
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Postpartum Nursing Care
Similar to Postpartum Nursing Care (20)
Recently uploaded
Recently uploaded (20)
Postpartum Nursing Care
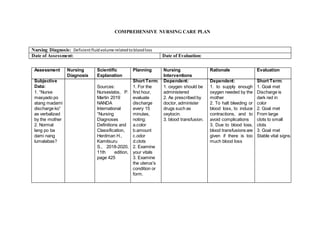
- 1. COMPREHENSIVE NURSING CARE PLAN Nursing Diagnosis: Deficientfluidvolume relatedtobloodloss Date of Assessment: Date of Evaluation: Assessment Nursing Diagnosis Scientific Explanation Planning Nursing Interventions Rationale Evaluation Subjective Data: 1. “Nurse masyado po atang madami discharge ko” as verbalized by the mother 2. Normal lang po ba dami nang lumalabas? Sources: Nurseslabs, P. Martin 2019 NANDA International “Nursing Diagnoses Definitions and Classification, Herdman H., Kamitsuru S., 2018-2020, 11th edition, page 425 Short Term: 1. For the first hour, evaluate discharge every 15 minutes, noting: a.color b.amount c.odor d.clots 2. Examine your vitals 3. Examine the uterus's condition or form. Dependent: 1. oxygen should be administered 2. As prescribed by doctor, administer drugs such as oxytocin. 3. blood transfusion. Dependent: 1. to supply enough oxygen needed by the mother 2. To halt bleeding or blood loss, to induce contractions, and to avoid complications 3. Due to blood loss, blood transfusions are given if there is too much blood loss Short Term: 1. Goal met Discharge is dark red in color 2. Goal met From large clots to small clots 3. Goal met Stable vital signs.
- 2. Objective Data: 1. Irritability 2. Rigid Uterus 3. Incision on the abdomen (low segment incision) 4. Vital Signs: Temperature: 36.7 ℃ Pulse: 85 bmp Respiration: BP: 140/90 Oxygenation: 90 Blood loss: 1,200 ml Long Term: 1. vital signs will be stable after 8 hours of monitoring 2. Correct pattern of lochia Independent: 1. Asses excessive bleeding and immediately call the doctor 2. weighing all of the mother's perineal pads to assess the amount of blood 3. Providing instruction to the pt. If she passes clots, she should notify the nurse noting of their size and amount. 4. oxygen should be administered 5. Uterine massaging 6. Care for the Perineum 7. lochia color, quantity, and pattern health education 8. encourage mother for breastfeeding Independent: 1. Excessive bleeding should be reported to the doctor for further investigation. 2. To find out how much blood has been lost. 3. Uterine contractions are indicated by a considerable number of clots. 4. 1-2 liters of oxygen are administered by nurses via nasal cannula. 5. Contractions and bleeding can be avoided by massagingthe uterine fundus. 6.Changing per pads and using a Sitz bath, as well as wiping from front to back, limit the spread of microorganism existing in the anus. 7. Pt. will benefit from health education Long Term: 1. Goal met, after 6 hours, the lochia flow is within normal range until discharge. 2. Goal met, no unpleasant odor was detected 3. Goal met Patients show understanding of the optimal lochia color, amount, and pattern, which will be reported if possible.
- 3. 9. monitor the rate of involution and check the color including amount of discharge 10. check REEDA on the abdominal incision site 11. assess vital signs every15 minutesfor the firsthour after surgery,every30 minutesforthe next2 hours,everyhourfor the next4 hours,or as specificallyordered( Collaborative: 1. Removal of left parts of clots 2. Examine WBC count, hemoglobin and hematocrit levels regarding discharges to reported by any unfavorable findings 8. 9. Collaborative: 1.To stop the excessive bleeding 2. Infection is indicated by a rise in WBC.
