and low mood caused frequent conflict with her husband, who didn’t see a reason for her to be so sad. This conflict, in turn, reinforced her belief that she would lose those close to her. Her score on the Beck Depression Inventory-II (described below) was a 16, indicative of mild depressive symptoms. Despite the persistence of her low mood, Amy reported other periods of her life when she did not meet full diagnostic cri- teria for a major depressive episode (e.g., she did not have sleep difficulties or difficulty concen- trating in college). Upon presentation.to treatment with this writer, Amy had completed CBT and had seen a notable decrease in her symptoms (see Figure 1). She no longer met diagnostic criteria for a major depressive episode, reporting improvements in sleep, concentration and feelings of hope- lessness. She continued to experience low mood for much of the day on most days, low self- esteem and passive suicidality, as well as resultant rumination and marital conflict. Her Beck Depression Inventory-II score had decreased to an 11, indicative of minimal depressive symp- toms and reflecting a 25 percent change over the course of CBT. Amy’s anxiety symptoms had also decreased. Though she continued to experience obsessive ruminations, particularly about her daughter’s wellbeing, she felt that they were more controllable using her newly developed cognitive restructuring skills. She said that she was successfully able to use cognitive restructur- ing to reduce catastrophizing about half of the time. The
- 13. frequency of her panic symptoms had also decreased. Her score on the Beck Anxiety Inventory was a six, indicative of a 60 percent change and placing her anxiety symptoms firmly in the mild range. However, she also continued to engage in the maladaptive avoidance behaviors described above. In sum, through a course of CBT, Amy was able to reach remission from a major depressive episode and to decrease her symptoms of generalized anxiety disorder. However, she continued to experience a persistent depressive disorder characterized by consistent low mood, low self- esteem and passive suicidality; and to engage in maladaptive coping behaviors such as rumina- tion, catastrophizing and avoidance behaviors. ST is intended to treat patients who, like Amy, Figure 1. Assessment of depressive and anxiety symptoms during CBT treatment. Herts and Evans 27 have largely recovered from anxiety and depressive episodes that can be treated through CBT, but who still have persistent subclinical symptoms that are maintained by maladaptive cognitive and behavioral patterns. Amy was thus appropriate for ST and was consented into treatment. 4 History Amy had a trauma history including extensive loss, sexual
- 14. abuse, emotional abuse and emotional neglect in childhood. Her grandparents , to whom she was close, both died of old age when she was 7 years old. Her father died unexpectedly from a heart attack when she was 12. Amy reported that her mother became increasingly depressed and unable to care for her and her two older sib- lings following her father’s death, spending most of her time alone in her room and rarely inter- acting with the children. Amy took on the role of caring for her mother for a few years, until Amy’s oldest brother and his friend moved home to help. When Amy was 14 years old, she was sexually molested by her brother’s friend. Amy told her mother, who accused her of lying. Later that year, Amy’s brother died in a car accident. Following her brother’s death, Amy’s mother often expressed out loud that she wished it had been Amy who died instead. Amy described her teenage years as a time of no oversight, rife with emotional neglect and abuse by her mother. Amy said that she first became depressed after her brother died at age 14 and had anxiety since childhood. Her depressive symptoms had never fully remitted, indicative of a course of chronic depression that lasted for over 40 years. Amy’s anxiety waxed and waned over time, but became worse in her 50s, which she attributed to ageing and becoming increasingly worried about death. 5 Assessment The Beck Anxiety Inventory, Beck Depression Inventory-II and the Columbia Suicide Severity Rating Scale were administered weekly for routine outcome
- 15. monitoring during treatment and at each of 2 biweekly and 2 monthly follow-up sessions. Beck Anxiety Inventory The Beck Anxiety Inventory (BAI; Beck & Steer, 1990) is a 21- item scale that was developed to address the need for an instrument that would reliably discriminate anxiety from depression while displaying convergent validity. Each item on the scale describes a symptom of anxiety. The respondent is asked to rate how much he or she has been bothered by each symptom over the past week on a 4-point scale ranging from 1 to 3. The items are summed to obtain a total score that can range from 0 to 63. The scale obtained high internal consistency and item-total correlations ranging from 0.30 to 0.71 (median = 0.60) and studies have demonstrated its convergent and discriminant validity. Beck Depression Inventory-II The Beck Depression Inventory-Second Edition (BDI II; Beck et al., 1996) is a 21-item scale and one of the most widely used self-report measures of depression. The psychometric properties of the original BDI are well established, and the BDI-II also appears to be psychometrically strong. Columbia-Suicide Severity Rating Scale The Columbia Suicide Severity Rating Scale (C-SSRS; Posner et al., 2011) demonstrated good convergent and divergent validity with other multi-informant suicidal ideation and behavior
- 16. 28 Clinical Case Studies 20(1) scales and had high sensitivity and specificity for suicidal behavior classifications compared with another behavior scale and an independent suicide evaluation board. Both the ideation and behav- ior subscales were sensitive to change over time. The intensity of ideation subscale demonstrated moderate to strong internal consistency. The Young Schema Questionnaire and the Young Parenting Inventory were administered at baseline to aid in case conceptualization. Young Schema Questionnaire The Young Schema Questionnaire (YSQ-L2; Young & Brown, 2001) is the long form of the self- report measure that assesses 18 maladaptive schemas. Patients rate themselves on how well each item describes them on a 6-point Likert scale. In studies, alpha co-efficients for each schema range from 0.83 to 0.96 and test-retest coefficients range from 0.50 to 0.82 in non-clinical sam- ples. Convergent and discriminant validity and primary factors mapping onto Young’s schemas have been established (Young et al., 2003). Young Parenting Inventory (YPI) The Young Parenting Inventory (YPI; Young, 1994) is one of the primary means of identifying childhood origins of schemas. The YPI is a 72-item
