
Recommended
More Related Content
What's hot
What's hot (20)
Similar to CA HYPOPHARYNX.pptx
Similar to CA HYPOPHARYNX.pptx (20)
More from Dr Monica P
Recently uploaded
Recently uploaded (20)
CA HYPOPHARYNX.pptx
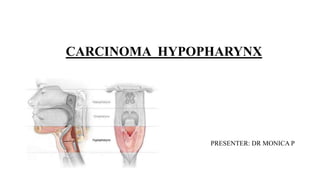
- 1. CARCINOMA HYPOPHARYNX PRESENTER: DR MONICA P
- 2. CONTENTS: • ANATOMY • INTRODUCTION • EPIDEMIOLOGY AND ETIOLOGY • PROGNOSTIC FACTORS • PATHOLOGY • PATTERNS OF SPREAD • CLINICAL PICTURE, EVALUATION AND STAGING • MANAGEMENT • RADIATION THERAPY SIMULATION, CONVENTIONAL AND CONFORMAL PLANNING • RT TECHNIQUES, FRACTIONATION, PLAN EVALUATION • TRIALS IN HYPOPHARYNX CANCER • SIDE-EFFECTS OF RT • ROLE OF RT IN PALLIATIVE SETTING • RECURRENCE
- 3. ANATOMY: • The hypopharynx, or laryngopharynx, is the longest and most inferior portion of the 3 segments of the pharynx and links the oropharynx to the esophagus. • It is located posterior to the cartilaginous structures of the larynx. • Hypopharynx extends from the level of hyoid bone and vallecula to the cricopharyngeus [or inferior margin of cricoid cartilage on imaging studies], corresponding to C4 through C6 vertebral bodies. • 3 major anatomical subsites: Pyriform sinuses [paired recesses lateral to the larynx], Post-cricoid area, Posterior pharyngeal wall. • Oropharynx lies above, cervical esophagus below, larynx anterior and medially, and retropharyngeal space posteriorly. • Function of hypopharynx: to guide the food into the esophagus and away from the larynx during normal swallowing.
- 4. Pyriform sinuses Post cricoid region Posterior pharyngeal wall • inverted pyramid shaped, with apex at the level of cricoarytenoid joint. • with the medial, lateral and anterior walls narrowing inferiorly to form the apices. • Posteriorly, pyriform sinuses are open and contagious with the pharyngeal walls. • Superiorly, the sinuses are surrounded by the thyrohyoid membrane through which the internal branch of the superior laryngeal nerve passes. • Tumor involvement of the sensory branches of internal br. Of superior laryngeal nerve causes referred otalgia. • It extends from the level of arytenoid cartilages to the inferior border of cricoid cartilage • Its composed of the mucosa overlying the cricoid cartilage, with the arytenoid and esophageal mucosa forming the superior and inferior borders, respectively. • It extends from the level of vallecula to the level of cricoarytenoid joints. • It predominantly comprises the squamous mucosa covering the middle and inferior pharyngeal constrictor muscles and is separated from the prevertebral fascia by the retropharyngeal space. • Typically, mucosa lining the pharyngeal wall is <1cm thick and provides a minimal barrier to direct tumor infiltration. • Posterior pharyngeal wall is contiguous with the lateral wall of the pyriform sinuses.
- 5. • Sensory innervation of hypopharynx: internal branch of superior laryngeal nerve, fibres deriving from glossopharyngeal nerve. • Primary motor supply: recurrent laryngeal nerve and pharyngeal plexus • Arterial supply of hypopharynx: branches of external carotid artery (superior thyroid arteries, ascending pharyngeal arteries and lingual arteries). • Lymphatics: Drain directly through the thyrohyoid membrane and into the jugulodigastric lymph nodes, Most commonly involving subdigastric node. Additional- into spinal accessory nodes. Tumors involving posterior pharyngeal wall can also drain into retropharyngeal nodes, including the most cephalad retropharyngeal nodes of Rouviere.
- 6. EPIDEMIOLOGYAND ETIOLOGY: • Hypopharynx cancers account for 5.2% of upper aerodigestive tract cancers • Majority of hypopharyngeal cancers originate in the pyriform sinus. Postcricoid carcinomas are uncommon. • Tobacco and alcohol use are clearly associated with the development of hypopharyngeal cancer. • The risk of hypopharyngeal and oropharyngeal cancer may be especially high in patients with inactive or less active forms of the ADH1B & ALDH2 enzymes. • Occupational exposure to coal dust, steel dust, iron compounds and fumes increased risk for developing hypopharynx cancer.
