Retinopathy of Prematurity
•Download as PPTX, PDF•
6 likes•371 views

Retinopathy of Prematurity

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Retinopathy of Prematurity
Similar to Retinopathy of Prematurity (20)
Recently uploaded
Recently uploaded (20)
Retinopathy of Prematurity
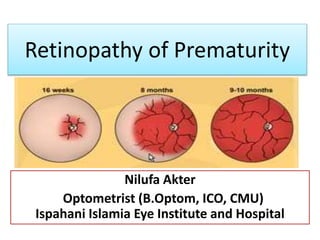
- 1. Retinopathy of Prematurity Nilufa Akter Optometrist (B.Optom, ICO, CMU) Ispahani Islamia Eye Institute and Hospital
- 2. Retinopathy of Prematurity • Is a bilateral abnormal proliferation of the retinal blood vessels in eyes of newborn infants in whom retinal vascularization is incomplete.
- 3. Incidence • Overall incidence: 16-17% for all premature infants • 68% ROP in BW <1250gm • 98% among those having BW <750gm
- 4. Risk Factors of ROP 3 Crucial risk factors: -Low gestational age <32 wks -Low Birth weight (<1500gm) -Supplemental O2 therapy Other risk factors: -Multiple child birth -Respiratory Distress Syndrome (RDS) -Blood transfusions -Fluctuation in SaO2 -Intra Uterine Growth Retardation (IUGR) -Multiple apneic episodes -Hypercarbia, Acidosis - Intra Ventricular Hge (IVH) -Vit E deficiency -Anemia -Seizures
- 5. Embryology of Retinal Blood Vessels
- 6. Pathogenesis of ROP Prematurity Incomplete retinal vascularization When exposure to increased O2 Immature vessels may be occluded (Vasoconstriction) by high O2 concentration Formation of Ischemic retinal vessels Peripheral retinal ischemia –increased metabolic demands, the O2 regulated VEGFs and non-O2 regulated IGF-1 are produced in excess resulting Neovascularization and fibrous proliferation of Retina
- 7. Role of VEGF and IGF-1 in the Pathogenesis of ROP
- 8. Clinical features of ROP ICROP (2005)- is based on: 1.Location (Zone) 2. Stage 3. and Extent. 1. Location(ZONE):- Retina is divided into 3 Zones, with optic nerve as the center.
- 9. 2. Staging of ROP (1-5) • Stage- 1: (Demarcation line)
- 12. Stage-4a:- Partial detachment not involving macula. Stage-4b:- Partial detachment involving the macula. Stage-4: (Partial RD)
- 13. 1. Open-Open funnel 2. Open-Narrow funnel 3. Narrow-Open funnel 4. Narrow-narrow funnel Stage-5: Total RD
- 14. 3. Extent of ROP • Divide the retinal surface into 12 segments (clock hours) • Stage of retinopathy can vary among segments.
- 15. Other features 1. Plus disease 2. Pre-plus disease 3. Aggressive posterior ROP (AP-ROP) 4. Threshold disease 5.Pretheshold disease : 2 types (Type-1 and Type-2)
- 16. 1. Plus disease • Venous dilatation or arteriolar tortousity in at least 2 quadrant. • Poor pupil dilatation • Vitreous haze • Vascular engorgement of the iris • Hallmark of rapidly progressive ROP
- 17. 2. Pre-Plus disease • Is labeled when venous dilation and arterial tortuosity is more than normal but insufficient to be defined as plus disease.
- 18. 3. Aggressive Posterior ROP(AP-ROP) • Is a severe form of ROP that rapidly causes TRD. • Direct AV shunting • Neovascularization may be Flat, featureless
- 19. 4. Threshold disease • If 5 or more contiguous or 8 cumulative clock hours (30 degree) of stage 3 with plus disease in either zone 1 or 2 are present. • Chances of blindness (50%).