- 17. questionnaire in which respondents rate their mothers and fathers separately on a variety of behaviors that may contribute to schemas. The YPI uses a 6-point Likert scale. 6 Case Conceptualization An ST Case Conceptualization covers five major areas: (1) current symptoms and life problems, for example, maladaptive behavioral patterns; (2) the developmental origins of these problems; (3) current schemas and schema modes, with related maladaptive behaviors; (4) the therapy relationship; and (5) the focus of treatment and plan for change (Young, 2007). As described above, Amy presented to ST with generalized anxiety disorder and persistent depressive dis- order. She reported “obsessive worries” about her own, her husband and her daughter’s health and wellbeing, low mood on most days, low self-esteem and passive suicidality. Amy’s anxiety and depressive symptoms led to significant distress as well as maladaptive behaviors including reassurance seeking to reduce anxiety, irresponsible spending on beauty treatments to combat feelings of defectiveness and avoidance behavior to minimize anxiety-provoking situations. For example, Amy avoided driving out of fear of an accident. In addition, when her daughter had a sports injury that required minor surgery, Amy catastrophized and worried about her resultant death and sought reassurance from her husband and her daughter’s doctors. This served to strain her relationship with her daughter, which was further distressing for Amy. In addition, Amy had a general cognitive style characterized by rumination and
- 18. catastrophizing, which led to conflict in her marital relationship. The developmental origins of these symptoms and maladaptive cognitive and behavioral patterns is best described as an unmet need for feeling connected, accepted and safe in childhood following the deaths of her grandparents, father and brother all before age 14. Amy’s mother’s own resultant depression led her to be unable to care for Amy and meet her emotional needs. Amy’s feeling of safety and acceptance further deteriorated after she was molested by her brother’s friend and not believed by her mother. These unmet needs resulted in Amy’s current schemas: (1) Abandonment; (2) Social Isolation; (3) Defectiveness; (4) Vulnerability to Harm or Illness; and (5) Negativity/Pessimism. Herts and Evans 29 Abandonment/Instability Schema The Abandonment schema involves the belief that significant others will not be able to provide ongoing emotional and practical support because they are unreliable, will die, or will abandon the patient (Young et al., 2003). During treatment, Amy worried that someone in her immediate fam- ily would die and that her daughter would abandon her in favor of a boyfriend. Her avoidance behavior on behalf of herself and her family, such as when she did not want to allow her daughter
- 19. to travel abroad, led her daughter to pull away from her. Her rumination and resultant low mood, as well as her reassurance seeking, led to marital conflict. For Amy, the experiences of her daugh- ter pulling away and her husband engaging in conflict both served to maintain this schema. Social Isolation/Alienation This schema reflects the belief that one is isolated and different from other people (Young et al., 2003). Amy believed that God had singled her out for a life of loss and sorrow that kept her emo- tionally separate from other people. When she shared her ruminations with her husband, he rein- forced the belief that she is different from others by invalidating her resultant low mood. However, Amy continually voiced her ruminations in search of reassurance. Defectiveness/Shame In line with this schema, Amy exhibited worry that she is defective and would be unlovable if exposed. This resulted in low self-esteem and made her feel insecure and ashamed around others, particularly around aspects of her appearance and about her depression. Amy said that her mother frequently criticized her appearance in childhood, and she spent considerable money on main- taining her appearance, for example, by going to an expensive hair salon. She felt very ashamed of this, as she and her husband otherwise felt financially insecure. Vulnerability to Harm or Illness
- 20. This schema was reflected in Amy’s catastrophic fears that an unpreventable tragedy would result in a family member’s death. For her daughter and her husband, these fears focused on medical and external catastrophes, such as her husband having a heart attack, or her daughter being in an airplane crash. For herself, Amy worried about becoming debilitated with depression and committing suicide if anything were to happen to her daughter. When Amy attempted to protect her daughter, she prevented her from engaging in age appropriate behaviors, such as attending field trips, which both angered her daughter and prevented her from gaining increased independence. In addition, this avoidance prevented Amy from experiencing her daughter safely returning from trips, which would have served to combat this schema. Negativity/Pessimism Amy described a lifelong focus on the negative aspects of life and minimization of the positive, which is characteristic of a Negativity/Pessimism schema (Young et al., 2003). Despite the tre- mendous loss she experienced as a child, Amy had many strengths and sources of positivity in her life, including a strong group of friends, a loving husband and daughter and a meaningful career where she felt valued. When she discounted these positive forces, it angered her husband and contributed to marital conflict. Further, Amy worried that she would pass along her depres- sion to her daughter, who also had many strengths.