- 8. • Long term exposure causes: Progressive cellular dysregulation by alteration of tumor suppressor genes such as TP53 Amplification of proto-oncogenes such as cyclin D1 Damage to regulatory factors such as TGF-beta and retinoic acid receptors. • Approximately 20-25% of patients with hypopharynx cancer test positive for HPV DNA • Seropositivity for antibodies against HPV-16 E6 & E7 antibodies are associated with a significantly elevated risk of hypopharyngeal cancer. • Increased risk of developing cancers of postcricoid region for patients with: Plummer-Vinson syndrome. o Its characterized by iron deficiency anemia, hypopharyngeal webs, weight loss and dysphagia.
- 9. PROGNOSTIC FACTORS: • Age >70yrs unfavorable predictor of outcome • Women have improved outcomes compared to men • Tumor location pyriform sinus generally faring better than postcricoid or posterior pharyngeal wall cancers. • Hypopharynx cancer patients fare poorly in comparison with patients harboring tumors from other head and neck sites. • Tobacco, alcohol, medical comorbidities and dietary factors may also impact on outcome.
- 10. PATHOLOGY: • Squamous cell carcinoma (>95%) • 1/3rd of pyriform sinus cancer are non-keratinizing type and 40% are poorly differentiated. • Basaloid variant of SCC occasionally arises in the hypopharynx and is associated with an aggressive biologic behavior and poor prognosis. • Other rare tumors of hypopharynx: Minor salivary gland tumors, sarcomas (fibrosarcoma, liposarcoma, synovial cell sarcoma, malignant fibrous histiocytomas), lymphomas.
- 11. Local extension Arising from pyriform sinus: Arising from postcricoid region: Arising from posterior pharyngeal wall: • spread superiorly to involve aryepiglottic folds and arytenoids, invade paraglottic and preepiglottic space. • extend circumferentially to involve cricoid cartilage • superiorly extend to involve oropharynx • Lateral extension: involves portions of thyroid cartilage, lateral compartment of neck. • Anteriorly involve larynx results in vocal cord fixation. • Inferiorly cervical esophagus • Arising from medial wall: involves pyriform sinuses, intrinsic muscles of larynx causing vocal cord fixation. • Involves pyriform sinus, trachea, esophagus • Posteriorly prevertebral fascia and retropharyngeal space. • Inferiorly extends beyond the apex, involves thyroid gland. PATTERNS OF SPREAD:
- 12. REGIONAL DISEASE: LYMPHATICS: PHARYNGEAL WALLS PYRIFORM SNUS • Primarily: jugular chain • Secondarily: level V nodes • Most often involved: level II • Primarily: jugular chain with small proportion to level V nodes. • Most often involved: level II • Level III can be involved without level II metastases. • At diagnosis: 75% have positive nodes clinically, and ~10% have bilateral nodes.
- 13. Distant metastases Field cancerization • Most common site: lung • Carcinogens can induce dysplastic changes throughout the mucosa of the upper aerodigestive tract, leading to an increased risk for field cancerization that enhances the likelihood of synchronous or metachronous secondary primary tumors. • Incidence of distant metastases increases notably with the length of time following initial treatment • ~7% of patients will manifest second primary tumor at initial diagnosis • 10-20% will develop secondary primary tumor over time.
- 14. CLINICAL PRESENTATION: • Main presenting symptoms: hoarseness of voice, odynophagia, neck mass. • Tumors lateralized to lateral pharyngeal wall or pyriform sinus: unilateral sore throat dysphagia (hallmark of postcricoid carcinoma) ear pain (tumor pressing or invading internal branch of superior laryngeal nerve) voice changes (involvement of larynx or RLN) • Lesions of apex of pyriform snus or post-cricoid are: pooling of secretions indicates obstruction of the gullet. • Arytenoid edema and inability to see into the apex of pyriform sinus may be observed. • Dysphagia and weight loss frequently occur with locally advanced disease. • Airway obstruction requiring emergency tracheostomy in 5-10% cases in very advanced stages.
- 15. PRETREATMENT EVALUATION AND STAGING WORKUP: • History : Duration of symptoms, presence of otalgia, changes in voice quality, degree of dysphagia, amount of weight loss. Previous H/O another upper aerodigestive tract malignancy H/O tobacco, smoking • Physical examination: Direct and indirect visualization of the full laryngopharyngeal axis with particular attention to size, location and anatomic positioning of primary tumor, mobility status of true vocal cords. • Dentition and oral health should be assessed. • Neck examination: to note the size, number, location, texture and mobility of cervical adenopathy. • FNA biopsy of cervical adenopathy
- 16. Imaging: • CE-CT or CE-MRI extending from skull base to below the clavicle : to assess the extent of the primary tumor and to quantitatively and qualitatively assess cervical adenopathy. • Chest X-ray (to assess for pulmonary metastasis) • 18-FDG PET CT imaging is increasingly used to assess the extent of regional adenopathy and survey for the presence of distant metastasis.
- 21. MANAGEMENT: • Key consideration in determining the favored approach for these patients is the likelihood and motivation to preserve laryngopharyngeal function.
- 22. SURGERY: T1 & T2 tumors: • Indications for primary surgical management of patients with early cancer of hypopharynx are: history of previous head and neck irradiation organ conservation approaches possible patients who refuse radiation Selected T1 & T2 tumors may need surgical excision. • Favorable subsites include: upper pyriform sinus, posterior pharyngeal wall • Relative contraindications to organ conservation surgery for carcinoma hypopharynx are: cartilage invasion vocal cord fixation post-cricoid invasion deep pyriform sinus invasion extension beyond the larynx
- 23. • The organ preserving surgeries are: Transoral laser microsurgery [TLM] Transoral robotic surgery [TORS]
- 24. T3 & T4 resectable tumors: • Most T3 & T4 hypopharynx cancers treated surgically will require total laryngectomy with efforts to preserve a posterior strip of the hypopharynx spanning the oropharynx to the esophagus. • For more bulky tumors of carcinoma hypopharynx total laryngopharyngectomy [removal of the larynx and entire hypopharynx] is required. • This procedure creates a gap between the oropharynx and esophagus that must be reconstructed with a tubed fasciocutaneous flap such as the radial forearm free flap or anterolateral thigh flap, a free jejunum or a tubed pedicled myocutaneous flap.
- 25. TYPES OF SURGERIES IN T3 & T4 CARCINOMA HYPOPHARYNX Vertical hemi-laryngectomy, or frontolateral vertical partial laryngectomy. Partial Laryngopharyngectomy Total Laryngopharyngectomy • Bisects larynx and removes 1/2 of thyroid cartilage, a portion or all of one True vocal cord and up to 1/3 (5 mm) of other true vocal cord • For small medial and anterior pyriform sinus lesion • For more advanced hypopharyngeal lesions • Removal of false vocal cords, epiglottis, aryepiglottic folds, pyriform sinus • But true vocal cords are preserved • Total laryngectomy with removal of variable amount of pharyngeal wall
- 26. Surgery Radiation Advantages • Less long term tissue damage • Better followup examination • Reserve RT for recurrence • Pathologic staging Disadvantages • Postop rehabilitation • Conversion to Total laryngopharyngectomy Advantages • Avoid operative morbidity/mortality • Reserve surgery for salvage Disadvantages • More long term tissue damage • More difficult followup exam • Chondroradionecrosis • Cannot be used again for recurrence or second primary • Surgical salvage more difficult
- 27. DEFINITIVE RADIATION THERAPY: T1& T2 TUMORS: • Curative RT is generally preferred treatment option for patients with T1 or T2 tumors. • It affords good potential for organ preservation without compromise in clinical outcome. T3 & T4 TUMORS: • Patients who are technically resectable but may not undergo surgery are: Age >70s, Significant medical co-morbidities or patient unwillingness to accept total laryngectomy • In unresectable cases: curative radiation or chemoradiation is often pursued. • Contraindications for surgery: o Cartilage invasion o Vocal Cord fixation o Post Cricoid invasion o Deep Pyriform invasion o Extension beyond larynx
- 28. RADIATION THERAPY: CONVENTIONAL RADIATION TEHRAPY: o SIMULATION: • Supine position • Neck should be maximally extended on a headrest that fits the patient well with the chin positioned superiorly. • Shoulders should be displaced inferiorly as such as possible to maximize the utility of lateral portals in treatment delivery. • Immobilization by using a custom-made mask [made of thermoplastic material, eg: aquaplast] o Portals are: opposed lateral photon fields and low anterior neck photon field and posterior cervical electron fields.
