1. • Inclusion criteria: Patient admitted to the inpatient family medicine service
greater than 18 years of age between September 15, 2015 and March 15,
2016.
• Patients with planned follow-up by a physician in the Family Care Center
were selected to receive a phone call from a pharmacist within 2-7 days of
discharge.
• Patients with no planned follow-up in the Family Care Center did not
receive a phone call from a pharmacist post discharge.
• Interventions and documentation were messaged to the primary care
physician via electronic medical record on the day of the phone call.
• If a patient required urgent resolution to a perceived medication-related
concern, the on-call family medicine resident was notified.
• A physician questionnaire was administered at the midpoint and
conclusion of the project to determine pilot impact.
Value of including a pharmacist in the transitions of care team; A
pilot study involving family medicine patients at NorthShore
LITERATURE REVIEW
OBJECTIVE
RESULTS CASE STUDIES
DISCUSSION
REFERENCES
• A recent study by Rozich and colleagues suggests up to 60% of all medication
errors occur during the discharge process.1
• Forster and colleagues found nearly 20% of discharged patients experienced
an error within three weeks of an inpatient stay.2
• Transitions of care programs may benefit both patients and practitioners by
reducing readmissions and associated costs.3-5
• Methods explored in the literature for reducing medication errors at
discharge include pharmacist-driven or nursing-driven counseling and
performing post discharge follow up calls.3-6
• By contacting patients after hospital discharge as part of a structured
protocol, the pharmacist may be able to reduce the time required for a
patient to obtain access to a medication and potentially prevent
readmissions.3
Disclosure
This medicationuse evaluationwas exempt from InstitutionalReview Board review since the results will be used as a quality improvementmeasure.
Authors of this presentation have the followingto disclose concerning possible financialor personal relationships with commercialentities that may have a direct or indirect interest in the subject matter of this
presentation:
Steven Asbill, PharmD: Nothing to disclose. Heather Minger, PharmD, BCPS: Nothing to disclose. Min Song, PharmD, BCPS: Nothing to disclose. Lauren Oshman, MD, MPH, FAAP: Nothing to disclose. Tina Zook,
PharmD: Nothing to disclose.
• To determine if a pharmacist’s involvement in the transitions of care process
via telephonic intervention post discharge will improve medication errors,
side effects, readmission, and emergency department (ED) visit rates.
Table 1: Physician satisfaction questionnaire responses
• Prior authorizations are an important consideration for both pharmacists
and physicians when prescribing new medications, as these have the
potential to delay patients’ therapy.
• Interventions may have prevented or delayed emergency department visits
and readmissions, potentially resulting in substantial cost savings for the
institution.
• Based on questionnaire data as well as interventions, methods to sustain
project currently being discussed.
• Pilot may provide framework for interdisciplinary patient care, as patient care
concerns were resolved due to a group effort.
• Potential expansion of this pilot may enhance the patient’s ability to
advocate for health concerns and medication needs.
• An effective transitions of care program may prevent medication related
adverse events at the point of discharge or quickly thereafter.
Limitations
• As this was a pilot program with a number of new procedures, discharges
may have been missed due to the pharmacy resident’s schedule as well as
weekend and holiday exclusions.
• Narrow window for daily discharge follow up calls due to resource limitation.
1. Rozich JD and Resar RK. Medicationsafety: One organization’sapproach to the challenge. Journal of ClinicalOutcomes Management 2001;8:27-34
2. Forster AJ, Murff H, Peterson JF, et al. The incidence and severity of adverse events affectingpatients after discharge from the hospital. Ann Intern Med 2003;138:161-162
3. Sanchez GM, Douglass MA, and Mancuso MA. Revisiting Project Re-EngineeredDischarge (RED): The impact of a pharmacist telephone interventionon hospital readmission rates. Pharmacotherapy2015;35(9):805-
812
4. GillespieU, Alassaad A, Henrohn D, et al. A comprehensive pharmacist interventionstrategy to reduce morbidityin patients 80 years or older, Arch Intern Med 2009;169(9):894-900.