- 21. These schemas are commonly associated with an enhanced “vulnerable child” mode, in which the patient experiences negative emotions such as sadness and fear (Young et al., 2003). Indeed, 30 Clinical Case Studies 20(1) in experiential exercises Amy was easily able to access her vulnerable child mode. In the therapy relationship, Amy was passive and friendly and frequently sought reassurance about her worries and her performance in treatment. The overarching aim of treatment was to bolster Amy’s “healthy adult” mode, in which she could nurture, affirm and protect the vulnerable child within. The tools of ST were used to achieve this, specifically, the cognitive, behavioral, interpersonal and experiential interventions described below. It was expected that these interventions would result in a significant reduction in Amy’s ongoing anxiety and depressive symptoms on the routine outcome measures, as well as a qualitative improvement in her functioning. 7 Course of Treatment and Assessment of Progress Course of Treatment Amy completed 18 sessions of ST and four follow-up sessions over the course of 9 months. Treatment began with psychoeducation about ST and assessment of Amy’s schemas. Thereafter, treatment incorporated cognitive, behavioral, interpersonal and experiential interventions. The
- 22. follow-up phase of treatment, described below, began once Amy’s depression had remitted. Interpersonal interventions (employed throughout treatment). The primary interpersonal intervention utilized was limited reparenting, which describes using the therapeutic relationship to provide patients with what they needed, but did not get from their parents, in childhood (Young et al., 2003). For Amy, this meant providing unconditional acceptance and positive regard; consistency in keeping appointments, timeliness and responsiveness to questions; and supplying the healthy adult voice through Socratic questioning in cognitive interventions and in real time during early schema dialogue exercises. The following dialogue demonstrates how the therapist provided the healthy adult voice. In this exercise, Amy was asked to first speak from her vulnerable child voice, then to switch chairs and respond from her healthy adult voice. Amy [as vulnerable child]: I’m just so scared. I can’t protect the people I love. Something terrible could happen at any time and I could lose them. Therapist: I’d now like you to move to this chair, here. In this chair, you embody the healthy adult part of yourself. Am I speaking with the healthy adult within Amy? Amy [as healthy adult]: Yes. Therapist: Great. Healthy Adult, the Vulnerable Child has just told us that they are very scared of losing someone they love. What can you say to them to provide comfort and care?
- 23. Amy: I. . .I don’t know. Therapist: That’s ok. Is it ok if I speak for you this time? Amy: Sure. Therapist [faces the vulnerable child chair]: Amy, as a child, it’s not your job to protect the people you love. It’s their job to protect you. I know they haven’t done that for you and I’m sorry. But now I am here to protect you and the people you love and I promise to do so. Therapist [faces Amy in the healthy adult chair]: Amy, can you summarize what I just said in your own words? Amy [as healthy adult, faces vulnerable child chair]: Ok. You don’t have to worry that terrible things will always happen. I know you’ve been scared, but I am here to protect you now. It’s not your job to be the protector anymore. I am here and I will keep you safe. Psychoeducation and assessment (Sessions 1–4). The initial phase of treatment involved additional assessment of Amy’s schemas using the YSQ-L2 and the YPI. Items that Amy endorsed were queried for better understanding. For example, Amy said that “people have not been there to meet Herts and Evans 31 my emotional needs” was “mostly true of me.” The therapist asked for examples of this, which led Amy to describe her mother’s emotional neglect and her
- 24. current perception that nobody truly knows how defective she is. The therapist also led Amy in a guided imagery exercise to help identify the childhood origins of her schemas. In the exercise, the patient is asked to imagine an upsetting situation with one of their parents and how they wish their parent had responded. They are then asked to wipe out that image and think of a current situation in which they have had the same emotional experience (Young et al., 2003). Amy described being sad and infuriated when, in a moment of conflict, her mother told her that she wished Amy had died instead of her brother. She said that she needed her mother to recognize that Amy was grieving her brother’s death, too and that she wanted to be allowed to “fall apart sometimes,” the way her mother always seemed to due to her depression. At the conclusion of the assessment phase of treatment, the therapist provided psychoeduca- tion about ST and collaboratively created the case conceptualization with Amy. Psychoeducation included assigning Amy to read “A Client’s Guide to Schema Therapy” (Bricker & Young, 2004) and sections of “Reinventing Your Life” (Young & Klosko, 1994), a self-help book based on Schema Therapy, that described Amy’s schemas. The therapist and Amy then discussed how each schema applied to Amy’s life at present. The decision to collaboratively complete the case con- ceptualization was made to increase rapport, set the basis for a collaborative treatment relation- ship and to gain further insight into Amy’s perceptions of her history and current functioning.