- 29. OPPOSED LATERAL PHOTON FIELDS ADDITIONAL SHAPING SUPERIOR BORDER 1.5cm above the cranial border of C1 [to include retropharyngeal and junctional nodes] INFERIOR BORDER [As low as possible without entrance beam going through the shoulder: ] atleast 2cm below inferior edge of the cricoid cartilage to include the apex of the pyriform sinus ANTERIOR BORDER 1-1.5cm beyond the skin surface [to include thyroid cartilage in its entirety, and anterior soft tissues. For posterior pharyngeal wall primary tumor, this border may be placed just posterior to the skin surface to exclude a small strip of anterior skin] POSTERIOR BORDER Upto 45Gy- just beyond posterior spinous process of C2 After 45Gy- curved border along the middle of vertebral bodies of cervical spine. [if tumor extends to/arises from posterior pharyngeal wall- posterior border should be placed at posterior edge of vertebral bodies using a split beam technique with 6MV photons] ADDITIONAL SHAPING With Cerrobend blocks to exclude spinal cord at posteroinferior aspect of field, as well as oral cavity, a portion of mandible, and cerebellum CONE-DOWN FIELD 2 After 54Gy to exclude regions of neck only at risk for having microscopic disease [additional Cerrobend blocking is added to the superior aspect of field to exclude region of RPLN, occasionally thin strips of blocking are also added to anterior and inferior aspects of field]
- 30. LOW ANTERIOR NECK [LAN] FIELD SUPERIOR BORDER Matched on skin to inferior border of opposed lateral fields. The spinal cord at the junction of fields is blocked in the upper fields. INFERIOR BORDER With low risk of mediastinal disease below heads of clavicles with blocking inferior to inferior aspect of clavicles. With high risk of mediastinal disease 5cm below head of clavicles, with lateral blocking extended inferiorly so that mediastinal portion of field is about 8cm wide. LATERAL BORDERS Positioned to exclude lateral 1/3rd of clavicles POSTERIOR ELECTRON STRIPS MATCHED ON SKIN TO OFF-CORD PHOTON FIELDS
- 31. Digitally reconstructed radiograph depicting a classical lateral field designed to encompass the T2 pyriform sinus cancer . plus bilateral cervical lymphatics from skull base to cricoid, with a matching anterior low-neck field to extend the lymphatic coverage to the level of the clavicle • Due to the high likelihood of subclinical nodal metastases even in the cN0 neck, patients traditionally receive comprehensive radiation to encompass nodal regions from the skull base to the clavicle. • Due to varying thicknesses of the head and neck, custom compensators or wedges should be used for the lateral fields to improve dose homogeneity. • Shrinking field techniques to spare direct spinal cord dose after ~45Gy, as well as final mucosal reductions after 54- 60Gy are often appropriate with posterior neck boosting, with electrons to supplement posterior chain nodal dosing without excessive dose to the spinal cord.
- 32. CONFORMAL RADIATION THERAPY: CT SIMULATION: • Using 3mm slice thickness with IV contrast to delineate the primary tumor, gross lymphadenopathy and additional regions at risk. • Extent: from vertex to carina with isocenter generally placed immediately above the arytenoids. • Patient is immobilized with thermoplastic head and neck mask with shoulder pull board. • Neck should be maximally hyperextended to pull as much of oral cavity and mandible out of the field as possible. • Shoulders should be pulled inferiorly to minimize the risk of beam interference.