- 4. Nursing Diagnosis: Activity intolerance related to CS secondary to surgical incision as evidenced by lying on bed all the time Date of Assessment: February 15, 2022 Date of Evaluation: February 17, 2022 Assessment Nursing Diagnosis Scientific Explanation Planning Nursing Interventions Rationale Evaluation Subjective Data: 1.“ wala po ako gana mag galaw- galaw, gusto ko naka higa lang” as verbalized by the mother 2. “masakit pa kase tong operasyon ko nurse” as the mother added 3. mother verbalized that she is having discomfort and difficulty performing ADL’s 4. 7/10 pain scale Activity intolerance related to CS secondary to surgical incision as evidenced by lying on bed all the time Insufficient physiological or psychological energy to endure or complete required or desired daily activities. Source: - NANDA International “Nursing Diagnoses Definitions and Classification, Herdman H., Kamitsuru S., 2018-2020, 11th edition, page 246 Short Term: 1.For 10 minutes, conduct interview to the mother about her feelings and pain sensations 2. For 10 hours monitor vital signs 3. After 12 hours of nursing interventions the mother will be able to verbalized the activities that she cannot perform and factors that contributes to immobility 4. After 24 hours, mother Dependent: 1. Administer non- opiod analgesic 500 mg as ordered through IV 2. Order stool softener Dependent: 1.Promotes comfort by blocking sensations. IV infusion is used for post-partum CS mothers since they are NPO for 6-8 hours 2.Stool softeners are used to avoid constipations in order for the mother to tolerate bathroom activities Short Term: 1.Goal partially met, interview was done but mother was a not totally verbally responsive. 2. Goal met, vital signs were assessed within normal unit with a Vital Sign: Temperature- 36.5 degrees Celsius BP- 125/80 mmHg Pulse- 90 bpm RR- 24 bpm 3. Goal met, mother was able to verbalized
- 5. will be able to perform limited activities with assistance factors that contributes activity intolerance 4. Goal partially met, after 24 hours’ postpartum mother was able to perform several ADL’S with complete assistance and wants to just lei and rest in bed. Objective Data: 1. Incision on the abdomen (low segment incision) 2. Patient is always lying on bed 3. Needs assistance when performing activities of daily living Long Term: 1.After 4 days of hospitalization and nursing intervention, patient will be able to perform tolerance in doing ADL’s as evidenced by being able to sit and comb her hair and Independent: 1. Assessmother’s vital indicators,such as: a. temperature b.heartrate c.bloodpressure d. usage of accessory muscles e.skincolor 2.Encourage mother to complete activity at a slowerpace, overa longerperiod Independent: 1. A motherwhois showingsignsof shockor postpartum hemorrhage should be referred immediately.If motherisgoinginto shock,herblood pressure istoolow and falling,andher pulse rate istoo highand rising.If Long Term: 1. Goal partially met, after 4 days of hospitalization and nursing intervention, patient was able to perform tolerance in doing several ADL’s as evidenced by
- 6. Vital Sign: Temperature- 37.5 degrees Celsius BP- 125/80 mmHg Pulse- 90 bpm RR- 24 bpm walk during rooming in of time,withmore restand interruptions,orwith assistance 3. Promote bedrest and assistpatientto lie supine for8 hours afterspinal anesthetic 4. For 10 to 15 minutes,assist patienttodangle legs fromthe bedside 5. As preferredbythe patient,provide a commode at the bedside 6. Promote an increase activity graduallybydoing active range-of- motionexercisesin bed,thensittingand finallystanding 7. Assistmotherin herADLs while remaining independentof the patient. 8. Promote non- pharmacologic measureslike there are no signsof bleedingfromthe vaginal area,she may be losingblood inside 2.It promotes developmentof tolerance forthe activity 3. To regain strength and energy 4.It prevents orthostatic hypotensionfrom occurring 5. Using a commode consumesless energythanusinga bedpanor walking to the bathroom 6. Overexertionis avoidedby graduallyincreasing the activitylevel or intensity.Passive range of motionis importantfor maintainingmuscle and jointflexibility by allowingmuscles to move passively 7. Assistingthe patientwithADLs being able to sit and comb her hair but when walking and in doing some activities like walking during rooming in and carrying her baby she still needs assistance.