5. KilcupM, Schultz D, Carlson J, and Wilson B, Postdischarge pharmacist medicationreconciliation:Impact on readmission rates and financialsavings. J Am Pharm Assoc 2013;53:78-84.
6. Kwan JL, Lo L, Sampson M and Shojania KG. Medicationreconciliationduring transitions of care as a patient safety strategy. Ann Intern Med 2013;158:397-403
Steven Asbill PharmD, Heather Minger PharmD, BCPS, Min Song PharmD, BCPS, Dr. Lauren Oshman MD, MPH, FAAP, Tina Zook PharmD
NorthShore University HealthSystem, Glenview, IL
RESULTS
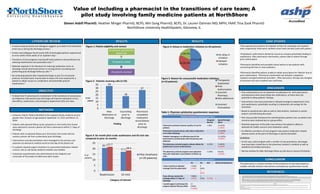
Figure 1: Patient eligibility and contact
40 patients qualified for
phone call
35 patients called
29 patients reached
33
18
27
0
5
10
15
20
25
30
35
New
Medication at
discharge
Counseling
prior to
discharge
Pharmacist
completed
medication
reconciliation
prior to
discharge
Figure 2: Patients receiving calls (n=35)
#of
patients
METHODS
Finding
17 (51.5%)
10 (30.3%)
6 (18.2%) No delay in
initiation
Delayed
initiation
Figure 4: Delays in medication initiation (n=33 patients)
2
2
2
1
1
1
1
Figure 5: Reason for unsuccessful medication initiation
(n=10 patients)
Therapeutic
Duplication
Prior
Authorization
Incorrect
Pharmacy
Non-adherence
Incorrect
Formulation
Physician Satisfaction Questionnaire Part 1
Disagree/
Neutral
Agree/Strongly
Agree
Pharmacist outreach improves quality of care for
patients
1 (8%) 12 (92%)
5 (100%)
Pharmacist outreach phone calls reduce medication
errors after discharge
- 13 (100%)
5 (100%)
Inbasket messaging is an effective way for the
pharmacist to communicate with the primary care
physician
- 13 (100%)
5 (100%)
The pharmacy outreach program reduces delays for
patients due to prior authorizations
2 (15%) 11 (85%)
5 (100%)
The pharmacy outreach program saves physician
time with medication reconciliation at follow up
visits
5 (39%) 8 (61%)
5 (100%)
Figure 3: Six month pilot crude readmission and ED visit rate
compared to prior six months
20.7
17.2
21.7
18.4
0
5
10
15
20
25
Readmission ED Visit
Pilot timeframe
(n=29 patients) Physician Satisfaction Questionnaire Part 2
Yes No N/A Abstained Responses
I have received an Inbasket
message from the pharmacist
7 (54%)
2 (40%)
6
(46%)
3
(60%)
-
If yes, did you receive the
message within 2-7 days of
discharge
7 (88%)
1 (25%)
1
(12%)
-
3 (75%) 1
I would support continuing this
program beyond February 2016
13
(100%)
5 (100%)
- -
*Black=midpoint responses (n=13) **Red=final responses (n=5)
•Two separate prescriptions for labetalol written by cardiology and inpatient
team respectively. Pharmacist clarified correct dose and discussed with patient.
•Prophylactic azithromycin denied by insurance company potentially leading to
readmission. After pharmacist intervention, patient able to obtain through
prior authorization.
•Pharmacist identified and provided clinical advice to two patients with
concerning diarrhea on new antibiotics.
•Pharmacist identified patient unable to obtain prescription for rifaximin due to
prior authorization. Pharmacist coordinated care between outpatient,
inpatient and gastrointestinal providers . After discussion, therapy was changed
to lactulose and cost to patient was confirmed.
The pharmacist is a valued member of the transitions of care team based on
notable clinically relevant interventions and physician questionnaire results.
% of
patients
Category of Interest