- 33. TARGET VOLUME DELINEATION AND TREATMENT PLANNING: TARGET VOLUMES DEFINITION AND DESCRIPTION GTV 70 Primary: all gross disease on physical examination and imaging Neck nodes: all nodes >/=1cm in SAD, grossly abnormal as well as suspicious LN should be contoured as GTV CTV 70 No margin or 5mm margin to GTV 70 PTV 70 10mm margin to CTV 70 for primary tumor CTV 70 + 3-5mm margin for lymph nodes Suggested dose/# : 2Gy/# to 70Gy TARGET VOLUMES DEFINITION & DESCRIPTION CTV 59.5 Primary: entire CTV 70 +1cm margin, include: entire subsite of involved hypopharynx and adjacent superior and inferior structures. Larynx from hyoid to cricoid is included in high risk CTV 59.5 Adjacent fat spaces [preepiglottic fat and prevertebral fascia] are included in CTV 59.5 Neck nodes: atleast 3mm margin on CTV 70 LN regions. I/L level Ib-IV + lateral RPLN, V [if gross level II-IV LN present] PTV 59.5 CTV 59.5 + 3 to 5mm High-risk subclinical dose: 1.7Gy/# to 59.5Gy TARGET VOLUMES DEFINITION & DESCRIPTION CTV 56 C/L level II-IV, RPLN PTV 56 CTV 56+ 3 to 5mm Lower-risk subclinical dose: 1.6Gy/# to 56Gy
- 34. Principles of radiation techniques: • IMRT or other conformal techniques [3DCRT, helical tomotherapy, VMAT] and proton beam therapy[PBT] may be used as appropriate depending on the stage, tumor location, physician training/experience, and available physics support. • FDG PET/CT or MRI [primary imaging] can be fused in treatment planning. • Advanced RT technologies [IMRT, VMAT, helical tomotherapy, IGRT, PBT] may offer clinically relevant advantages in specific instances to spare important OARs and decrease the risk for late normal tissue damage while still achieving the primary goal of local tumor control. • Image guidance is required to provide assurance of accurate daily delivery. Anatomical changes including rapidly shrinking tumors, changes in air cavities or significant weight loss may necessitate repeat diagnostic imaging and replanning [Adaptive treatment].
- 35. FRACTIONATION: • SIB technique uses differential dose painting [66-72Gy to gross disease, 44-63Gy to subclinical disease] for each fraction of treatment throughout the entire course of radiation, o SIB is commonly used in the conventional [5#/week] and 6#/week accelerated schedule. • SEQ [Sequential] technique typically delivers the initial [lower dose] phase [5 weeks] followed by the high-dose boost volume phase [week 6-7] using 2-3 separate dose plans, and is commonly applied in standard fractionation and hyperfractination. • Concomitant boost accelerated approach utilizes modified SEQ dose plan by delivering the dose to the subclinical targets once a day for 6weeks, and a separate boost dose plan as a second daily fraction for the last 12 treatment days. • Another accelerated approach 6 fractions/week • Altered fractionation may be used for select patients with comorbidities who are not good candidates for 6-7 weeks of adjuvant RT or CTRT.
- 36. PLAN EVALUATION: • Check all contours and OARs • Check the beams used, and the OARs which come in the field • Check for coverage: atleast 95% of volume of PTV should receive 95% of the prescription dose. • Check for Hot spots: hot spot of >105% of prescription dose should not be outside PTV or over OARs. • Check Normal structures constraints on DVH • Check the prescription dose, fractions, dose/#, Monitor unit, energy of photon used.
- 37. ORGAN DOSE ENDPOINT RATE (%) Brainstem Dmax <54Gy Necrosis or cranial neuropathy <5% Spinal cord Dmax <50 Gy Grade >/=2 myelopathy <1% Optic nerve and chiasma Dmax <55Gy Dmean <50Gy Optic neuropathy <3% Retina Dmax <50Gy Blindness <1% Cochlea Dmean <45Gy Hearing loss <15% Single Parotid gland Dmean <20Gy Grade 4 xerostomia <20% B/L Parotid glands Dmean <25Gy Grade 4 xerostomia <20% Mandible Dmax <70Gy Osteoradionecrosis (ORN) <5% Pharyngeal constrictors Dmean 50Gy Dmean <60Gy PEG tube placement Aspiration <5% <5% Brachial plexus Dmax <60Gy Clinically apparent nerve damage <5% Oral cavity Dmean </=40Gy Submandibular gland Dmean <35Gy