- 7. changinginposition and arrangingbed linenscanhelp promote comfort 9. Instruct and encourage the womanto walk duringroomingin 10.Patientmustbe tiltedleftandright every6-10 hours. Checktensioninthe calf and humansign 11. Promote early mobilizationmaydo ismove the arm, hand,move the toe and ankle twisting, elevatingthe heel, calf musclestight,as well asbendingand slidingthe footinthe first6 hours postpartum 12. Instructthe postpartummother on energy-saving techniques,suchas sittingtobrush teeth or comb hair,and performingtasksata slowerspeed. conservesenergy; carefullybalance assistance; facilitatinggrowing endurance will improve the patient’sactivity tolerance andself- esteem 8. In orderfor the motherto notrely to painmedications 9. It is the bestway to ease gas pain 10. To avoid thrombosisand embolismfrom occurringor Deep veinthrombosis (DVT) 11. Early ambulation makesmotherfeel healthierand stronger.By mobilizingregular bloodcirculation/ smooth,the danger of thrombosisand thromboembolism can be reduced. Usedto strengthen musclesand joints inorder to conduct activities
- 8. 13. Astolerated, elevate the headof the bed 14. Assesspain scale 15. Teach motheras she feedsthe baby to put a pillowonher lap. 16. Football holdfor breastfeeding 12. Energy-saving strategieshelpto equalize oxygen supplyanddemand by loweringenergy consumption 13. Improveslung expansionforbetter oxygenationand cellularabsorption 14. Enable patient to rate the severity of herpain 15. to alleviatepain by shiftingthe infant’sweight away fromthe suture line 16. a technique for keepingthe baby’s weightoff the mother’sincision Collaborative: 1.As needed,seek physical/occupational treatment. 2.Involve and encourage S.Oin assistingthe needfor additional assistance at home Collaborative: 1.May be required/desiredin orderto design individualized exercise/progressive activityprograms 2.In aidingthe patientin conservingenergy, coordinatedefforts ismore effective
- 9. COMPREHENSIVE NURSING CARE PLAN Nursing Diagnosis: Date of Assessment: Date of Evaluation: Assessment Nursing Diagnosis Scientific Explanation Planning Nursing Interventions Rationale Evaluation Subjective Data: Short Term: 1. Dependent: 1. Dependent: 1. Short Term: 1. Objective Data: 1 Long Term: 1 Independent: 1. Independent: 1. Long Term: Collaborative: 1. Collaborative: COMPREHENSIVE NURSING CARE PLAN Nursing Diagnosis: Date of Assessment: Date of Evaluation: Assessment Nursing Diagnosis Scientific Explanation Planning Nursing Interventions Rationale Evaluation Subjective Data: Short Term: Dependent: Dependent: Short Term:
- 10. 1. 1. 1. 1. Objective Data: 1 Long Term: 1 Independent: 1. Independent: 1. Long Term: Collaborative: 1. Collaborative: COMPREHENSIVE NURSING CARE PLAN Nursing Diagnosis: Date of Assessment: Date of Evaluation: Assessment Nursing Diagnosis Scientific Explanation Planning Nursing Interventions Rationale Evaluation Subjective Data: Short Term: 1. Dependent: 1. Dependent: 1. Short Term: 1. Objective Data: 1 Long Term: 1 Independent: 1. Independent: 1. Long Term: Collaborative: Collaborative:
- 11. 1. COMPREHENSIVE NURSING CARE PLAN Nursing Diagnosis: Date of Assessment: Date of Evaluation: Assessment Nursing Diagnosis Scientific Explanation Planning Nursing Interventions Rationale Evaluation Subjective Data: Short Term: 1. Dependent: 1. Dependent: 1. Short Term: 1. Objective Data: 1 Long Term: 1 Independent: 1. Independent: 1. Long Term: Collaborative: 1. Collaborative: COMPREHENSIVE NURSING CARE PLAN Nursing Diagnosis: Date of Assessment: Date of Evaluation: Assessment Nursing Diagnosis Scientific Explanation Planning Nursing Interventions Rationale Evaluation Subjective Data: Short Term: Dependent: Dependent: Short Term:
- 12. 1. 1. 1. 1. Objective Data: 1 Long Term: 1 Independent: 1. Independent: 1. Long Term: Collaborative: 1. Collaborative: COMPREHENSIVE NURSING CARE PLAN Nursing Diagnosis: Date of Assessment: Date of Evaluation: Assessment Nursing Diagnosis Scientific Explanation Planning Nursing Interventions Rationale Evaluation Subjective Data: Short Term: 1. Dependent: 1. Dependent: 1. Short Term: 1. Objective Data: 1 Long Term: 1 Independent: 1. Independent: 1. Long Term: Collaborative: Collaborative:
- 13. 1. COMPREHENSIVE NURSING CARE PLAN Nursing Diagnosis: Date of Assessment: Date of Evaluation: Assessment Nursing Diagnosis Scientific Explanation Planning Nursing Interventions Rationale Evaluation Subjective Data: Short Term: 1. Dependent: 1. Dependent: 1. Short Term: 1. Objective Data: 1 Long Term: 1 Independent: 1. Independent: 1. Long Term: Collaborative: 1. Collaborative: