Longitudinal Analysis of Factors Predicting Receipt of Treatment for Opioid Use Disorder in Redeployed Army Service Members Assigned to Warrior Transition Units, FY2008-2015
•
0 likes•18 views

Longitudinal Military Health System data were analyzed from redeployed active duty Army service members (n=15,544) who were assigned to Warrior Transition Units (WTUs), FY2008-2015, to identify factors predicting OUD treatment.
Recommended

Recommended
More Related Content
What's hot
What's hot (19)
Similar to Longitudinal Analysis of Factors Predicting Receipt of Treatment for Opioid Use Disorder in Redeployed Army Service Members Assigned to Warrior Transition Units, FY2008-2015
Similar to Longitudinal Analysis of Factors Predicting Receipt of Treatment for Opioid Use Disorder in Redeployed Army Service Members Assigned to Warrior Transition Units, FY2008-2015 (20)
Recently uploaded
Recently uploaded (20)
Longitudinal Analysis of Factors Predicting Receipt of Treatment for Opioid Use Disorder in Redeployed Army Service Members Assigned to Warrior Transition Units, FY2008-2015
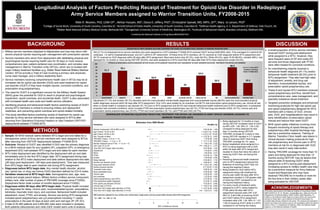
- 1. Longitudinal Analysis of Factors Predicting Receipt of Treatment for Opioid Use Disorder in Redeployed Army Service Members assigned to Warrior Transition Units, FY2008-2015 Nikki R. Wooten, PhD, LISW-CP1 , Akhtar Hossain, MS2, Diana D. Jeffery, PhD3, Christopher Spevak, MD, MPH, JD4,5, Mary Jo Larson, PhD6 1College of Social Work, University of South Carolina, Columbia SC. 2Arnold School of Public Health, University of South Carolina, Columbia SC. 3Defense Health Agency, U. S. Department of Defense, Falls Church, VA. 4Walter Reed National Military Medical Center, Bethesda MD. 5Georgetown University School of Medicine, Washington DC. 6Institute of Behavioral Health, Brandeis University, Waltham MA. Funded by the National Institute on Drug Abuse #K01DA037412 Military service members deployed to Afghanistan and Iraq may return with severe physical injuries requiring pain management with prescription opioids. Service members who return from deployment with debilitating physical and psychological injuries requiring health care for 30 days or more receive comprehensive care, patient-centered care coordination, and complex case management in Warrior Transition Units (WTUs), which are co-located with major military treatment facilities (e.g. Walter Reed National Military Medical Center). WTUs provide a Triad of Care involving a primary care physician, nurse case manager, and a military leadership team. Service members receiving comprehensive health care in WTUs may be at increased risk for opioid use disorder (OUD) and need treatment for opioid use disorder (OUDT) if they have multiple injuries, comorbid conditions, and prescription drug polypharmacy. The need for OUDT is a significant concern for the Military Health System (MHS) given the potential for OUD to result in physical and psychological impairment, opioid overdose, and accidental death. OUDT is also associated with increased health care costs and health service utilization. Identifying physical and behavioral health factors predicting receipt of OUDT among WTU members is critical to ensuring military and deployment readiness, and preventing opioid overdose and opioid-related mortality. This study identified factors predicting receipt of treatment for opioid use disorder by Army service members who were assigned to WTUs after returning from Operations Enduring Freedom or Iraqi Freedom (OEF/OIF) deployments between FY2008-2015. BACKGROUND This study was funded by the National Institute on Drug Abuse (NIDA #K01DA037412, PI: Dr. Wooten, nwooten@sc.edu). Data are from the Department of Defense Military Health System Data Repository. Dr. Jeffery is the Defense Health Agency’s project officer who sponsored access to these data. Laura Hopkins of Kennell & Associates, Inc. created data extracts utilized for this study. The opinions and assertions herein are those of the authors and do not necessarily reflect the official views of the U. S. Department of Defense, NIDA, the Defense Health Agency, or the National Institutes of Health. ACKNOWLEDGEMENTS A small proportion of Army service members received OUDT during post-deployment while assigned to a WTU. However, they were frequent users of OP and costly ED services and those diagnosed with PTSD were often treated for comorbid conditions. An overwhelming majority received a behavioral health diagnosis (91.1%) and/or behavioral health treatment (82.5%) prior to WTU assignment. They also had high rates of adjustment, anxiety, and drug use disorders, musculoskeletal injuries, and prescription opioid polypharmacy use. These ill and injured WTU members received opioid polypharmacy and thus, benefit from comprehensive care, case management, and specialty substance abuse treatment. Targeted prevention strategies and enhanced monitoring protocols for high risk opioid use and opioid polypharmacy designed for WTU members with a history of OUD, chronic pain, DUD, and hospitalizations may result in early identification of prescription opioid misuse and reduce their need OUDT. MHS opioid safety initiatives involving more frequent monitoring of opioid therapy and polypharmacy after hospital discharge may also be a preventive measure. Training of Warrior Transition Clinic health care teams in clinical decision making protocols for high risk polypharmacy and chronic pain in WTU members at risk for or diagnosed with OUD may also result in early intervention. Having TRICARE coverage for more than 10 years and being deployed for less than 12 months during OEF/OIF may be factors that reduce odds of receiving OUDT while assigned to a WTU during post-deployment. Increasing access to military health care may be a preventive measure for Army National Guard and Reservists who may have received TRICARE for 9 months or more for the first time in their military career after being activated for OEF/OIF. DISCUSSION Sample: All MHS medical claims between WTU begin and end dates for a retrospective cohort of Army service members who were assigned to WTUs after returning from OEF/OIF deployments between FY2008-2015. Outcome: Receipt of OUDT was identified if OUD was the primary diagnosis on a MHS medical claim for any inpatient (IP), outpatient (OP), or emergency department (ED) visit between WTU begin and end dates for each member. WTU index deployment was identified by the deployment with an end date immediately prior to the first WTU begin date. WTU assignment timing was relative to the WTU index deployment end date (before deployment end date, <90 days post-deployment, >90 days post-deployment). Time was measured from WTU begin date to each medical visit during WTU assignment. Diagnoses before WTU begin date: Any mental health disorder; alcohol use, opioid use, or drug use (minus OUD) disorders defined by ICD-9 codes. Variables measured at WTU begin date: Demographics (sex, age, race, marital and single parent status). Military factors (military service component, military rank, total number of years of TRICARE coverage since FY2002). Deployment factor (total number of months deployed since FY2002). Diagnoses within 90 days after WTU begin date: Physical health included any diagnoses for sleep, chronic pain, musculoskeletal injuries, amputations, blindness, traumatic brain injury, and overdose. Behavioral health included adjustment, mood, PTSD, and anxiety. Service use during WTU assignment included opioid polypharmacy use (>4 prescriptions including >1 opioid prescriptions in the past 30 days at each visit) and visit type (IP, OP, ED). A total of 25,385 patients and 4,660,064 visits were included in analyses. Both patients (descriptives) and visits (GEE model) were units of analysis. METHODS RESULTS 530 (2.1%) of redeployed Army service members who were assigned to a WTU between FY2008-2015 received OUDT during 8,648 MHS visits. They averaged 5.5 (sd=6.8) ED visits/year, 1.6 (sd=2) hospitalizations/year, and 20.7 (sd=8.4) OP visits/month. Of these Army WTU members, 28.1% received an OUD diagnosis before WTU assignment and 38.7% received an OUD diagnosis within 90 days after WTU assignment. Most were Active duty (67.2%), male (94.5%), White (93.4%), ages 18-39 (86.6%), enlisted (96%), had deployed for 12 months or more during OEF/OIF (53.6%), and were assigned to a WTU more than 90 days after their WTU index deployment ended (54.9%). Adjustment (71.7%) and anxiety (78.1%) disorders were the most prevalent mental health diagnoses and musculoskeletal injuries (88.9%) were the most prevalent physical health diagnoses received within 90 days after WTU assignment. Only 3.6% were treated for an overdose, but 68.7% had prescription opioid polypharmacy use. Almost all had either a mental health or substance use disorder (91.1%) prior to WTU assignment and 82.5% had received behavioral health treatment prior to WTU assignment. A substantial proportion had comorbid conditions, which included PTSD and prescription opioid polypharmacy use (35.7%), PTSD and drug use disorder (DUD; 34.7%), chronic pain and prescription opioid polypharmacy use (33.0%), PTSD and mood disorders (32.1%), and PTSD and OUD (24.7%). 71.7 78.1 46.6 50.9 55.7 26 62.6 39.3 88.9 39.3 0 10 20 30 40 50 60 70 80 90 100 ADJUSTMENT ANXIETY MOOD PTSD SLEEP ALCOHOL USE DX DRUG USE DX TBI MUSCULOSKELETAL CHRONIC PAIN GENERALIZED ESTIMATING EQUATIONS PREDICTING TREATMENT FOR OPIOID USE DISORDER IN ARMY SERVICE MEMBERS ASSIGNED TO WARRIOR TRANSITION UNITS % of U. S. Army WTU members receiving OUDT, FY2008-2015 Being deployed for 12 months or more during OEF/OIF increased odds of OUDT by 84% (OR: 1.84, 95% CI: 1.04-3.25) compared to being deployed for less than 12 months during OEF/OIF. TRICARE coverage for 4 years or less during OEF/OIF resulted in 3.71 greater odds of receiving OUDT than having TRICARE coverage for 10+ years. Being hospitalized while assigned to a WTU or being diagnosed with a DUD within 90 days after WTU assignment resulted in more than twice the odds of receiving OUDT than not having this history. Receiving behavioral health treatment prior to WTU assignment reduced the likelihood of receiving OUDT than not having this treatment history. Being treated for OUD before WTU assignment along with treatment for chronic pain within 90 days after WTU assignment resulted in 3.60 greater odds of receiving OUDT compared to not having this treatment history. For every month of treatment while assigned to a WTU, being treated for PTSD within 90 days after WTU assignment reduced odds (OR: 0.97, 95% CI: 0.95-0.99) of receiving OUDT and OUDT before WTU assignment increased odds (OR: 1.05, 95% CI: 1.01- 1.09) of receiving OUDT while in a WTU compared to not having this history. PHYSICAL & BEHAVIORAL HEALTH DIAGNOSES WITHIN 90 DAYS AFTER WARRIOR TRANSITION UNIT ASSIGNMENT IN ARMY MEMBERS RECEIVING TREATMENT FOR OPIOID USE DISORDER DESCRIPTION OF ARMY MEMBERS RECEIVING TREATMENT FOR OPIOID USE DISORDER WHILE ASSIGNED TO WARRIOR TRANSITON UNITS ***p < .0001. **p < .005. *p < .05. GEE model also adjusted for race, military rank, marital status, single parent, and any mental health disorder before WTU assignment. ***p < .0001. **p < .005. *p < .05. * * * * * *** ** * * ***