- 25. Amy participated actively in completing the conceptualization. Cognitive interventions (main focus in sessions 5–10). In the middle section of treatment, cognitive, behavioral and experiential interventions were used whenever needed, though in general cognitive interventions were taught prior to behavioral and experiential interventions. Core beliefs, or sche- mas, were identified at the outset of treatment during the assessment phase. The focus of cognitive interventions was to restructure these beliefs using cognitive restructuring driven by Schema Diaries (Young, 1993) and Schema Flashcards (Young et al., 2003). Schema Diaries allow a patient to track their thoughts, feelings and behaviors in the present day and then connect them to their schemas and childhood origins. The patient is then guided to come up with a healthy alterna- tive belief and behavior. Schema Flashcards are completed for situations and feelings that arise repeatedly, so that the patient can have easy access to a healthy belief and behavioral instruction. Amy completed schema diaries and flashcards throughout treatment. The content of her diaries was largely about worry about her daughter. For example, after meeting her daughter’s boyfriend, Amy worried that he would break up with her and she would become depressed, ultimately com- mitting suicide. Other events that elicited schema-related beliefs also involved threats to those close to her, such as when a dear friend had a heart attack and when her husband lost his job. Early in treatment, Amy was unable to come up with healthy alternative beliefs and behaviors on her own and required the therapist’s assistance through
- 26. limited reparenting. However, over the course of treatment Amy became adept at completing Schema Diaries and Flashcards and reported that the cognitive restructuring that resulted from them was highly effective at mitigat- ing her anxiety. The therapist also regularly engaged Amy in cognitive restructuring of schema- related beliefs that arose in session, first by providing examples of restructured thoughts and then through Socratic questioning to guide Amy to restructure her own thinking. Behavioral interventions (Main focus in sessions 10–12). Behavioral interventions included design- ing behavioral experiments to test maladaptive, schema-related beliefs, as well as imaginal expo- sures to feared experiences. Examples of behavioral experiments are Amy being more vulnerable with close friends to test the belief that they would reject her (they did not); and allowing her daughter increased independence to see if she would be hurt or abandon her (she did not). Imaginal exposures focused on feared events happening to her daughter, such as her getting in a minor car accident. Amy did not complete imaginal exposure homework over the course of three 32 Clinical Case Studies 20(1) sessions and reported that it was too distressing. The therapist and Amy thus collaboratively decided to shift the focus of treatment to experiential interventions.
- 27. Experiential interventions (Main focus in sessions 13–17). There were two types of experiential interventions used in treatment, guided imagery and schema dialogues. First, a guided imagery exercise was conducted to help Amy visualize a safe place that she could return to mentally when schemas were activated. Amy imagined a room in her childhood home and reported that conduct- ing the safe place imagery exercise was comforting. The purpose of imagery and schema dia- logue exercises was to help Amy express schema-related beliefs and emotions and learn to respond to them from a healthy adult perspective. Schema dialogue exercises used imagery to help Amy imagine an upsetting childhood situation, such as her father’s death and speak about her needs from the part of her that represented her “vulnerable child” mode. She was then asked to switch chairs and respond to the “vulnerable child” from her “healthy adult” mode. Amy reported feeling many symptoms of panic and anxiety while in vulnerable child mode, such as perceived tachycardia and sweating. In the dialogue below, Amy successfully responds to the vulnerable child within her with minimal help from the therapist. Amy [as vulnerable child]: Everyone dies and there is nobody to take care of me. I can’t take care of myself. I’m going to go crazy. I should just die, too. Therapist: I’d now like you to move to this chair, here. Please take a moment to access the healthy adult part of yourself – the part that cares for your daughter. Am I speaking with the healthy adult within Amy?
- 28. Amy [as healthy adult]: Yes. Therapist: Great. Healthy Adult Amy, the Vulnerable Child has just told us that she wants to die because there is nobody to care for her. Please respond so as to comfort and care for her. Amy [as healthy adult, faces vulnerable child chair]: I know you have had a lot of loss and I am so sorry about that. But I am here now and I promise to take care of you. You’re not going crazy; you’re just a child and you need adults to care for you—that’s ok. I will be that adult for you. I don’t want you to die—you have so much life left to live and things are only going to get better for you. I promise—I’ve seen it. Figure 2. Assessment of depressive and anxiety sympto ms during ST treatment. Herts and Evans 33 Schema dialogue sessions concluded with processing the exercise and conducting the safe place imagery exercise to help Amy regulate her emotions prior to leaving the session. Unlike exposure, Amy participated fully in schema dialogue exercises. Imagery was also used to help Amy identify the schemas that were driving current maladap- tive behavioral patterns. For example, imagery was helpful when Amy was catastrophizing that her daughter would get in a plane crash and die if she flew to
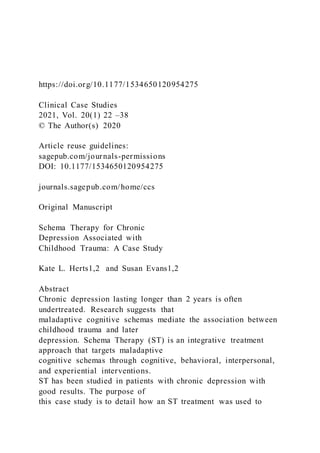
- 29. Israel. Amy was first asked to close her eyes and engage in mindfulness of the emotions she was feeling: panic and despair. She was then guided to imagine a time in her childhood when she had felt the same way. Amy responded that her father had died shortly after flying back from visiting her grandparents. Through this exercise, it became clear that Amy’s Abandonment and Vulnerability to Harm or Illness schemas were activated by her daughter’s upcoming trip because she fel t abandoned and terrified by her father’s unexpected death from a heart attack. By identifying these schemas it was possible to create an effective schema diary to address their current trigger. Assessment of Progress Figure 2 depicts Amy’s scores on the BDI and BAI throughout the course of Schema Therapy. Amy’s scores on the BAI remained low throughout treatment, with a range from three to six, indicative of minimal anxiety symptoms. At termination, her score (BI = 3) had seen a 50 per- cent change since the commencement of ST (BAI = 6). Amy’s scores on the BDI ranged from three at termination to 11 at the commencement of ST, indicative of minimal depressive symp- toms with a 73 percent change over the course of ST treatment. It is notable that Amy’s descrip- tion of her symptoms in session was more severe than was reflected on the BDI and BAI, particularly at the start of ST. Amy’s anxiety symptoms may have been more accurately assessed by a measure that focuses more on worry (as opposed to somatic, as in the BAI) symptoms of anxiety. Amy’s low scores on the BDI may have been
- 30. indicative of a relatively low level of depressive symptoms as compared to other times in Amy’s life, rather than a minimal level of absolute depressive symptoms. It is a limitation of this report that the authors did not identify other quantitative metrics to better capture the negative functional impact of Amy’s depressive and anxiety symptoms. On the CSSRS, Amy consistently endorsed passive suicidal ideation, but denied suicidal plan, intent, or means. In addition, at termination she reported decreased frequency of this ideation from weekly to approximately once per month. Finally, her passive suicidal ideation was no lon- ger general (e.g., I can’t take this anymore), but rather only arose when triggered by the thought of her daughter dying, for example, when Amy saw a news report about a teenager being killed in a park. When triggered, Amy would think “I can’t go on if she dies” but would quickly identify this as her Vulnerability to Harm or Illness schema being activated and engage in cognitive restructuring. Qualitatively, Amy reported that her persistent depression lifted over the course of treatment and that she was happier than she had ever been. She was no longer experiencing low mood on most days and felt more hopeful about the future. Further, she was proud of herself for “graduating” from treatment and reported increased self-esteem as a result. Amy expressed amazement that less than 1 year of ST had helped her remit from 40 years of chronic depression. She no longer engaged in depressive rumination and noticed an accordant
- 31. improvement in her relationship with her husband. Amy also reported that her “obsessive worries” were now only occasional (less than daily) and that she was consistently able to successfully cope with them using cognitive tech- niques learned in ST, rather than catastrophizing. She had reduced her avoidance behaviors and was allowing her daughter increased independence, such as sleeping over at friends’ houses. Amy said that this had both improved their relationship and reduced Amy’s fear that something bad would befall her daughter, as her daughter returned from the sleepovers and other endeavors 34 Clinical Case Studies 20(1) unharmed. The therapist observed that in addition, Amy had increased self-efficacy to manage her mental health, with which Amy agreed. 8 Complicating Factors At the time of Amy’s treatment, there was significant media attention on antisemitism. In October 2018, the New York Times published an article called “Is it Safe to be Jewish in New York?” (Bellafante, 2018) in which they reported that antisemitic events had comprised half of all hate crimes in New York that year. These ranged from drawing swastikas on public property to physi- cal assaults against Hasidic Jews (Bellafante, 2018). That same month, George Soros, a promi- nent Jewish philanthropist, was mailed a pipe bomb just days before 11 congregants were killed
- 32. in a mass shooting at the Tree of Life Synagogue in Pittsburgh (Robertson et al., 2018). Amy, in her work at a Jewish religious organization, became very scared that she would be threatened or attacked at work. She also feared for her family’s physical and emotional wellbeing. The very real, ongoing and public nature of antisemitic activity strongly reinforced Amy’s Vulnerability to Harm or Illness schema. In contrast to past traumas, from which Amy’s healthy adult voice could reassure her of her current safety, there was likely a true increased risk of unknown proportion to Amy, particularly at work. Thus, problem solving was introduced to help Amy identify steps she could take to keep herself safe, for example, by rearranging the furniture at work so she was not directly in front of the door. Problem solving interventions were coupled with cognitive restruc- turing to help Amy de-catastrophize the likelihood of harm occurring from her initial prediction of 95 percent. About 3 months into treatment, Amy received multiple threatening phone calls at work over the course of a two-day period. She effectively reported this to her boss and the police and followed their instructions for how to proceed with answering calls. This adaptive behavior was highlighted to reinforce Amy’s healthy adult mode. 9 Access and Barriers to Care Amy complained of financial distress throughout treatment. Her husband, who had long been a successful business executive, was unemployed and having difficulty finding work. In addition, she herself had a six-month period of unemployment that ended shortly before beginning treat-
- 33. ment with this writer. This was so stressful for Amy that at times she considered leaving her husband and finding a more financially stable partner. Unsurprisingly, Amy was reluctant to pay the $40 copay for ongoing therapy for an extended period of time and this almost prevented her from entering ST, which typically lasts between 6 months and 2 years. The therapist encouraged Amy to discuss the copay with her husband to see if they realistically could continue to pay it and offered to file a request for a fee reduction with the clinic director if the answer was no. The thera- pist also provided the rationale that ST, if effective, might result in a remission of symptoms and enhance the quality of her life, which Amy had never experienced in over a decade of past ther- apy. Amy and her husband ultimately decided to work the copay into their ongoing budget in order to prioritize Amy’s mental health. 10 Follow-up Follow-up: Relapse Prevention and Final Termination (Sessions 18–22) Amy reported that her depressive and anxiety symptoms had decreased significantly by session 15 and remained consistently low throughout the rest of treatment. This was in line with her scores on the BDI (see Figure 2). Thus, we ended standard treatment to begin both relapse pre- vention planning and tapering treatment at session 18. Relapse prevention planning consisted of reviewing the cognitive, behavioral and imagery skills learned in treatment, as well as the
- 34. Herts and Evans 35 learning from other experiential interventions. Tapering consisted of meeting every other week from sessions 18 to 20, and then monthly for sessions 21 and 22. This allowed Amy to practice skills outside of therapy and process termination with the therapist after having a break from treatment. Amy said that the cognitive restructuring skills that she learned in ST were of great value to her, as was the learning from experiential interventions. Upon initially tapering treat- ment, Amy expressed great sadness and an uptick in maladaptive thoughts related to the Abandonment schema. The therapist guided Amy to respond to those thoughts using her Healthy Adult voice, which instructed her that this was a healthy goodbye wholly unlike past situations where those close to her died. At the final termination session, the therapist and Amy celebrated Amy’s great progress and Amy expressed pride that she was ready to “graduate” from therapy. 11 Treatment Implications of the Case Chronic depression is a psychiatric condition with significant impact on the function and quality of life of millions of people. While medication and CBT are effective for a percentage of people suffering from chronic depression, there are many who remain refractory to these gold standard approaches to care. Of significance, is that early life events, including the death of a parent or sibling, as well as childhood trauma (i.e., abuse, neglect) may
- 35. play a role in the development of chronic depression as mediated through maladaptive schemas. Targeting early disconnection schemas such as abandonment, mistrust/abuse and emotional deprivation stemming from these experiences may be of critical importance in optimizing treatment for patients with chronic depression. Amy’s case demonstrates a partial response to a standard CBT approach focusing on cognitive restructuring, behavioral activation and coping skills for chronic depression. Nonetheless, Amy continued to endorse feelings of low self-esteem and hopelessness at the end of treatment and she remained obsessively worried about the health of her family, including her daughter. Her worries were associated with maladaptive behavioral patterns aimed at keeping her daughter safe from harm, but in fact they reinforced an enmeshed and dependent relationship. The major treatment implication of this case is through furthering her work in ST, Amy was able to experience and process her core sense of vulnerability and to cultivate healthier and more adaptive beliefs includ- ing that the significant relationships in her life were secure and stable. This case also demonstrates the importance of constructing a case conceptualization to guide the therapy process. Early on in ST, the therapist and Amy examined specific life situations that revealed patterns of obsessive thoughts around the safety of family members. It was important for Amy to understand that early life events and traumas contributed to the development of her
- 36. core beliefs that “the world is a dangerous place” and “you can’t trust people for being there in a stable and consistent way.” She was able to understand how these beliefs were linked to a certain assumptions, “If I don’t watch out and worry all the time, something bad will happen” and also specific rules, “I have to protect everyone.” The conceptualization allowed Amy to develop a deeper awareness of how her constant anxiety, worry and obsessive efforts to protect her daugh- ter and other family members functioned to maintain her underlying fears of abandonment, loss and feeling unsafe. Amy improved from a course of CBT and further benefitted from the experiential processing and healing of early life wounds that was addressed in ST. Nonetheless, it should be noted that Amy continued to endorse passive suicidal ideation at the end of treatment. We know that Amy internalized the harsh/critical voice of her mother telling her that she wished Amy had died instead of her brother. It remains unclear if Amy’s passive suicidal ideation will remain intrac- table or if it will diminish with time if she continues to experience greater self-confidence and a sense of safety in the world. 36 Clinical Case Studies 20(1) 12 Recommendations to Clinicians and Students ST should be considered in patients who exhibit chronic maladaptive life patterns that are linked
- 37. to early life events and are not currently impaired by symptoms concurrent with an active anxiety or depressive disorder. In patient who do have an active anxiety or depressive disorder, a tradi- tional course of CBT may be the most appropriate therapeutic option. Other indications for con- sidering ST are for patients, such as Amy, who may have experienced a partial remission of symptoms from a standard course of CBT and remain mildly symptomatic and continue to engage in maladaptive behavioral patterns. ST may also be considered for patients suffering from personality disorders, including borderline and narcissistic personality disorder. Supervision Techniques The supervisee should work with a clinician who has trained in ST, has experience supervising other clinicians and who will be able to guide them in understanding the underlying conceptual model behind ST in concert with learning about the eighteen schemas and maladaptive copying styles that maintain schemas. The trainee started by reading Schema Therapy: A practitioner’s guide (Young et al., 2003). Learning to conduct ST parallels the course of patient treatment; therefore, the supervisee began with understanding the assessment and education phase of ST. The supervisee first learned to take a life history and identify current problematic life patterns and patient goals. The supervisor instructed the beginning schema therapist to administer and score the YSI and query the patient on individual high scores to further elucidate potential sche- mas. It was useful to conduct imagery exercises with the
- 38. supervisee, including the assessment imagery exercise. The supervisee was able to draw on her experience of memories with her own parents as the supervisor guided her through the exercise. Cognitive, behavioral and experiential strategies were practiced in supervision. For example, the supervisee brought in a schema diary that their patient completed to review with the supervisor to get specific feedback. It was particu- larly helpful to role play the experiential techniques in supervision. For example, the supervisor first modeled how to conduct the imagery exercises aimed at accessing greater affect and insight into schemas. Then the supervisee practiced guiding the supervisor through an imagery exercise. As treatment progressed, supervisor and supervisee practiced dialogues (sometimes using chair work) to differentiate between the schema side and the healthy side. Time in supervision was allotted to debriefing the supervisee’s experience with these techniques and particularly the more experiential strategies such as imagery exercises and schema dialogues. Declaration of Conflicting Interests The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Funding The author(s) received no financial support for the research, authorship, and/or publication of this article. ORCID iD
- 39. Kate L. Herts https://orcid.org/0000-0002-7967-327X References Beck, A. T., Rush, A. J., Shaw, B. F., & Emery, G. (1979). Cognitive therapy of depression. Guilford Press. Beck, A. T., & Steer, R. A. (1990). Beck anxiety inventory manual. The Psychological Corporation. Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Comparison of the Beck depression inventories-IA and II in psychiatric outpatients. Journal of Personality Assessment, 67, 588–597. https://orcid.org/0000-0002-7967-327X Herts and Evans 37 Bellafante, G. (2018, October 31). Is it safe to be Jewish in New York? The New York Times. https:// www.nytimes.com/2018/10/31/nyregion/jewish-bias-safety- nyc.html?searchResultPosition=2 Bricker, D. C., & Young, J. E. (2004). A client’s guide to schema therapy. Cognitive Therapy Center of New York. Byllesby, B. M., Elhai, J. D., Tamburrino, M., Fine, T. H., Cohen, G., Sampson, L., Shirley, E., Chan, P. K., Liberzon, I., Galea, S., & Calabrese, J. R. (2017). General distress is more important than PTSD’s cognition and mood alterations factor in accounting for PTSD and depression’s comorbidity. Journal of Affective Disorders, 211, 118–123.
- 40. Contractor, A. A., Greene, T., Dolan, M., & Elhai, J. D. (2018). Relations between PTSD and depression symptom clusters in samples differentiated by PTSD diagnostic status. Journal of Anxiety Disorders, 59, 17–26. Cuijpers, P., van Straten, A., Schuurmans, J., van Oppen, P., Hollon, S. D., & Andersson, G. (2010). Psychotherapy for chronic major depression and dysthymia: A meta-analysis. Clinical Psychology Review, 30(1), 51–62. David, D., Cristea, I., & Hofmann, S. G. (2018). Why cognitive behavioral therapy is the current gold standard of psychotherapy. Frontiers in Psychiatry, 9(4). doi: 10.3389/fpsyt.2018.00004 Ferrari, A. J., Charlson, F. J., Norman, R. E., Patten, S. B., Freedman, G., Murray, C. J., Vos, T., & Whiteford, H. A. (2013). Burden of depressive disorders by country, sex, age, and year: Findings from the global burden of disease study 2010. PLoS Medicine, 10(11), e1001547. Gurak, K. K., Freund, B., & Ironson, G. (2016). The use of both prolonged exposure and cognitive pro- cessing therapy in the treatment of a person with PTSD, multiple traumas, depression, and suicidality. Clinical Case Studies, 15(4), 295–312. Hiraoka, R., Cook, A. J., Bivona, J. M., Meyer, E. C., & Morissette, S. B. (2016). Acceptance and commit- ment therapy in the treatment of depression related to military sexual trauma in a woman veteran: A case study. Clinical Case Studies, 15(1), 84–97.