- 20. 5. Pre-threshold ROP ETROP group has classified prethreshold disease into 2 types: Type-1: (High risk prethreshold disease)- Treatment is recommended within 72 hours. Zone-1: Plus disease, any stage Zone-2: Non-plus disease, stage3 Zone-3: Plus disease stage2 and stage3 Type-2: (Low risk prethreshold disease)-Requires observation Zone-1: Nonplus disease, stage1 and2 Zone-2: Nonplus disease stage 3
- 21. Differential Diagnosis of ROP 1. Retinoblastoma 2. Cataract 3. PHPV 4. Familial Exudative vitreoretinopathy (FEVR) 5. Coat’s disease 6. Endophthalmitis 7. Chronic vitreous hge 8. Retinochoroidal coloboma
- 22. Management of ROP 1. Screening of risk babies 2. Diagnosis 3. Decision to treat or not 4. Medical Treatment a. Cryotherapy(Mostly outdated) b. Laser treatment (gold standard) c. Anti-VEGF(adjuvant) before laser and Surgery Correction of systemic factors Rx of ROP related complication 5. Post treatment follow up 6. Low Vision Management/Rehabilitation
- 23. Screening Whom to Screen? 1. Birth weight<1500gm 2. Gestational age <32wks 3. Between 1500-2000gm or gestational age >30wks if they have been ill (RDS, Hypotension, Surgery) 4. Need for cardio respiratory support 5. Prolonged O2 therapy 6. Apnea of prematurity 7. Neonatal sepsis 8. If thought by the neonatologist to be high risk
- 24. How to screen? Preparation: -Prior informed and written consent from parents -Temperature controlled room -Ensure stability of infants Dilatation of pupil: Phenylephrine 2.5% and Tropicamide 0.5% 1 drop of Tropicamide every 10-15 minutes for 4times
- 25. Procedure Performed by Experienced Ophthalmologist • Indirect Ophthalmoscopy using 20D/28D lens • Scleral depression is done to stabilize the eye, indent it and contrast retina (For Plus Disease) • Wire Speculum to keep the eyelids apart
- 26. Record Keeping • Identification Data • Gestation, birth • Risk factors • Date of first screening • Findings of ROP • Date of follow up
- 27. Wide field digital camera (Retcam) for Screening • Alternative to indirect Ophthalmoscope • Provide retinal images at 130 degree • High cost, limitation in diagnostic sensitivity, specificity and accuracy.
- 28. Medical Treatment 1.Cryotherapy (Mostly outdated) 2. Laser Treatment(Gold standard) 3. Anti-VEGF (adjuvant) before laser and surgery 4. Surgery
- 29. 1. Cryotherapy
- 30. 2. Laser Therapy • Laser Photocoagulation: Diod (red 810nm) or frequency doubled Nd:YAG (532nm) with LIO delivery should be carried out in all pts with high risk prethreshold, threashold and AP-ROP.
- 31. 3. Anti-VEGF Treatment Anti-VEGF:- Bevacizumab (Avastin) -Ranibizumab (Lucentis) Adjunctive therapy: Injection to allow regression beyond Zone 1 - Laser for recurrent ROP - Anti-VEGF as a bridge to laser peripherally Perioperative Therapy before surgery: - Reduce bleeding -Promote regression of neovascularization -Vitrectomy and Scleral Buckles
- 32. 4. Surgery
- 33. Scleral Buckle • Done under GA • Peritomy • 2.5mm encircling band passed beneath 4 Recti • One anchoring mattress suture applied in all quadrant • Removal after 3-6 months
- 34. Vitrectomy • Necessary in advance cases • Lensectomy avoided • Peeling of membrane • Relief of traction
- 35. Low Vision Management 1. High amount of myopic Refractive error can be corrected with conventional spectacles or contact lenses. 2. Magnification with microscopes, magnifiers 3. Electronic magnification systems and telesopic devices 4. Various Tints and Filters may be useful in decreasing photophobia 5. Increased, direct, nonglare illumination is helpful at near 6. May also benefit from Field awareness systems and mobility services if their peripheral field have been affected.
- 36. References 1. Comprehensive Ophthalmology-by A.K Khurana 2. Clinical Ophthalmology- By Kanski’s Bowling 3. Essentials of Low Vision Practice-by Richard L.Brilliant 4. American Academy of Ophthalmology 5. Internet