- 38. RADIATION DOSE: RT ALONE: PTV High risk: primary tumor and involved lymph nodes Fractionation: • 66Gy [2.2Gy/#] to 70Gy [2Gy/#] • 69.96Gy [2.12Gy/#] Concomitant boost accelerated RT: • 72Gy/1.8Gy/# large field, 1.5Gyboostas a second daily fraction during last 12 treatment days • 66-70Gy/2Gy/#, 6 fractions in a week Hyperfractionation: • 81.6Gy [1.2Gy/#, twice daily] PTV: Low to intermediate risk [sites of suspected subclinical spread] • 44-50Gy [2Gy/#] to 54-63Gy [1.6-1.8Gy/#]
- 39. CONCURRENT CTRT PTV High risk: • 70Gy / 2Gy/# Low to intermediate risk • 44-50Gy [2Gy/#] to 54-63Gy [1.6-1.8Gy/#] • Either IMRT or 3DCRT is recommended technique. POST OPERATIVE RT or CTRT PTV High risk Low to intermediate risk [sites of suspected subclinical spread] • 60-66Gy [2Gy/#] • 44-50Gy [2Gy/#] to 54-63Gy [1.6- 1.8Gy/#] • Either IMRT or 3DCRT is recommended. • Preferred interval between resection and postoperative RT >/= 6weeks
- 40. TRIALS IN HYPOPHARYNX Altered fractionation RT for Locally advanced head and neck cancer RTOG 9003 [Beitler et al] Postop RT vs. CTRT RTOG 9501 & EORTC 22931 [Bernier and Cooper et al] Induction CT f/b CTRT vs. concurrent CTRT alone EORTC 24891, TAX 323, 324 RT + Cetuximab Bonner et al RT vs. CTRT MACH-NC [Benjamin Lacas et al] Induction chemo with PF vs. TPF TAX 324 [Lorch et al]
- 41. TRIALS FOR DEFINITIVE RT ALONE IN EARLY STAGE LESIONS
- 42. METHODS: Stage III or IV [ or stage II base of tongue] SCC, n= 1076 4 arms 1. SFX, 70Gy/35#/7weeks 2. Hyperfractionation, 81.6Gy/68# BID/7weeks 3. Altered fractionation with split, 67.2Gy/42#/6 weeks with 2wk rest after 38.4Gy 4. Altered fractionation continuous, 72Gy/42#/6weeks TRIALS FOR HYPERFRACTIONATION
- 43. RTOG 90-03 Results: at 2years: LRC: significant improvement in 2 yr locoregional control for the hyper fractionation and concomitant boost arms DFS: trend toward improved disease-free survival (p = 0.067 and p = 0.054 respectively for the hyper fractionation and concomitant boost arms OS: difference in overall survival was not significant. TOXICITY: altered fractionation regimens were associated with higher incidence of grade 3 or worse acute mucosal toxicity, but no significant difference in overall toxicity at 2 years following completion of treatment.
- 44. TRIALS FOR CHEMOTHERAPY WITH RT IN ADJUVANT SETTING
- 46. CONCLUSION: • In locally advanced head and neck cancer, microscopically involved section margins and ECE from neck nodes are the most significant prognostic factors for poor outcome as measured either by locoregional recurrence or survival endpoints. • The addition of concomitant cisplatin to postoperative radiotherapy seems to improve the outcome of patients with one or the combination of these two risk factors, whether measured by locoregional control, disease- free/progression-free survival, or overall survival.
- 47. TRIALS FOR INDUCTION CHEMOTHERAPY ROLE EORTC 24891: Lefebvre et al, JNCI, 1996 Lefebvre et al, Ann Oncol, 2012 • For larynx preservation • N=202 • Inclusion criteria: SCC of pyriform sinus or AE fold • Arms: Surgery + adjuvant RT Induction Cis/5-FU followed by RT if complete response or surgery for partial response • Results: local failure is higher with RT Distant metastasis is less with chemo 3-yr and 5-yr larynx preservation is 42% and 35% respectively 5-yr OS 33% and 10-yr OS is 13.5% 10-yr chemoRT survival with functional larynx is 87% 10-yr PFS is 8.5% vs.. 11% 10-yr DM is 36% vs.. 28%
- 48. EORTC TAX 324 TRIALS FOR INDUCTION CHEMOTHERAPY AGENT ROLE
- 49. • Five-year survival in the TPF arm was 52% versus 42% receiving PF, while no increased rates of gastric feeding tubes or tracheostomies were noted between groups.
- 50. CONCLUSION: Concomitant chemoradiotherapy is the mainstay of treatment for locally advanced HNSCC whether as sole treatment or given as adjuvant after surgery, and this analysis confirms, with a much longer follow-up of 9.2 years. The OS benefit of 0.83 [0.79;0.86] with an absolute benefit of 6.5% and 3.6% at 5 and 10 years respectively. • 107 RCTs & 19,805 patients included. • Sixteen new trials (2767 patients) and 2327 deaths (including death from updated previous trials) were added for this update • Subsites: Oral Cavity, Oropharynx, Larynx, Hypopharynx.
