2. OBJECTIVES
• Review of anatomy
• Define pericarditis
• Etiology & pathophysiology
• Clinical manifestations
• Diagnostic evaluation studies
• Medical and surgical management
• complications
• Nursing management
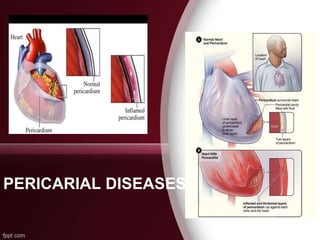
3. INTRODUCTION
• Pericardium • The pericardium is
a sac made up of outer fibrous
pericardium – inner serous
pericardium (parietal & visceral)
separated by a (potential) space,
the pericardial cavity.
• the pericardial cavity contains 15
to 50 mL of an ultra filtrate of
plasma.
4. Functions of Pericardium
1. Stabilization of the heart within the thoracic cavity --
limiting the heart’s motion.
2. Protection of the heart from mechanical trauma and
infection.
3. The pericardial fluid functions as a lubricant and
decreases friction of cardiac surface.
4. Prevention of excessive dilation of heart. (e.g. acute aortic
or mitral regurgitation).
6. DEFINITION
• Pericarditis: is a
condition caused by
inflammation of the
pericardial sac.
• Pericarditis can be
acute or chronic.
7. • Acute pericarditis occurs due to
complications of infections or even as a
result of heart attack.
• Chronic pericarditis is less common form of
constrictive pericarditis. It can also develop
as primary illness / as a result of medical
and surgical disorders.
8. CHRONIC PERICARDITIS
Chronic pericarditis occurs when the layers
adhere to each other causing fibrosis of the
pericardial sac.
It restricts movement of the heart. So the
fibrosis pericardium tightens the heart
decreasing cardiac filling and output.
It leads the patient reports the symptoms of
heart failure.
9. ETIOLOGY
ETIOLOGICAL CLASSIFICATION - TUMOR
• T = Trauma, Tumour , Neoplasm
• U = Uraemia
• M = Myocardial infarction (acute)
• Medications (hydralazine)
• O = Other infections (viral, bacterial, fungal, TB)
• R = Rheumatoid arthritis, autoimmune disorder/
hypersensitivity
11. CLINICAL MANIFESTATIONS
• Chest pain beneath the clavicle, in the neck
region worsens with deep inspiration, relieved
with sitting or leaning forward.
• Mild fever, chills and night sweats.
• Malaise, myalgia
• Dyspnea due to constriction or cardiac
tamponade
12. DIAGNOSTIC FINDINGS
• Patient history
• Physical examination ( pericardial friction
rub by auscultation).
• ECG (ST changes)
• Chest X – ray
• ECHO
• Blood test – Elevated WBC,CRP,ESR
• Pericardial biopsy - analysis
15. ETIOLOGY
• Idiopathic
• Post cardiac surgery
• Post radiation therapy
• Post infectious – tuberculus /purulent
pericarditis
• Others – malignancy, trauma, uremic
pericarditis, asbestosis.
16. PATHOPHYSIOLOGY
CONSTRICTIVE PERICARDITIS
A thickened, fibrotic pericardium forms a
non-compliant shell around the heart.
Ventricles are encased by thick
pericardium
It prevents the heart from expanding when
blood enters in it.
It interferes ventricular filling.
18. DIAGNOSTIC EVALUATION
• ECG – Flattened / inverted T waves
• Chest X – Ray (Pericardial
calcification)
• ECHO cardiogram ( Pericardial
thickening)
19. PERICARDIAL EFFUSION
Accumulation of fluid between the
visceral and parietal layers of serous
pericardium.
•Serous – Transudative (CHF, Renal failure)
•Suppurative – Pyogenic infection.
•Hemorrhagic – occurs with any type of
pericarditis – especially with infections
and malignancies.
20. ETIOLOGY
• Inflammation from infection, immunologic
process.
• Trauma causing bleeding in pericardial space.
• Noninfectious conditions such as:
a. increase in hydrostatic pressure e.g.
congestive heart failure.
b. increase in capillary permeability e.g.
hypothyroidism.
21. ETIOLOGY…………
c. decrease in plasma oncotic pressure
e.g. cirrhosis
• Decreased drainage of pericardial fluid
due to obstruction of thoracic duct as a
result of malignancy or damage during
surgery.
22. CLINICAL FEATURES
• Usually asymptomatic
• Can have signs of compression -
dyspnoea, dysphagia, hoarseness of
voice, hiccoughs, nausea
• Signs : muffled heart sounds paradoxically
reduced intensity of rub
23. • Chest x ray - distinguish
between pericardial
effusion and cardiomegaly.
– Water bottle sign
Electrocardiogram
Echocardiogram
24. MANAGEMENT
• Diuretics & salt restriction
• Digoxin for sinus tachycardia to slow the
ventricular rate.
• Beta blockers & calcium channel blockers
Surgical management
• Pericardiectomy
25. NURSING ASSESMENT
• Physical assessment to obtain the base
line data.
• Vital signs.
• Assess patient in various positions in order
to detect pain whether it is influenced by
respiratory movements, coughing and
swallowing.
26. NURSING ….
• Assess Heart and Lung Sounds
May hear a pericardial friction rub,
muffled heart sounds, or extra sounds because of
the pressure being placed on the hear
• Assess and Address Oral Hygiene
There is a significant connection between
oral health and pericarditis. Bacteria can travel to
the heart easily from the oral cavity. Patients
should brush their teeth twice daily to prevent
complications.
27. NURSING INTERVENTIONS
• Pain management – elevate head end to
45 deg.
• Anti inflammatory drugs as prescribed.
• Monitor complications
28. NURSING DIAGNOSIS
• Ineffective breathing pattern related to chest pain.
• Altered thermoregulation , hyperthermia, related to infection
and inflammation as evidenced by temp.
• Pain related to inflammation of the pericardium.
• Risk for cardiogenic shock related to decreased cardiac
output.
• Ineffective tissue perfusion related to decrease blood flow.
• Anxiety related to therapeutic interventions and uncertainty
of prognosis.
29. NURSING MANAGEMENT
• Explain every procedure to the patient in order to
get consent, cooperation and array anxiety.
• Position patient in semi fowlers to relieve pain
and allow expansion of chest for effective
breathing.
• Explain the pathophysiology to the patient.
• Encourage gradual increase activity.
• Monitor vital signs closely to detect infections.
30. NURSING MANAGEMENT
• Educate patient on signs and symptoms of
infection.
• Educate patient to inform the need
prophylactic antibiotics.
• No dental procedures for at least 6 months.
31. COMPLICATIONS
• Pericarditis progresses to heart failure.
• Pericardial effusion fluid collection in
pericardial space.
• Cardiac tamponade - it develops when
pericardial effusion increases.
32. REFERENCES
• Smeltzer S.C, Bare B.G. & Hinke J.L
(1999). Brunner & Suddarth’s textbook of
medical surgical nursing. (9th E.D).
Philadelphia: J.B. Lippincott
• Linton A.D (2007) Introduction to medical
– surgical nursing. (4th ed) Saunders
Elsevier.