- 41. Hölzel, L., Härter, M., Reese, C., & Kriston, L. (2011). Risk factors for chronic depression - A systematic review. Journal of Affective Disorders, 129, 1–13. Hovens, J. G., Giltay, E. J., Wiersma, J. E., Spinhoven, P., Penninx, B. W., & Zitman, F. G. (2012). Impact of childhood life events and trauma on the course of depressive and anxiety disorders. Acta Psychiatrica Scandinavica, 126(3), 198–207. Kocsis, J. H., Gelenberg, A. J., Rothbaum, B., Klein, D. N., Trivedi, M. H., Manber, R., Keller, M. B., Howland, R., & Thase, M. E. (2008). Chronic forms of major depression are still undertreated in the 21st century: Systematic assessment of 801 patients presenting for treatment. Journal of Affective Disorders, 110, 55–61. Malogiannis, I. A., Arntz, A., Spyropoulou, A., Tsartsara, E., Aggeli, A., Karveli, S., Vlavianou, M., Pehlivanidis, A., Papadimitriou, G. N., & Zervas, I. (2014). Schema therapy for patients with chronic depression: A single case series study. Journal of Behavior Therapy and Experimental Psychiatry, 45, 319–329. Mandelli, L., Petrelli, C., & Serretti, A. (2015). The role of specific early trauma in adult depression: a meta-analysis of published literature. Childhood trauma and adult depression. European Psychiatry, 30(6), 665–680. Posner, K., Brown, G. K., Stanley, B., Brent, D. A., Yershova, K. V., Oquendo, M. A., Currier, G. W., Melvin, G. A., Greenhill, L., Shen, S., & Mann, J. J. (2011).
- 42. The Columbia-Suicide Severity Rating Scale: Initial validity and internal consistency findings from three multisite studies with adolescents and adult. The American Journal Psychiatry, 168(2), 1266– 1277. Renner, F., Arntz, A., Peeters, F. P. M. L., Lobberstael, J., & Huibers, M. J. H. (2016). Schema therapy for chronic depression: results of a multiple single case series. Behav Ther Ex Psychiatry, 51, 66–73. Rezaei, M., & Ghazanfari, F. (2016). The role of childhood trauma, early maladaptive schemas, emo- tional schemas and experimental avoidance on depression: A structural equation modeling. Psychiatry Research, 246, 407–414. Robertson, C., Mele, C., & Tavernise, S. (2018, October 27). 11 Killed in Synagogue Massacre; Suspect Charged with 29 Counts. The New York Times. https://www.nytimes.com/2018/10/27/us/active- shooter-pittsburgh-synagogue- shooting.html?searchResultPosition=4 https://www.nytimes.com/2018/10/31/nyregion/jewish-bias- safety-nyc.html?searchResultPosition=2 https://www.nytimes.com/2018/10/31/nyregion/jewish-bias- safety-nyc.html?searchResultPosition=2 https://www.nytimes.com/2018/10/27/us/active-shooter- pittsburgh-synagogue-shooting.html?searchResultPosition=4 https://www.nytimes.com/2018/10/27/us/active-shooter- pittsburgh-synagogue-shooting.html?searchResultPosition=4 38 Clinical Case Studies 20(1)
- 43. Seavey, A., & Moore, T. M. (2012). Schema-focused therapy for major depressive disorder and personality disorder: A case study. Clinical Case Studies, 11(6), 457–473. Spijker, J., van Straten, A., Bockting, C. L., Meeuwissen, J. A., & van Balkom, A. J. (2013). Psychotherapy, antidepressants, and their combination for chronic major depressive disorder: A systematic review. The Canadian Journal of Psychiatry, 58(7), 386–392. Torpey, D. C., & Klein, D. N. (2008). Chronic depression: Update on classification and treatment. Current psychiatry reports, 10(6), 458–464. Wiersma, J. E., Hovens, J. G., van Oppen, P., Giltay, E. J., van Schaik, D. J., Beekman, A. T., & Penninx, B. W. (2009). The importance of childhood trauma and childhood life events for chronicity of depression in adults. Journal of Clinical Psychiatry, 70(7), 983–989. Young, J. E. (1993). The schema diary. Cognitive Therapy Center of New York. Young, J. E. (1999). Cognitive therapy for personality disorders: A schema-focused approach (rev.ed.). Professional Resources Press. Young, J. E. (2007). Schema therapy case conceptualization form. Schema Therapy Institute. Young, J. E., & Brown, G. (2001). Young schema questionnaire: Special Edition. Schema Therapy Institute. Young, J. E., & Klosko, J. S. (1994). Reinventing your life: The breakthrough program to end negative
- 44. behavior and feel great again. Penguin Putnam Inc. Young, J. E., Klosko, J. S., & Weishaar, M. E. (2003). Schema therapy: A practitioners guide. The Guilford Press. Young, J. E., Wattenmaker, D., & Wattenmaker, R. (2003). Schema therapy flashcard. Schema Therapy Institute. Author Biographies Kate L. Herts is an assistant professor of Psychology in Clinical Psychiatry at Weill Cornell Medicine and an Assistant Attending Psychologist at New York Presbyterian Hospital. Dr. Herts completed her Bachelor of Arts at Brown University and earned her PhD in Clinical Psychology from the University of California, Los Angeles. Susan Evans is a professor of Psychology in Clinical Psychiatry at Weill Cornell Medicine and an Attending Psychologist at New York Presbyterian Hospital. She is the Director of Education in Psychology and Director of the Cornell Cognitive Therapy Clinic. She received her PhD from the New School for Social Research.