- 51. SIDE EFFECTS: ACUTE EFFECTS: LATE EFFECTS: • Major dose-limiting toxicity of RT: Mucositis • Other accompanied symptoms: sore throat, dysphagia, hoarseness • Xerostomia and dysgeusia invariably occur with the standard doses administered. • Weight and nutritional status can be affected due to these acute effects, hence they should be closely monitored. • RT feeding or PEG feeding may be necessary. • Laryngeal edema is usually induced by RT, may persist for upto 6 months after completion of treatment. • Late laryngeal chondronecrosis in the preserved larynx or soft tissue necrosis of the pharyngeal wall [in 2-4% of patients] • Severe laryngeal edema requiring tracheostomy [in 1-6% of patients] • Subcutaneous fibrosis of the soft tissues of the neck [in 11% of patients] • Permanent gastrostomy for inability to swallow becomes necessary [in 2-7% patients treated with RT alone, upto 31% at 2yrs in patients treated with surgery and postoperative irradiation]
- 52. PALLIATIVE RT: Indications for palliative RT: • Advanced cancer setting when curative intent treatment is not appropriate • Medically unsuitable for standard RT or who have widely metastatic disease palliative RT should be considered for relief or prevention of locoregional symptoms if the RT toxicities are acceptable. Recommended RT regimens: • 50Gy in 20# • 37.5Gy in 15# if well tolerated, consider additional 5 fractions to 50Gy • 30Gy/10# • 30Gy/5# 2 fractions/week with >/=3days between the 2 treatments • 44.4Gy in 12# in 3cycles [each cycle give 2 fractions 6hrs apart for 2days in a row, treatment must exclude spinal cord after 2nd cycle] reassessment done at 1-3week intervals.
- 53. MANAGEMENT OF RECURRENCE • After completion of treatment, patients should be followed closely for signs of recurrent or persistent disease. If recurrence is suspected, this should be confirmed by biopsy. • If biopsy is confirmatory Patient should undergo complete restaging to assess the extent of disease. • Recent prospective RTOG studies have demonstrated that reirradiation to the H&N is feasible. • With the advent of highly conformal radiation delivery techniques, selected patients may benefit from reirradiation approaches in conjunction with systemic chemotherapy. • Many patients with recurrent disease, however, are not good candidates for aggressive surgery or salvage radiation therapy and are best served with systemic chemotherapy or best supportive care approaches .
- 54. RE-IRRADIATION: • If the area in consideration overlaps with the previously irradiated volume prior RT should have been >6months from the appearance of new disease. • Before re-irradiation: patient should have PS 0-1 • Better outcomes are seen if the patients received RT previously >2yrs ago, who underwent surgery to remove gross disease prior to reirradiation and who are free of organ dysfunction [eg, laryngectomy, feeding tube]. • Prophylactic treatment of subclinical disease [eg, elective nodal irradiation] is not routinely indicated. • Reirradiation dose: Conventional: postop 56-60Gy[1.8-2Gy/#] definitive66-70Gy [1.8-2Gy/#] • Accelerated fractionation: 60-70Gy [1.2-1.5Gy/#, BID]
Editor's Notes
- ADH1B : Alcohol dehydrogenase 1B ALDH2: Aldehyde dehydrogenase 2 ADH1B is one of several genes that encode the alcohol dehydrogenase (ADH) enzymes, which regulate oxidation of ethanol to acetaldehyde (Edenberg, 2007). ALDH2 encodes the mitochondrial aldehyde dehydrogenase (ALDH) enzyme, the principal catalyst for oxidation of acetaldehyde during alcohol metabolism.
- Submucosal spread 60% of hypopharynx cancers demonstrate subclinical spread with a range of 10mm superiorly, 25mm medially, 20mm laterally and 20mm inferiorly.
- Role of surgeon in carcinoma hypopharynx who undergo non-operative treatment approaches are: To perform: endoscopic biopsy detailed assessment of tumor extent methods to secure the airway [tracheostomy or laser debulking] methods to ensure adequate nutrition [gastrostomy] multidisciplinary oncologic follow-up after non-operative treatment